Survey
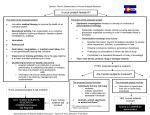
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Journal of Medical Microbiology (2013), 62, 1673–1679 DOI 10.1099/jmm.0.064758-0 Molecular diagnosis of bloodstream infections with a new dual-priming oligonucleotide-based multiplex PCR assay Lucrecia Carrara,1,2 Ferran Navarro,1,2 Miquel Turbau,2,3 Montse Seres,2,3 Indalecio Morán,2,4 Isabel Quintana,2,4 Rodrigo Martino,2,5 Yesica González,1,2 Albert Brell,1,2 Oscar Cordon,1,2 Karol Diestra,1,2 Caterina Mata,1,2 Beatriz Mirelis1,2 and Pere Coll1,2 Correspondence 1 Ferran Navarro 2 Servicio de Microbiologı́a, Hospital de la Santa Creu i Sant Pau, 08025 Barcelona, Spain Biomedical Research Institute Sant Pau (IIB Sant Pau), Sant Antoni Ma Claret 167, 08025 Barcelona, Spain [email protected] 3 Servicio de Urgencias Generales, Hospital de la Santa Creu i Sant Pau, 08025 Barcelona, Spain 4 Servicio de Medicina Intensiva, Hospital de la Santa Creu i Sant Pau, 08025 Barcelona, Spain 5 Servicio de Hematologı́a, Hospital de la Santa Creu i Sant Pau, 08025 Barcelona, Spain Received 25 June 2013 Accepted 4 August 2013 Mortality from bloodstream infections (BSIs) correlates with diagnostic delay and the use of inappropriate empirical treatment. Early PCR-based diagnosis could decrease inappropriate treatment, improving patient outcome. The aim of the present study was to assess the clinical utility of this molecular technology to diagnose BSIs. We assessed a new dual-priming oligonucleotide-based multiplex PCR assay, the Magicplex Sepsis Test (MST) (Seegene), along with blood culture (BC). A total of 267 patients from the intensive care unit and haematology and emergency departments were enrolled. Clinical data were also used by physicians to determine the likelihood of infection. Ninety-eight (37 %) specimens were positive: 29 (11 %) by both the MST and BC, 29 (11 %) by the MST only, and 40 (15 %) by BC only. The proportion of agreement between the two methods was 73 % (Cohen’s k: 0.45; 0.28–0.6; indicating fair to moderate agreement). According to clinical assessment, 63 (64 %) positive specimens were considered BSIs: 23 (36 %) were positive by both the MST and BC, 22 (35 %) were positive only by BC, and 18 (29 %) were positive only by the MST. Thirty-eight (14 %) positive specimens by the MST and/ or BC were considered as contaminants. Of 101 specimens collected from patients receiving antibiotics, 20 (20 %) were positive by the MST and 32 (32 %) by BC. Sensitivity and specificity were 65 % and 92 %, respectively, for the MST and 71 % and 88 %, respectively for BC. We concluded that the MST shows a high specificity but changes in design are needed to increase bacteraemia detection. For viability in clinical laboratories, technical improvements are also required to further automate the process. INTRODUCTION Bloodstream infection (BSI) is a serious condition that causes around 215 000 deaths per year in the USA and 135 000 in Europe (Bassetti et al., 2012; Mancini et al., 2010; Wolk & Fiorello, 2010a). A significant cause of this high mortality is the delay in microbiological diagnosis Abbreviations: BC, blood culture; BSI, bloodstream infection; CoNS, coagulase-negative Staphylococcus; DPO, dual-priming oligonucleotide; MST, Magicplex Sepsis Test; READ, real amplicon detection; TTP, time to positivity. Supplementary material is available with the online version of this paper. 064758 G 2013 SGM (Mancini et al., 2010; Schaub et al., 2011; Wolk & Fiorello, 2010b). Standard diagnosis, i.e. blood culture (BC), takes up to 5 days – a time lapse that forces physicians to use empirical antibiotic treatment. Kumar et al. (2006) showed that mortality from BSI increases about 7–8 % per hour of delay in effective antimicrobial administration within the first hour of documented hypotension in adult patients with septic shock. In parallel, several studies have shown that the earlier specific treatment is established, the better the outcome of patients (Dellinger et al., 2008; Rivers et al., 2012). All these studies suggest that diagnostic methods should be Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Thu, 04 May 2017 03:44:02 Printed in Great Britain 1673 L. Carrara and others improved (Mancini et al., 