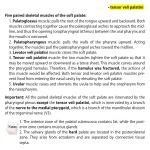
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Soft palate muscle responses to negative upper airway pressure T. C. AMIS, N. O’NEILL, J. R. WHEATLEY, T. VAN DER TOUW, E. DI SOMMA, AND A. BRANCATISANO Department of Respiratory Medicine, Westmead Hospital, and University of Sydney, Westmead, New South Wales 2145, Australia soft palate muscles; negative pressure; superior laryngeal nerve RETROPALATAL AIRWAY PATENCY is controlled via soft palate muscle activity (20), and, during sleep, this segment of the upper airway is a major site of narrowing in both normal humans (6) and patients with the obstructive sleep apnea (OSA) syndrome (5). Consequently, depression of soft palate muscle activity during sleep, with resultant impaired defense of retropalatal airway caliber, has emerged as a potentially important factor in the pathogenesis of OSA (21, 25). Negative pressure within the upper airway lumen (NUAP) is a well-recognized and potent stimulus for the reflex recruitment of upper airway dilator muscle activity. Upper airway muscles known to be responsive to NUAP include the alae nasi (23), genioglossus (3, 4, 14, 23, 24), cricothyroid (13), posterior cricoarytenoid (13, 23), and sternohyoid and sternothyroid (13). The tensor veli palatini (25), levator veli palatini (18), palatoglossus (18, 19), and palatopharyngeus (17) muscles are also reported to be recruited by NUAP. Negative pressure recruitment of upper airway electromyographic muscle (EMG) activity is mediated via a reflex response originating from upper airway mechanoreceptors (8, 9, 15, 27) and having afferent pathways thought to involve the trigeminal, glossopharyngeal, and superior laryngeal nerves. Thus, for muscles such as the genioglossus, receptors located in the nasal, pharyngeal, and laryngeal segments of the upper airway are reportedly involved (2, 8, 9, 15) in the response. The implication from such a distribution of receptor sites is that exposure of any single upper airway segment to NUAP will result in the global recruitment of upper airway dilator muscle activity. However, the soft palate contains both elevator and depressor muscles. Consequently, the resultant effect (on upper airway geometry) of global recruitment of palatal muscles is likely to depend on interactions between anatagonists, which, in turn, will depend on relative mechanical advantage and the responsiveness of individual muscles to NUAP. The afferent pathways for augmentation of soft palate muscle activity with NUAP have not been defined (25). Consequently, the relative contribution (to soft palate muscle recruitment) of receptors located in different topographical zones of the upper airway is not understood. Furthermore, in a previous study in dogs (22), recruitment of individual soft palate muscles by NUAP varied, with recruitment of levator being the least reproducible of the muscles studied. This finding has led us to hypothesize that there are differences in the linkage of individual soft palate muscles to the NUAP reflex (i.e., muscle-specific reflex responses). In addition, the magnitude of individual soft palate muscle responses to differing levels of NUAP (i.e., stimulusresponse characteristics) have not been defined. The strength of the response of individual soft palate muscles to NUAP is relevant to their ability to contribute to the resolution and prevention of obstructive apneas in OSA. Thus the aims of the present study were as follows: 1) localize the negative-pressure-sensitive zones within the upper airway that participate in the NUAPmediated reflex recruitment of individual palatal muscles and 2) define stimulus-response characteristics for recruitment of individual palatal muscles with NUAP. METHODS The costs of publication of this article were defrayed in part by the payment of page charges. The article must therefore be hereby marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. http://www.jap.org We studied 11 adult crossbred dogs (5 males, 6 females) under general anaesthesia induced by intravenous pentobarbital sodium (25–30 mg/kg) followed by intravenous a-chloralose (initial dose 25 mg/kg). Anesthesia was maintained with 8750-7587/99 $5.00 Copyright r 1999 the American Physiological Society 523 Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 Amis, T. C., N. O’Neill, J. R. Wheatley, T. Van der Touw, E. Di Somma, and A. Brancatisano. Soft palate muscle responses to negative upper airway pressure. J. Appl. Physiol. 86(2): 523–530, 1999.—The afferent pathways and upper airway receptor locations involved in negative upper airway pressure (NUAP) augmentation of soft palate muscle activity have not been defined. We studied the electromyographic (EMG) response to NUAP for the palatinus, tensor veli palatini, and levator veli palatini muscles in 11 adult, supine, tracheostomized, anesthetized dogs. NUAP was applied to the nasal or laryngeal end of the isolated upper airway in six dogs and to four to six serial upper airway sites from the nasal cavity to the subglottis in five dogs. When NUAP was applied at the larynx, peak inspiratory EMG activity for the palatinus and tensor increased significantly (P , 0.05) and plateaued at a NUAP of 210 cmH2O. Laryngeal NUAP failed to increase levator activity consistently. Nasal NUAP did not increase EMG activity for any muscle. Consistent NUAP reflex recruitment of soft palate muscle activity only occurred when the larynx was exposed to the stimulus and, furthermore, was abolished by bilateral section of the internal branches of the superior laryngeal nerves. We conclude that soft palate muscle activity may be selectively modulated by afferent activity originating in the laryngeal and hypopharyngeal airway. 524 PALATAL MUSCLE RESPONSES TO UPPER AIRWAY PRESSURE an intermittent infusion of a 0.5% a-chloralose solution administered via a cannula inserted into a femoral vein. a-Chloralose produces stable, long-lasting, light anesthesia and has been used widely in animal studies examining upper airway reflexes (11, 23, 26). Anesthesia levels were adjusted, as necessary, to maintain a stable heart rate and blood pressure throughout the study. Seven of the animals were also part of a previous study in which responses of the genioglossus and hyoepiglotticus muscles to NUAP were examined (1). The investigation was approved by the Western Sydney Area Health Service Animal Care and Ethics Committee. Experimental Preparation Bipolar Teflon-coated fine-wire electrodes (40 gauge) were inserted per orally via a 23-gauge hypodermic needle into each soft palate muscle by using a technique we have described previously (22). Electrodes were placed unilaterally in the tensor, levator, and palatinus muscles (equivalent to the human musculus uvulae). Placement of the electrodes in each muscle was confirmed by visual observation of soft palate movements during tetanic low-voltage electrical stimulation (model S48 Grass stimulator, 5–7 V, 2-s duration, 40 pulses/s, 0.2 ms/pulse) applied via the fine-wire electrodes. Correct placement of the electrodes was accepted only when specific soft palate movements characteristic for each soft palate muscle (22) and unaccompanied by visual movement of any other structures were observed during electrical stimulation. The raw EMG signal was filtered (80–1,000 Hz), amplified, rectified, and integrated (model NT1900, Neotrace) with a time constant of 100 ms to produce a moving time average (MTA) EMG. In addition, the raw EMG was displayed on an oscilloscope as well as transformed into an audio signal via an amplifier and loudspeaker. These visual and auditory signals were used to determine the presence of action potentials in the raw EMG signal. Data Recording The volume, pressure, and integrated EMG signals were recorded on a strip-chart recorder (model 7758B, HewlettPackard). Experimental Protocol Measurements of soft palate muscle MTA EMG activity were obtained during quiet tidal tracheostomy breathing (control) and during progressive sequential (0 to 240 cmH2O in 25-cmH2O steps) or single-step (0 to 210, 0 to 220, and 0 to 232 to 240 cmH2O) changes in NUAP. The NUAP was applied to either the nasal (via the face mask) or laryngeal end of the isolated upper airway, via the cranial tracheal cannula in group 1 dogs or via the retrograded endotracheal tube in group 2 dogs. Each NUAP stimulus was applied for 5–10 breaths. One to two runs of progressive sequential NUAP were obtained for each condition in each dog, whereas one to three runs were obtained for the single-step changes in NUAP. In seven dogs, studies were performed before and after bilateral section of the SLNin. Data Analysis The MTA EMG activity was quantified in arbitrary units (AU) above baseline (i.e., where the raw EMG did not show any action potentials). Timing of the soft palate muscle MTA EMG signal was related to the VT signal. Peak inspiratory and peak expiratory MTA EMG activity was measured as the maximum value of MTA EMG activity during inspiration and expiration, respectively. Tonic activity was defined as the minimum value of MTA EMG measured above baseline. The EMG activity was measured for four to six representative breaths, usually the five breaths immediately preceding NUAP for control and the first five breaths after application of NUAP. These data were averaged to produce single control and intervention values for each NUAP challenge. The data from repeated runs were then averaged and expressed as single values at each NUAP level for each dog. The analysis of the topographical distribution of responses to NUAP was confined to an analysis of changes in EMG Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 The animals were studied supine with the mouth closed and secured with tape. A tight-fitting