2010; Paolucci et al., 2010; Schaub et al., 2011; Wolk & Fiorello, 2010b). The key to improving management of BSI is to reduce the time taken to obtain microbiological results. The concept of theranostics could be introduced into the medical management of BSI. Theranostics in infectious diseases implies using rapid and accurate diagnostic assays to enable better initial management of patients and more efficient use of antimicrobials (Picard & Bergeron, 2002). Multiplex PCR assays are promising approaches that aim to reduce aetiological diagnosis of BSI to hours (Paolucci et al., 2010; Reinhart et al., 2012), avoiding the need for culture-based microbiological methods. Several molecular assays (PCR/ES-MS, SeptiTest, SeptiFast, Vyoo/Looxter) shorten the time of detection of many micro-organisms to 6–8 h, but some of them do not detect drug resistance genes (Bloos et al., 2012; Ecker et al., 2010; Fitting et al., 2012; Lucignano et al., 2011; Tsalik et al., 2010; Wallet et al., 2010; Wellinghausen et al., 2009). To date, neither BC nor molecular approaches are as powerful as we would like (Baron, 2006). A new commercial kit, the Magicplex Sepsis Test (MST; Seegene) appeared on the market in July 2010. The MST was designed to detect most pathogenic micro-organisms responsible for BSIs as well as three key drug resistance genes, mecA, vanA and vanB, within 6 h. The assay uses a selective human cell lysis pre-treatment of specimens to increase detection of bacterial nucleic acids. A dualpriming oligonucleotide (DPO) is then used for amplification. DPO consists of two functional priming regions separated by a poly(I) linker. It generates dual-priming regions, resulting in only target-specific products (Chun et al., 2007). Moreover, DPO primers are labelled with a fluorescence marker, which allows early detection of fluorescence signals [READ (real amplicon detection) technology] and gives quicker results. The aim of the present study was to assess the clinical utility of this new technology to diagnose BSIs. METHODS This prospective study was performed at Hospital de la Santa Creu i Sant Pau – a tertiary university hospital in Barcelona. Patients were recruited between April 2011 and September 2011 from the intensive care unit (ICU) and haematology and emergency departments. Demographic data of patients, clinical and laboratory findings, cultures of suspected source of infection, and administration of antimicrobial therapy were recorded prospectively to determine patients’ infection status. One blood specimen per patient and episode was selected for the MST on the basis of suspected sepsis. Blood samples were selected regardless of previous antibiotic treatment. Patients younger than 18 years were excluded from the study. During weekends, samples for the molecular approach were not processed and they were therefore excluded from the study. The study was approved by the Ethics Committee at Hospital de la Santa Creu i Sant Pau (study no. 11BSP-MOL-2011-62). BC processing. Blood specimens were collected by direct venipunc- ture. In 11 cases, venipuncture was not available for sampling and 1674 specimens were obtained from catheters. About 10–20 ml of blood was inoculated in each BC bottle (aerobic and anaerobic culture) and incubated as soon as possible at 35 uC in BacT/Alert (bioMérieux) BC cabinets for 7 days. When growth in BC bottles was automatically detected, Gram stain and subcultures were performed, and isolates were identified according to standard laboratory methods (Baron, 2005). Antibiotic susceptibility was determined using accredited routine laboratory methods (CLSI, 2012). Genotypic identification by 16S rDNA sequencing was required in two anaerobe isolates and was performed as previously described (http://rdna4.ridom.de/static/ primer.html; Esparcia et al., 2011; Petti, 2007). MST processing. An aliquot of 1 ml of fresh whole blood was required for the MST test, according to the manufacturer’s instructions. The paired samples used for BC and the MST derived from the same venipuncture or catheter draw. Specimens were transported in EDTA tubes to the laboratory and stored at 2–8 uC until processing. Specimens were discarded if the MST was not performed within 24 h. Microbial nucleic