face mask was sealed to the animal’s muzzle. Pressure in the mask was measured with a pressure transducer (6100 cmH2O, Celesco Transducer Products, IDM Instruments, Dandenong, Victoria, Australia). The trachea was divided between the fourth and fifth cartilage rings caudal to the cricoid cartilage. Care was taken to preserve the recurrent laryngeal nerves. Separate tracheal cannulas were inserted and fastened to the cranial and caudal cut ends of the trachea. Airflow was measured at the caudal tracheal cannula with a pneumotachograph (Fleisch no. 1) coupled to a differential pressure transducer (MP 45, 65 cmH2O, Validyne, Northridge, CA). Tidal volume (VT ) was measured by electrical integration of the flow signal. In six dogs (group 1), pressure in the laryngeal lumen was measured with a pressure transducer attached to a side port on the cranial tracheal cannula. With the use of three-way taps, a high-impedance negative-pressure source was connected to either the cranial tracheal cannula or the face mask, thus allowing a constant negative pressure to be applied to the nasal or laryngeal end of the isolated and sealed upper airway. The remaining five animals (group 2) were prepared in an identical manner except that a cuffed endotracheal tube (internal diameter 5.0 mm, external diameter 6.9 mm, length 23 cm, Mallinckrodt) was passed into the nasopharyngeal airway via the cranial tracheal cannula. The tip of this tube was placed at the nasal choanae, and the cuff was inflated. Negative pressure was then applied to the airway via the endotracheal tube with the applied pressure measured at the caudal end of the tube via a pressure transducer (MP 45, 6100 cmH2O, Validyne). The cuff was then deflated, and the tip of the tube was moved caudally by 2–4 cm. The cuff was then inflated, and negative pressure was reapplied. This procedure was repeated until the tip of the tube was caudal to the glottis and in the cranial trachea. In this manner, systematically longer segments of the nasopharyngeal airway were exposed to the NUAP stimulus. The position of the tip of the tube was assessed from a distance scale marked on the tube at the commencement of the study when, with the mouth open, the position of the tube could be related visually and by palpation to upper airway structures (i.e., glottis, tip of epiglottis, and nasal choanae). In all group 2 dogs, the cranial tracheal cannula (and laryngeal lumen) was open to the atmosphere for all measurements except those in which the endotracheal tube tip was caudal to the glottis. In seven of the dogs, the internal branches of the superior laryngeal nerve (SLNin) were identified bilaterally at their entrance to the thyrohyoid membrane and then were separated from surrounding structures and tagged for later identification and section. EMG PALATAL MUSCLE RESPONSES TO UPPER AIRWAY PRESSURE RESULTS Transmision of NUAP Through the Upper Airway In all group 1 dogs, the changes in NUAP applied at either the larynx/cranial trachea or the face mask were not transmitted to the opposite end of the upper airway for any NUAP level studied (Fig. 1). In the group 2 dogs, NUAP was transmitted to the face mask in all cases where the tip of the endotracheal tube was at the nasal choanae. Transmission also occurred to varying degrees as the tube was moved caudally. When the tube was in the cranial trachea, partial transmission of the pressure stimulus (,5–50%) to the face mask occurred in three dogs. Laryngeal NUAP Application: SLNin Intact Palatinus. Data for palatinus MTA EMG activity were obtained in 10 dogs. During control conditions, respiratory-related phasic inspiratory palatinus MTA EMG activity was detected in six dogs, phasic expira- Fig. 1. Strip-chart recording for 1 dog from group 1 showing the following from top to bottom: moving time average (MTA) EMG activity in arbitrary units of the palatinus (PAL), levator veli palatini (LP), and tensor veli palatini (TP); tidal volume (VT ), and pressure in the face mask (Pmask) and laryngeal lumen (Plarynx). Shown is single-step application of 210 cmH2O pressure to 1) laryngeal/cranial tracheal end [Laryngeal negative upper airway pressure (NUAP)], 2) nasal end (Nasal NUAP) of isolated upper airway [with internal branches of superior laryngeal nerves (SLNin) intact], and 3) laryngeal/cranial tracheal end of upper airway after bilateral section of SLNin (Laryngeal NUAP-SLNin Cut). Insp, inspiration; 0, baseline EMG activity. Amplifier gains shown as 32 and 35 (lower numbers represent higher amplification). Note gain change for LP and TP in panel at right. Arrows on EMG traces indicate onset of NUAP. Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 activity with NUAP of between 220 and 240 cmH2O. Distance along the upper airway was expressed as a percentage of the total distance from the nasal choanae (0%) to the glottis (100%). Group mean data were then analyzed for three zones in the nasopharyngeal airway: 1) measurements obtained at all sites ,70% of the distance from the nasal choanae to the glottis, i.e., rostral zone; 2) measurements obtained between the 70% distance point and the glottis, i.e., epiglottic zone; and 3) measurements obtained with NUAP applied below the glottis, i.e., subglottic zone. Group 1 and group 2 dogs showed similar responses; hence the data, where applicable, have been pooled for analysis. Similar findings were also obtained for both single-step and progressive graded changes for the same level of NUAP (P . 0.05); consequently, these data have also been pooled for analysis. Statistical comparisons were made by using a paired t-test for single-condition paired data and ANOVA (with appropriate adjustment where neccessary for unbalanced data) for multiple-condition comparisons. Fisher’s protected least significant difference test was used as a post hoc multiple-comparison technique. P , 0.05 was taken as significant. 525 526 PALATAL MUSCLE RESPONSES TO UPPER AIRWAY PRESSURE tory activity was found in four dogs, and low-level tonic activity was present in three dogs. Application of laryngeal NUAP increased palatinus peak inspiratory EMG (by .0.5 AU) in 94% of 128 trials, peak expiratory EMG in 66%, and tonic EMG in 64%. Figure 1 shows the response to a single-step change in NUAP of 0 to 210 cmH2O in one dog. Compared with control values, peak inspiratory palatinus EMG activity increased significantly with all levels of NUAP (P , 0.05; Fig. 2A). Peak expiratory activity also increased significantly with all levels of NUAP less than 25 cmH2O (P , 0.05; Fig. 2B), whereas tonic activity increased with all levels of NUAP less than 210 cmH2O (P , 0.05; Fig. 2C). Beyond 210 cmH2O, larger decreases in NUAP (up to 240 cmH2O) did not result in any significant (P . 0.05) further augmentation of palatinus EMG activity (Fig. 2). Tensor veli palatini. Data for tensor MTA EMG activity were obtained in 10 dogs. During control Fig. 2. Group mean data for peak inspiratory (PI; A), peak expiratory (PE; B), and tonic (T; C) MTA EMG of palatinus muscle vs. pressure at larynx or nares (Pressure). Data are shown for application of progressive sequential negative pressure steps (NUAP) at larynx/ cranial trachea (r; n 5 10 dogs) and nares (j; n 5 9 dogs), both with SLNin intact, and at larynx/cranial trachea after bilateral section of SLNin (s; n 5 6 dogs). au, Arbitrary units. Bars, 61 SE. * P , 0.05, compared with value at 0 cmH2O. conditions, respiratory-related phasic inspiratory tensor EMG activity was detected in six dogs, phasic expiratory activity was found in six dogs, and low-level tonic activity was present in six dogs. Application of laryngeal NUAP increased peak inspiratory tensor MTA EMG in 74% of 132 trials, peak expiratory EMG in 30%, and tonic EMG in 32%. Compared with control values, peak inspiratory (but not peak expiratory or tonic) tensor veli palatini EMG activity increased significantly with all levels of NUAP less than 25 cmH2O (P , 0.05; Fig. 3). Beyond 210 cmH2O, larger decreases in NUAP (up to 240 cmH2O) did not result in any significant (P . 0.05) further augmentation of tensor EMG activity (Fig. 3). Levator veli palatini. Data for levator MTA EMG activity were obtained from nine dogs. During control conditions, respiratory-related phasic inspiratory levator EMG activity was detected in four dogs and phasic expiratory activity in five animals. No tonic activity was present in any dog. Application of laryngeal NUAP resulted in variable EMG responses. Peak inspiratory levator EMG increased in only 43% of 118 trials. Peak expiratory and tonic activity increased in only 9 and 10% of trials, respectively. Consequently, there was no Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 Fig. 3. Group mean data for PI (A), PE (B), and T (C) MTA EMG of tensor veli palatini muscle vs. pressure at larynx or nares (Pressure). Data are shown for application of progressive sequential negative pressure steps (NUAP) at larynx/cranial trachea (r; n 5 10 dogs) and nares (j; n 5 10 dogs), both with SLNin intact, and at larynx/cranial trachea after bilateral section of SLNin (s; n 5 6 dogs). Bars, 61 SE. * P , 0.05 compared with value at 0 cmH2O. PALATAL MUSCLE RESPONSES TO UPPER AIRWAY PRESSURE 527 peak inspiratory, peak expiratory, and tonic EMG activity failed to increase with the application of laryngeal NUAP in the majority (.83%) of the 55 trials performed. There was no significant change in EMG activity with any individual level of laryngeal NUAP for any muscle (P . 