acids were enriched by performing a pre-treatment with a Blood Pathogen kit (Seegene) according to the manufacturer’s instructions. This kit allows selective human cell lysis and degradation of the released (human and nonhuman) DNA by a DNase. Intact microbial cells (viable and nonviable) were then concentrated from the lysed blood (Wellinghausen et al., 2009). Microbial nucleic acids were automatically extracted by the SEEPREP12 purification system (Seegene) according to the manufacturer’s instructions. The extraction procedure took approximately 2.5 h. Nucleic acids were amplified using a conventional PCR thermocycler (System 9700; Applied Biosystems) in two independent reaction tubes: one for Gram-negative bacteria and fungi, and another for Gram-positive bacteria and three drug resistance markers: mecA, vanA and vanB. This initial amplification process took approximately 2.5 h (Fig. 1a). Amplicon specimens were then detected, screened and identified using SmartCycler II real-time PCR (Cepheid). Screening and identification steps were performed separately. For the screening step, three real-time PCRs were performed (approximately 30 min): one for Gram-positive bacteria, one for drug resistance markers, and one for Gram-negative bacteria and fungal pathogens (Fig. 1b). If amplification occurred, the pathogen was identified using suitable identification probes (Fig. 1c), taking an additional 30 min. Amplicons were detected by fluorescent nucleotide probes and results were analysed by Seegene VIEWER real-time PCR software. An internal control was used in all amplification steps. For the staphylococcal amplification probe, a Ct of ,10 cycles was needed to determine positivity according to the manufacturer’s instructions. For the other probes, Ct had to be ,15 cycles. To minimize contamination, DNA extraction and amplification/detection were performed in separate rooms. The MST was performed by specially trained laboratory technicians that had been working with molecular techniques (both manual and automatic) for many years. Analyses of microbiological results. To determine whether the micro-organisms corresponded to a true pathogen, we used recommended microbiological criteria as previously described (Weinstein & Doern, 2011). Accordingly, the following data were taken into consideration: identification and antimicrobial resistance pattern of micro-organisms, and clinical findings in the patient (e.g. fever, leukocytosis, imaging studies). Possible contaminant micro-organisms detected only by the MST were considered true pathogens when clinical data and additional clinical cultures supported this consideration. It should be pointed out that antibiotic susceptibility patterns cannot be used with the MST to compare isolates from different specimens. Clinicians were not informed about the MST results until the end of the study. These results did not therefore influence the medical management of patients. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Thu, 04 May 2017 03:44:02 Journal of Medical Microbiology 62 Molecular diagnosis of sepsis (a) Amplification Amplicon Bank 1. Gram-positive bacteria/drug resistance 73 Gram-positive bacteria, three drug resistance markers Amplicon Bank 2. Gram-negative bacteria/fungi 12 Gram-negative bacteria, six fungi (b) (c) Screening Gram-positive bacteria screening Streptococcus spp. Enterococcus spp. Staphylococcus spp. Drug resistance screening vanA vanB mecA Gram-negative bacteria/fungal screening Gram-negative bacteria-A Gram-negative bacteria-B Fungi Identification Enterococcus spp. ID 1. Streptococcus spp. E. faecalis S. agalactiae S. pyogenes E. gallinarum S. pneumoniae E. faecium ID 3. Staphylococcus spp. S. epidermidis S. haemolyticus S. aureus ID 4. Gram-negative bacteria-A ID 5. Gram-negative bacteria-A Pseudomonas aeruginosa Serratia marcescens Acinetobacter baumannii Bacteroides fragilis Stenotrophomonas maltophilia Salmonella typhi ID 6. Gram-negative bacteria-B ID 7. Gram-negative bacteria-B Klebsiella pneumoniae Escherichia coli Klebsiella oxytoca Enterobacter cloacae Proteus mirabilis Enterobacter aerogenes ID 8. Fungi ID 9. Fungi Candida albicans Candida glabrata Candida tropicalis Candida krusei Aspergillus fumigatus Candida parapsilosis Fig. 1. Amplification (a), screening (b) and identification (c) panels of the MST. Vassar Stats website (http://vassarstats.net/). In all cases, the 95 % confidence intervals are shown. Cohen’s k values of 0.41–0.60 are considered of moderate agreement and values of 0.21–0.40 are considered of fair agreement. In total, 101 of 267 specimens were collected from patients receiving antibiotic treatment: 20 specimens (20 %; 13– 29 %) were positive by the MST and 32 specimens (32 %; 23–41 %) were positive by BC. Six specimens (6 %; 2– 13 %) were positive only by the MST. RESULTS Results of the MST and BC according to clinical assessment (Table 2) Statistical analyses. Statistical analyses were performed using the From the 267 paired MST and BC set specimens, 142 came from the emergency department, 99 from ICU areas and 26 from the haematology department. Specimens were collected by venipuncture in 256 cases and by catheter in 11 cases. Global results of the MST and BC (Table 1) Ninety-eight of 267 (37 %; 31–43 %) specimens were positive: 29 (11 %; 8–15 %) by both the MST and BC, 29 (11 %; 8– 15 %) by the MST only, and 40 (15 %; 11–20 %) by BC only. The percentage of agreement between the two methods was 73 % (Cohen’s k: 0.45; 0.28–0.6; indicating fair to moderate agreement). Thirty-eight of 98 (14 % of 267; 11–19 %) positive specimens were considered as contaminants: three (1 %; 0.4– 3 %) by both the MST and BC, 14 (5 %; 3–9 %) by the MST only, and 21 (8 %; 5–12 %) by BC only. In specimens considered as contaminant, time to positivity (TTP) for BC was 31 h (20–72 h) and the Ct of the MST was .13. http://jmm.sgmjournals.org Sixty-three of 98 (64 %; 54–73 %) positive specimens (by the MST and/or BC) were considered BSIs. Global sensitivity and specificity of the MST for BSI detection were 65 % (52–76 %) and 92 % (87–95 %), respectively, whereas for BC they were 71 % (58–82 %) and 88 % (83– 92 %), respectively. In specimens considered as BSIs, TTP for BC was 15 h (8–39 h) and the Ct of the MST was ,13. Among specimens obtained from catheters, only three were positive by the MST (two S. epidermidis and one K. pneumoniae). Both S. epidermidis specimens were considered true bacteraemia according to other specimens (including the paired BC) and clinical data. MST-positive specimens. Forty-one of the 58 MST- positive specimens were considered as BSIs: 23 (36 %; 25– 50 %) specimens were positive by both the MST and BC (MST-positive/BC-positive) and 18 (29 %; 18–42 %) Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Thu, 04 May 2017 03:44:02 1675 L. Carrara and others Table 1. Global results of the MST and BC Result MST-positive MST-negative Total BC-positive BC-negative Total 29*Dd§ 40 69 29|| 169 198 58 209 267 *BC detected two additional Bacteroides fragilis and coagulasenegative Staphylococcus (CoNS) in two different specimens. DMST detected two additional Staphylococcus epidermidis and Streptococcus agalactiae in two different specimens. dIn three specimens the MST was positive for: Klebsiella pneumoniae in two cases and for Pseudomonas aeruginosa in the other while CoNS isolated by BC were considered as contaminants. §Three positive specimens by both the MST and BC were considered as contaminants. ||Ten were Escherichia coli (two by polymicrobial detection: K. pneumoniae and E. coli), two K. pneumoniae, two Streptococcus pneumoniae, one Enterobacter cloacae. The remaining specimens were considered as contaminants. Six were E. coli, three CoNS, two P. aeruginosa, two by polymicrobial detection: P. aeruginosa and CoNS, one Klebsiella oxytoca, one K. pneumoniae, one S. pneumoniae, two Streptococcus dysgalactiae subsp. equisimilis, one Atopobium rimae, one Bacillus spp., one Corynebacterium spp., one Odoribacter splanchnicus (see supplementary material available with the online version of this paper). The remaining positive specimens were considered as contaminants. specimens were positive only by the MST (MST-positive/ BC-negative). Among these specimens, 13 (88.9 %; 67.2– 96.9 %) were MST-positive for Enterobacteriaceae (two of these samples were positive for both K. pneumonia and E. coli). Seven specimens were collected from patients under antibiotic treatment (Tables 1, 2 and 