0.05; Figs. 1–4). Topographical Distribution of NUAP Responses Fig. 4. Group mean data for PI (A), PE (B), and T (C) MTA EMG of the levator veli palatini muscle vs. pressure at larynx or nares (Pressure). Data are shown for application of progressive sequential negative pressure steps (NUAP) at larynx/cranial trachea (r; n 5 9 dogs) and nares (j; n 5 10 dogs), both with SLNin intact, and at larynx/cranial trachea after bilateral section of the SLNin (s; n 5 6 dogs). Bars, 61 SE. * P , 0.05 compared with value at 0 cmH2O. significant (P .0.05) increase in levator veli palatini EMG activity with any level of NUAP applied at the larynx (Fig. 4). Nasal NUAP Application: SLNin Intact Data for MTA EMG activity during NUAP applied to the nose (and not transmitted to the larynx) were obtained in 9 dogs for palatinus and in 10 dogs for both levator and tensor. In all three muscles, peak inspiratory, peak expiratory, and tonic EMG activity failed to increase or decreased with the application of nasal NUAP in the vast majority (.75%) of the 100–111 trials performed. There was no significant change in EMG with any individual level of nasal NUAP for any muscle (Figs. 1–4) except for a small, but significant (P , 0.05), increase in tonic EMG activity for the levator at a NUAP of 240 cmH2O (Fig. 4C). This mean change was very small (0.1 AU) and, in fact, was beyond the resolution of our measurement technique (0.5 AU). Laryngeal NUAP Application: SLNin Cut After section of the SLNin, data was obtained in six dogs for each soft palate muscle. In all three muscles, Fig. 5. A: change in PI palatinus muscle MTA EMG activity from control and recorded during 189 applications of 220 to 240 cmH2O NUAP to all sites in upper airway in 5 dogs. Distance along upper airway has been expressed as percentage of total distance from nasal choanae (NC) to glottis (G). Also shown is range of distances encountered for epiglottic tip (ET). Note that there is considerable overlap of data points such that total number of points visible on plot is ,189. B: group mean (1SE) data (n 5 5 dogs) for change in PI, PE, and T MTA EMG activity occurring with NUAP challenges applied at rostral, epiglottic, and subglottic zones of upper airway. Dashed lines, upper airway zones; dotted line, zero EMG change with NUAP. * P , 0.05 compared with control. 1 P , 0.05 compared with rostral zone. Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 Palatinus. When NUAP challenges (n 5 189) were applied at different topographical sites within the upper airway, there was no significant change in palatinus EMG activity within both the rostral (P . 0.5) and epiglottic zones (P . 0.1). Within the subglottic zone, peak inspiratory palatinus EMG increased significantly with NUAP (P 5 0.05; Fig. 5, A and B). Peak expiratory and tonic activity also showed increases with NUAP; however, these changes achieved only borderline significance (P 5 0.06 and P 5 0.07, respectively; Fig. 5B). When the change in EMG activity with NUAP was compared between zones, the changes in peak inspiratory and peak expiratory EMG activity in 528 PALATAL MUSCLE RESPONSES TO UPPER AIRWAY PRESSURE Fig. 7. A: change in PI levator veli palatini muscle MTA EMG activity recorded during 183 applications of 220 to 240 cmH2O NUAP to all sites in upper airway in 5 dogs. Distance along upper airway has been expressed as percentage of total distance from NC to G. Also shown is range of distances encountered for ET. Note that there is considerable overlap of data points such that total number of points visible on plot is ,183. B: group mean (1SE) data (n 5 5 dogs) for change in PI, PE, and T MTA EMG activity occurring with NUAP challenges applied at rostral, epiglottic, and subglottic zones of upper airway. Dashed lines, upper airway zones; dotted line, zero EMG change with NUAP. 1 P , 0.05 compared with rostral and epiglottic zones. in peak inspiratory EMG activity (but not peak expiratory or tonic activity) was significantly greater in the subglottic zone than in the other two zones (P , 0.05, Fig. 7). DISCUSSION Fig. 6. A: change in PI tensor veli palatini muscle MTA EMG activity recorded during 197 applications of 220 to 240 cmH2O NUAP to all sites in upper airway in 5 dogs. Distance along upper airway has been expressed as percentage of total distance from NC to G. Also shown is range of distances encountered for ET. Note that there is considerable overlap of data points such that total number of points visible on plot is ,197. B: group mean (1SE) data (n 5 5 dogs) for change in PI, PE, and T MTA EMG activity occurring with NUAP challenges applied at rostral, epiglottic, and subglottic zones of upper airway. Dashed lines, upper airway zones; dotted line, zero EMG change with NUAP. * P , 0.05 compared with control. The principal findings in this study are that in anesthetized, supine, tracheostomized, mouth-closed dogs 1) tensor veli palatini and palatinus muscle EMG activity is augmented by negative pressure in the hypopharynx, larynx, and cranial trachea, 2) levator veli palatini muscle EMG activity is weakly and inconsistently recruited by laryngeal NUAP, 3) NUAP applied exclusively to the nasal passages or nasopharynx does not recruit soft palate muscle EMG activity, 4) recruitment of soft palate muscle activity with NUAP is mediated via the SLNin, and 5) the reflex activation of soft palate muscles with NUAP is maximal with a NUAP level of 210 cmH2O. In addition, it was observed that in most dogs the upper airway remained closed during the application of NUAP despite maximal Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 the subglottic zone were significantly greater than those in the rostral zone (P , 0.05). However, changes in the epiglottic zone were not significantly different from those in the other two zones (P . 