3). BC-positive specimens. Forty-five of 69 BC positive specimens were considered as BSIs: 22 (35 %; 24–48 %) specimens were positive only by BC (MST-negative/BCpositive). Four specimens were positive for P. aeruginosa; MST amplification was performed on the isolates, giving a positive result for P. aeruginosa. The MST was inhibited in one specimen that was BC-positive for Staphylococcus haemolyticus. In four specimens, BCs were positive by species not included in MST detection and identification panels. The remaining 13 specimens are detailed in Tables 1, 2 and 3. We found no statistical significance between the number of pathogens detected by the two methods (63) and the number of pathogens (45) detected by BC alone (P.0.05). Regarding drug resistance markers, 10 meticillin-resistant staphylococci were detected by antibiotic susceptibility test (eight CoNS and two S. aureus). The MST detected the mecA gene in four of these specimens (three CoNS and one S. aureus). In the remaining six specimens, three MSTs were negative, two MSTs were positive only for Staphylococcus spp. and failed to detect both the species 1676 and mecA gene, and one MST was inhibited (no Ct detected for internal control). The Ct of the identification probe of one of the meticillin-resistant S. aureus was 10.02. As the Ct for Staphylococcus spp. is 10, the software scored this specimen as negative. In two specimens, the MST detected the mecA gene but failed to detect any organism. Vancomycin-resistant enterococci were not detected in the present study either by the MST or by the antibiotic susceptibility test. DISCUSSION This is the first study to assess the clinical performance of the multiplex PCR assay, the Magicplex Sepsis Test. We found that sensitivity for the MST (65 %) was not higher than for BC (71 %) but was comparable to the rates found in similar studies (52–87 %) using other commercial kits (Bloos et al., 2012; Fitting et al., 2012; Tsalik et al., 2010; Wallet et al., 2010). However, a remarkable proportion (37 %) of Enterobacteriaceae spp. was detected by the MST but not by BC. BC detected a higher number of P. aeruginosa isolates than the MST (four of five). Only one of 267 MST amplifications was inhibited. The proportion of agreement between the MST and BC was 73 %, mostly due to negative results. The ability of the MST to detect whole cells, viable or not, should increase the number of positive specimens processed under the antimicrobial effect. Unexpectedly, the number of positive specimens processed under the antimicrobial effect was not higher by the MST than by BC. The most striking finding was the discrepancy between positive MST and BC results. We detected more discrepant results than in previous studies (Bloos et al., 2012; Tsalik et al., 2010; Wallet et al., 2010). Explanations suggested for PCR-negative/BC-positive results are genetic variability or mutations of the target site, inhibition of PCR and low microbial load (Bloos et al., 2012; Esparcia et al., 2011; Wellinghausen et al., 2009). Our current findings do not fully confirm earlier works. Mutations of the target alteration were excluded for P. aeruginosa because MST amplification performed in the isolates was positive. Only one MST amplification was inhibited (1/267; 0.4 %). The bacterial load was indirectly measured by the TTP. The mean TTP for all MST-positive/ BC-positive results was 15 h. Nevertheless, the mean TTP for all MST-negative/BC-positive results was 19 h. Accordingly, the hypothesis of a low bacterial load can be ruled out. In this study, the blood volume used for the MST was smaller than in other studies (Bloos et al., 2012; Fitting et al., 2012; Tsalik et al., 2010; Wallet et al., 2010). The significant difference in the sample volumes used for the MST and BC testing is likely a major contributing factor to the poor sensitivity of PCR. Hansen et al. (2009) evaluated different pre-analysis sample treatments together with various DNA extraction kits for the selective isolation of bacterial DNA from whole blood. They concluded that the combination of performing a pre-analysis sample Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Thu, 04 May 2017 03:44:02 Journal of Medical Microbiology 62 Molecular diagnosis of sepsis Table 2. Results of the MST and BC compared to clinical criteria Results BSI BSI MST Positive Negative Total BC Positive Negative Total Not BSI Total 41 22 63 17* 187 204 58 209 267 45 18 63 24* 180 204 69 198 267 MST values: sensitivity 65 % (52–76 %), specificity 92 % (87–95 %), positive predictive value 71 % (57–82 %), negative predictive value 89 % (84–93 %), Cohen’s unweighted k50.45. BC values: sensitivity 71 % (58–82 %), specificity 88 % (83–92 %), positive predictive value 68 % (55 279 %), negative predictive value 91 % (86–94 %), Cohen’s unweighted k50.45. *Non-proven BSIs with positive specimens either by BC or the MST were considered as contaminated specimens. treatment and using a larger sample volume increased the bacterial detection limit (Hansen et al., 2009). Accordingly, in our molecular approach, the volume of blood requested should probably be increased to improve sensitivity. A possible explanation for the PCR-positive/BC-negative results could be the use of antimicrobial agents before blood extraction (Wellinghausen et al., 2009). These agents affect the viability of micro-organisms, diminishing the ability of BC to detect bacteraemia. Nevertheless, there were no significant differences between percentages of positivity by BC and the MST (32 % and 20 %, respectively) in the specimens collected from patients receiving antibiotic treatment. These results do not support the notion that micro-organisms detected by PCR may have been nonviable and thus non-detectable by BC (Hansen et al., 2009; Wellinghausen et al., 2009). Moreover, to give PCR-positive/ BC-negative results could be misleading to the clinician and cause an unnecessary change in antimicrobial therapy. These discrepancies could be explained by an unmeasured combination of bacterial load, bacterial viability and decreased antimicrobial concentration in BC. The MST failed to detect five staphylococcal BSIs (one S. aureus). The manufacturer has proposed a cut-off of 10 to diminish the number of Staphylococcus spp. falsepositive results. However, some bacteraemia caused by Staphylococcus spp. could be missed (one in our series). A Ct cut-off of 15 as for the other micro-organisms could be better to detect staphylococcal BSIs. Despite its low sensitivity (65 %), we would like to emphasize that the MST is a reliable tool to detect bacteraemia, particularly those produced by Enterobacteriaceae. A DPO design, along with the pre-treatment of samples, reduced both false-negative and false-positive results (Kommedal et al., 2012). The MST could therefore be useful and reliable for the selection of an antibiotic, even in those meticillinresistant Staphylococcus in which the MST detected a mecA Table 3. Total micro-organisms detected by the MST and BC Species Enterobacter cloacae Enterococcus faecalis Escherichia coli Klebsiella oxytoca Klebsiella pneumoniae Pseudomonas aeruginosa Proteus mirabilis CoNS Streptococcus pneumoniae Staphylococcus aureus oxaS Staphylococcus aureus oxaR Streptococcus dysgalactiae Streptococcus viridans Bacillus spp. Corynebacterium spp. Anaerobe Candida spp. Totally detected Detected by the MST Detected by BC MST control BC control 2 2 20 1 11 5 1 44 4 3 2 3 1 1 4 4 1 2 1* 13 0 10 1 1 21 3 3 1 1D 0 0 0 0 0 0 2 10 1 5 4 1 30 2 3 2 3 1 1 4 4 1 – 0 0 0 0 0 0 16 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 20 0 0 0 0 1 1 3 0 0 Coincidence (%) 0/2 1/2 4/20 0/1 4/11 0/5 1/1 7/44 1/4 3/3 1/2 1/3 0/1 0/1 0/4 0/4 0/1 (0) (50) (20) (0) (36) (0) (100) (16) (25) (100) (50) (30) (0) (0) (0) (0) (0) *MST detected Enterococcus sp. DMST detected Streptococcus sp. http://jmm.sgmjournals.org Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Thu, 04 May 2017 03:44:02 1677 L. Carrara and others resistance gene. This should make the MST a practical kit for clinical laboratories. The MST is also a reliable tool to detect bacteraemia within 6 h. Its DPO design makes it an attractive primer set in this setting, where false-negative and false-positive PCRs can be reduced by preventing human DNA cross-reactivity (Kommedal et al., 2012). We emphasize here that the MST allowed us to detect Enterobacteriaceae that were not detected in BC. Some important technological features could be improved, however. In our