0.05). Tensor veli palatini. When NUAP challenges (n 5 197) were applied at different topographical sites within the upper airway, changes in peak inspiratory, peak expiratory, and tonic EMG activity of the tensor veli palatini muscle were not significant within the rostral (P . 0.4) and epiglottic (P . 0.1) zones. Within the subglottic zone, peak expiratory and tonic EMG activity also did not change (P . 0.1). However, there was a significant increase in peak inspiratory activity (P 5 0.04; Fig. 6, A and B). Although the changes in EMG activity with NUAP tended to be greater in the epiglottic and subglottic zones (Fig. 6B), a significant difference (P . 0.1) between the zones was not detected. Levator veli palatini. When NUAP challenges (n 5 183) were applied at different topographical sites within the upper airway, there was no significant change in levator veli palatini EMG activity within any zone (P . 0.08; Fig. 7, A and B). However, when the change in EMG activity was compared between zones, the change PALATAL MUSCLE RESPONSES TO UPPER AIRWAY PRESSURE application of NUAP to the nasal cavity has been shown to augment alae nasi and posterior cricoarytenoid muscle activity in some studies (23, 26), whereas other studies have attributed the response to NUAP almost entirely to laryngeal afferents (11, 16). Furthermore, Kaminuma and co-workers (11) reached the conclusion that nasal pressure receptors have only minimal impact on the reflex recruitment of posterior cricoarytenoid muscle activity in dogs. The present study now extends this conclusion to the canine soft palate muscles. Some previous studies have suggested that the oropharynx is also not an important site for NUAP-related reflex recruitment of genioglossus muscle activity (2). Moreover, sectioning of the glossopharyngeal nerves in cats increases rather than decreases the augmentation of hypoglossal nerve activity with NUAP (8). Results from the present study suggest that the pharynx is also not important in the NUAP-mediated reflex recruitment of the soft palate muscles. In the present study, laryngeal afferent activity appeared to be the only pathway for augmentation of soft palate muscle activity by NUAP. We base this conclusion on the following results: 1) the response was not elicited by nasal NUAP, 2) the response disappeared after sectioning of the SLNin, and 3) the response was confined to the epiglottic/laryngeal region of the upper airway in the group 2 dogs. However, evidence obtained in laryngectomized humans, in whom afferent impulses from the larynx have been ablated, suggests that genioglossus muscle EMG activity is still augmented by NUAP (10), an effect attributed to receptors located in the oropharyngeal and/or nasopharyngeal mucosa. This evidence suggests that, at least in humans, pharyngeal receptors do exist and may play an enhanced role in the absence of laryngeal receptor input. However, in the intact upper airway it seems that it is the laryngeal receptors which play the dominant role. The stimulus response characteristics for soft palate muscle activation by graded NUAP have not been previously studied over the range of NUAP employed in the present study. The finding that there was no further augmentation of soft palate muscle EMG activity by NUAP beyond 210 cmH2O is similar to previously reported data for other upper airway muscles (4, 17, 23). The plateau of reflex recruitment might be interpreted as representing maximal muscle EMG activation. However, we have previously observed spontaneous levels of soft palate muscle EMG activity during upper airway breathing in anesthetized dogs (22) that were two to four times higher than those measured at an equivalent level of NUAP (211.3 6 1.8 cmH2O) to that associated with the maximum EMG recruitment in the present study. Plateauing of upper airway muscle responses to NUAP may then suggest saturation of receptor activation, with muscle EMG recruitment via this reflex pathway limited to submaximal levels. Indeed, discharge frequencies of receptors generating changes in afferent activity in the SLNin in response to NUAP have been shown to reach plateau levels in the 27- to 228-cmH2O range in cats (9). Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 NUAP-mediated reflex recruitment of soft palate muscle activity. Application of NUAP to the laryngeal end of the upper airway (and not transmitted to the nose) consistently resulted in the recruitment of palatinus and tensor veli palatini muscle EMG activity (see Figs. 1–3). This augmentation of EMG activity occurred on the first breath after the change in NUAP (see Fig. 1). Incomplete adaptation was observed with maintenance of the stimulus being associated with a fall in response compared with the first breath after application of NUAP (see Fig. 1). This phenomenon has been reported previously for other upper airway muscles (13) and also in terms of the discharge of receptors (9). The responses of the palatinus and tensor veli palatini muscles to laryngeal NUAP in the present study are in general agreement with our previous findings in dogs in which only a single level of NUAP was used (22) and with those of Wheatley et al. (25) in humans. However, the lack of consistent recruitment of the levator veli palatini by laryngeal NUAP was surprising in view of previous results demonstrating responses of the levator to NUAP in humans (19) and animals (22). The reason for this discrepancy is not entirely clear. However, even in our previous study, some individual animals did not show a levator response to NUAP (22). In the present study, levator responses to NUAP were small and variable. Because general anesthesia is known to depress the recruitment of upper airway muscles (7), the effect of anesthesia on levator activity is a concern; however, a-chloralose produces light, stable anesthesia, and all soft palate muscles within each animal were studied concurrently. Consequently, for the depressant effects of anesthesia to have been responsible for the lack of recruitment of levator, this would have had to have been a selective effect for this muscle compared with the other soft palate muscles. Thus the levator veli palatini in the dog appears to be only inconsistently and weakly recruited in response to NUAP applied at the larynx. This may also be the case in humans because levator veli palatini EMG activity in humans has been shown to have high inter- and intrasubject variability both in terms of its activity during quiet breathing and in its response to chemostimulation (12). The complete loss of the response to laryngeal NUAP after bilateral section of the SLNin is consistent with results reported for the response of other upper airway muscles to laryngeal NUAP (13, 15, 23) and establishes that the SLNin is also the afferent pathway for soft palate muscle recruitment. When the NUAP was applied exclusively to the nasal passages (and not transmitted to the larynx), there was no augmentation of soft palate muscle EMG activity. This finding suggests that local negative pressure reflex control of soft palate muscle activity does not involve receptors located in the nose. This conclusion for the soft palate muscles is in contrast to results reported for the genioglossus in rabbits, where nasal NUAP (not transmitted to the larynx) has been shown to recruit genioglossus EMG activity (15). In dogs, the 529 530 PALATAL MUSCLE RESPONSES TO UPPER AIRWAY PRESSURE In conclusion, we have demonstrated that, in supine, anesthetized dogs, reflex recruitment of soft palate muscle activity by NUAP is predominantly modulated by afferent activity originating from the laryngeal and/or hypopharyngeal airway and transmitted via the SLNin. The soft palate muscles may exhibit selective recruitment in response to NUAP in that the levator frequently failed to respond to NUAP, whereas the palatinus and, to a lesser extent, tensor both consistently increased their activity. The response of the soft palate muscles to NUAP reached a maximum at a NUAP of 210 cmH2O; however, this level of activity was insufficient to ensure a patent upper airway in most dogs. Consequently, we speculate that NUAPmediated reflex recruitment of upper airway muscles, including the soft palate muscles, may be more important in the prevention of upper airway collapse than in the resolution of any resultant airway closure. Received 16 March 1998; accepted in final form 14 October 1998. REFERENCES 1. Amis, T. C., N. O’Neill, T. Van der Touw, and A. Brancatisano. Control of epiglottic position in dogs: role of negative upper airway pressure. Respir. Physiol. 105: 187–194, 1996. 2. Horner, R. L., J. A. Innes, H. B. Holden, and A. Guz. Afferent pathway(s) for pharyngeal dilator reflex to negative pressure in man: a study using upper airway anaesthesia. J. Physiol. (Lond.) 436: 31–44, 1991. 3. Horner, R. L., J. A. Innes, M. J. Morrell, S. A. Shea, and A. Guz. The effect of sleep on reflex genioglossus muscle activation by stimuli of negative airway pressure in humans. J. Physiol. (Lond.) 476: 141–151, 1994. 4. Horner, R. L., J. A. Innes, K. Murphy, and A. Guz. Evidence for reflex upper airway dilator muscle activation by sudden negative airway pressure in man. J. Physiol. (Lond.) 436: 15–29, 1991. 