experience, the MST technology is hard to use as a diagnostic tool in clinical microbiology laboratories that provide service 24/7. The whole process requires four manual steps of manipulation: pre-treatment of specimens, extraction of DNA, screening amplification and amplification to identify the micro-organism. The use of the conventional PCR is a handicap for the MST because of potential contamination of PCR reagents by amplicons. Technological features should thus be modified accordingly. We suggest increasing the volume of the specimens for the MST and homogenizing the cut-off for all micro-organisms, including Staphylococcus. Both these changes would help to increase the detection of bacteraemia. Finally, the whole procedure of the MST should be automated, as this would facilitate the integration of the MST in microbiology laboratories. A positive point of the MST is its ability to detect resistance genes such as mecA and van. Nevertheless, in our experience, the MST failed to detect six out of 10 meticillin-resistant genes. Moreover, the detection of additional resistance genes such as those involved in carbapenem resistance, e.g. blaKPC , blaVIM, blaIMP, and blaOXA-48, would be beneficial. This point is particularly relevant for countries where carbapenem resistance is even more frequent than vancomycin resistance. The MST could therefore be useful for the selection of an antibiotic within the first hours of BSI. In conclusion, the MST shows high specificity but its rate of positivity is similar to that of BC. Changes in design are needed to increase bacteraemia detection and technical improvements are needed to further automate the process for viability in clinical laboratories. Baron, E. J. (editor) (2005). Cumitech 1 C: Blood Cultures IV. Washington, DC: American Society for Microbiology. Baron, E. J. (2006). Implications of new technology for infectious diseases practice. Clin Infect Dis 43, 1318–1323. Bassetti, M., Trecarichi, E. M., Mesini, A., Spanu, T., Giacobbe, D. R., Rossi, M., Shenone, E., Pascale, G. D., Molinari, M. P. & other authors (2012). Risk factors and mortality of healthcare-associated and community-acquired Staphylococcus aureus bacteraemia. Clin Microbiol Infect 18, 862–869. Bloos, F., Sachse, S., Kortgen, A., Pletz, M. W., Lehmann, M., Straube, E., Riedemann, N. C., Reinhart, K. & Bauer, M. (2012). Evaluation of a polymerase chain reaction assay for pathogen detection in septic patients under routine condition: an observational study. PLoS ONE 7, e46003. Chun, J. Y., Kim, K. J., Hwang, I. T., Kim, Y. J., Lee, D. H., Lee, I. K. & Kim, J. K. (2007). Dual priming oligonucleotide system for the multiplex detection of respiratory viruses and SNP genotyping of CYP2C19 gene. Nucleic Acids Res 35, e40. CLSI (2012). Performance Standards for Antimicrobial Susceptibility Testing; 22nd International Supplement M100–S22. Wayne, PA: Clinical and Laboratory Standards Institute. Dellinger, R. P., Levy, M. M., Carlet, J. M., Bion, J., Parker, M. M., Jaeschke, R., Reinhart, K., Angus, D. C., Brun-Buisson, C. & other authors (2008). Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med 36, 296–327. Ecker, D. J., Sampath, R., Li, H., Massire, C., Matthews, H. E., Toleno, D., Hall, T. A., Blyn, L. B., Eshoo, M. W. & other authors (2010). New technology for rapid molecular diagnosis of bloodstream infections. Expert Rev Mol Diagn 10, 399–415. Esparcia, O., Montemayor, M., Ginovart, G., Pomar, V., Soriano, G., Pericas, R., Gurgui, M., Sulleiro, E., Prats, G. & other authors (2011). Diagnostic accuracy of a 16S ribosomal DNA gene-based molecular technique (RT-PCR, microarray, and sequencing) for bacterial meningitis, early-onset neonatal sepsis, and spontaneous bacterial peritonitis. Diagn Microbiol Infect Dis 69, 153–160. Fitting, C., Parlato, M., Adib-Conquy, M., Memain, N., Philippart, F., Misset, B., Monchi, M., Cavaillon, J. M. & Adrie, C. (2012). DNAemia detection by multiplex PCR and biomarkers for infection in systemic inflammatory response syndrome patients. PLoS ONE 7, e38916. Hansen, W. L., Bruggeman, C. A. & Wolffs, P. F. (2009). Evaluation of new preanalysis sample treatment tools and DNA isolation protocols to improve bacterial pathogen detection in whole