5. Hudgel, D. W. Variable site of airway narrowing among obstructive sleep apnea patients. J. Appl. Physiol. 61: 1403–1409, 1986. 6. Hudgel, D. W., and C. Hendricks. Palate and hypopharynx— sites of inspiratory narrowing of the upper airway during sleep. Am. Rev. Respir. Dis. 138: 1542–1547, 1988. 7. Hwang, J., W. M. St. John, and D. Bartlett, Jr. Respiratoryrelated hypoglossal nerve activity: influence of anesthetics. J. Appl. Physiol. 55: 785–792, 1983. 8. Hwang, J., W. M. St. John, and D. Bartlett, Jr. Afferent pathways for hypoglossal and phrenic responses to changes in upper airway pressure. Respir. Physiol. 55: 341–354, 1984. 9. Hwang, J., W. M. St. John, and D. Bartlett, Jr. Receptors responding to changes in upper airway pressure. Respir. Physiol. 55: 355–366, 1984. Downloaded from http://jap.physiology.org/ by 10.220.33.4 on May 3, 2017 The authors thank K. Byth for statistical advice. This study was supported by the National Health and Medical Research Council of Australia, a Harry Windsor Research Grant from the Community Health and Anti-Tuberculosis Association of New South Wales, and the Garnett Passe and Rodney Williams Foundation. Address for reprint requests: T. C. Amis, Dept. of Respiratory Medicine, Westmead Hospital, Westmead, NSW 2145, Australia. 10. Innes, J. A., M. J. Morrell, I. Kobayashi, R. D. Hamilton, and A. Guz. Central and reflex neural control of genioglossus in subjects who underwent laryngectomy. J. Appl. Physiol. 78: 2180–2186, 1995. 11. Kaminuma, O., H. Tsubone, J. M. Matias, R. Nishimura, and S. Sugano. Reflex activities of the upper airway muscles during experimental nasal occlusion in anesthetized dogs. J. Vet. Med. Sci. 53: 93–99, 1991. 12. Launois, S. H., J. Tsui, and J. W. Weiss. Respiratory function of velopharyngeal constrictor muscles during wakefulness in normal adults. J. Appl. Physiol. 82: 584–591, 1997. 13. Mathew, O. P. Upper airway negative-pressure effects on respiratory activity of upper airway muscles. J. Appl. Physiol. 56: 500–505, 1984. 14. Mathew, O. P., Y. K. Abu-Osba, and B. T. Thach. Influence of upper airway pressure changes on genioglossus muscle respiratory activity. J. Appl. Physiol. 52: 438–444, 1982. 15. Mathew, O. P., Y. K. Abu-Osba, and B. T. Thach. Genioglossus muscle responses to upper airway pressure changes: afferent pathways. J. Appl. Physiol. 52: 445–450, 1982. 16. Mathew, O. P., and F. B. Sant’Ambrogio. Laryngeal reflexes. In: Respiratory Function of the Upper Airway, edited by O. P. Mathew and G. Sant’Ambrogio. New York: Dekker, 1988, vol. 35, p. 259–302. (Lung Biol. Health Dis. Ser.) 17. Mortimore, I. L., and N. J. Douglas. Palatopharyngeus has respiratory activity and responds to negative pressure in sleep apnoeics. Eur. Respir. J. 9: 773–778, 1996. 18. Mortimore, I. L., and N. J. Douglas. Palatal muscle EMG response to negative pressure in awake sleep apneic and control subjects. Am. J. Respir. Crit. Care Med. 156: 867–873, 1997. 19. Mortimore, I. L., R. Mathur, and N. J. Douglas. Effect of posture, route of respiration, and negative pressure on palatal muscle activity in humans. J. Appl. Physiol. 79: 448–454, 1995. 20. Rodenstein, D. O., and D. C. Stanescu. The soft palate and breathing. Am. Rev. Respir. Dis. 134: 311–325, 1986. 21. Tangel, D. J., W. S. Mezzanotte, and D. P. White. Influence of sleep on tensor palatini EMG and upper airway resistance in normal men. J. Appl. Physiol. 70: 2574–2581, 1991. 22. Van der Touw, T., N. O’Neill, A. Brancatisano, T. Amis, J. Wheatley, and L. A. Engel. Respiratory-related activity of soft palate muscles: augmentation by negative upper airway pressure. J. Appl. Physiol. 76: 424–432, 1994. 23. Van Lunteren, E., W. B. Van de Graaff, D. M. Parker, J. Mitra, M. A. Haxhiu, K. P. Strohl, and N. S. Cherniak. Nasal and laryngeal reflex responses to negative upper airway pressure. J. Appl. Physiol. 56: 746–752, 1984. 24. Wheatley, J. R., W. S. Mezzanotte, D. J. Tangel, and D. P. White. Influence of sleep on genioglossus muscle activation by negative pressure in normal men. Am. Rev. Respir. Dis. 148: 597–605, 1993. 25. Wheatley, J. R., D. J. Tangel, W. S. Mezzanotte, and D. P. White. Influence of sleep on response to negative airway pressure of tensor palatini muscle and retropalatal airway. J. Appl. Physiol. 75: 2117–2124, 1993. 26. Widdicombe, J. G. Nasal and pharyngeal reflexes: protective and respiratory functions. In: Respiratory Function of the Upper Airway, edited by O. P. Mathew and G. Sant’Ambrogio. New York: Dekker, 1988, vol. 35, p. 233–258. (Lung Biol. Health Dis. Ser.) 27. Widdicombe, J. G., G. Sant’Ambrogio, and O. P. Mathew. Nerve receptors of the upper airway. In: Respiratory Function of the Upper Airway, edited by O. P. Mathew and G. Sant’Ambrogio. New York: Dekker, 1988, vol. 35, p. 193–231. (Lung Biol. Health Dis. Ser.)