blood. J Clin Microbiol 47, 2629–2631. Kommedal, O., Simmon, K., Karaca, D., Langeland, N. & Wiker, H. G. (2012). Dual priming oligonucleotides for broad-range amplification of the bacterial 16S rRNA gene directly from human clinical specimens. J Clin Microbiol 50, 1289–1294. Kumar, A., Roberts, D., Wood, K. E., Light, B., Parrillo, J. E., Sharma, S., Suppes, R., Feinstein, D., Zanotti, S. & other authors (2006). ACKNOWLEDGEMENTS This study was partially supported by the Ministy of Health and Consumer Affairs, Instituto de Salud Carlos III-FEDER, Spanish Network for Research in Infectious Diseases (REIPI/RD06/0008/ 0013). We thank the IZASA-Werfen Group for providing diagnostic kits and C. Newey for revising the English. All authors except K. D. and C. M. declare that they have no conflict of interest. Both K. D. and C. M. are now working with the IZASA-Werfen Group. Results of this study were presented at the XVI Congress of the Spanish Society of Microbiology and Infectious Diseases, 9–11 May 2012, Bilbao, Spain. 1678 REFERENCES Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 34, 1589–1596. Lucignano, B., Ranno, S., Liesenfeld, O., Pizzorno, B., Putignani, L., Bernaschi, P. & Menichella, D. (2011). Multiplex PCR allows rapid and accurate diagnosis of bloodstream infections in newborns and children with suspected sepsis. J Clin Microbiol 49, 2252–2258. Mancini, N., Carletti, S., Ghidoli, N., Cichero, P., Burioni, R. & Clementi, M. (2010). The era of molecular and other non-culture- based methods in diagnosis of sepsis. Clin Microbiol Rev 23, 235–251. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Thu, 04 May 2017 03:44:02 Journal of Medical Microbiology 62 Molecular diagnosis of sepsis Paolucci, M., Landini, M. P. & Sambri, V. (2010). Conventional and molecular techniques for the early diagnosis of bacteraemia. Int J Antimicrob Agents 36 (Suppl 2), S6–S16. Petti, C. A. (2007). Detection and identification of microorganisms by gene amplification and sequencing. Clin Infect Dis 44, 1108–1114. Picard, F. J. & Bergeron, M. G. (2002). Rapid molecular theranostics in infectious diseases. Drug Discov Today 7, 1092–1101. admitted from the emergency department with sepsis. J Clin Microbiol 48, 26–33. Wallet, F., Nseir, S., Baumann, L., Herwegh, S., Sendid, B., Boulo, M., Roussel-Delvallez, M., Durocher, A. V. & Courcol, R. J. (2010). Preliminary clinical study using a multiplex real-time PCR test for the detection of bacterial and fungal DNA directly in blood. Clin Microbiol Infect 16, 774–779. New approaches to sepsis: molecular diagnostics and biomarkers. Clin Microbiol Rev 25, 609–634. Weinstein, M. & Doern, G. (2011). A critical appraisal of the role of the clinical microbiology laboratory in the diagnosis of bloodstream infections. J Clin Microbiol 49 (9 Suppl), S26–S29. Rivers, E. P., Katranji, M., Jaehne, K. A., Brown, S., Abou Dagher, G., Cannon, C. & Coba, V. (2012). Early interventions in severe sepsis and Wellinghausen, N., Kochem, A. J., Disqué, C., Mühl, H., Gebert, S., Winter, J., Matten, J. & Sakka, S. G. (2009). Diagnosis of bacteremia in septic shock: a review of the evidence one decade later. Minerva Anestesiol 78, 712–724. whole-blood samples by use of a commercial universal 16S rRNA genebased PCR and sequence analysis. J Clin Microbiol 47, 2759–2765. Schaub, N., Frei, R. & Müller, C. (2011). Addressing unmet clinical Wolk, D. & Fiorello, A. B. (2010a). Code sepsis: rapid methods to needs in the early diagnosis of sepsis. Swiss Med Wkly 141, w13244. diagnose sepsis and detect hematopathogens: Part I: the impact and attributes of sepsis. Clin Microbiol Newslett 32, 33–37. Tsalik, E. L., Jones, D., Nicholson, B., Waring, L., Liesenfeld, O., Park, L. P., Glickman, S. W., Caram, L. B., Langley, R. J. & other authors (2010). Multiplex PCR to diagnose bloodstream infections in patients Wolk, D. & Fiorello, A. B. (2010b). Code sepsis: rapid methods to Reinhart, K., Bauer, M., Riedemann, N. C. & Hartog, C. S. (2012). http://jmm.sgmjournals.org diagnose sepsis and detect hematopathogens: Part II: challenges to the laboratory diagnosis of sepsis. Clin Microbiol Newslett 32, 41–49. Downloaded from www.microbiologyresearch.org by IP: 88.99.165.207 On: Thu, 04 May 2017 03:44:02 1679