Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Evaluation of nonacute scrotal
pathology in adult men
VARICOCELE
• A varicocele is caused by dilatation of the
pampiniform plexus of spermatic veins
• It is present in 15 to 20 percent of postpubertal males, occurring in the usually left
hemiscrotum in the vast majority of cases.
• The venous complex in the scrotum dilates
and produces anything from minimal fullness
on Valsalva maneuver to a large soft scrotal
mass ("bag of worms") that decompresses and
disappears in the recumbent position
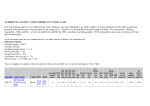
•Grading of varicoceles
Grade
Size
Clinical description
1
Small
Palpable only with valsalva maneuver
2
Moderate
Nonvisible on inspection, but palpable upon standing
3
Large
Visible on gross inspection
• Bilateral varicoceles occur in 33 percent of
patients.
• Unilateral right varicoceles are very rare and
should alert the clinician to possible underlying
pathology causing inferior vena caval obstruction
(renal cell carcinoma with IVC thrombus, right
renal vein thrombosis with clot propagation
down the IVC, etc), since the right gonadal vein
directly empties into the IVC.
Symptoms
• Varicoceles may be asymptomatic or present
with:
– Dull, aching, usually left scrotal pain, typically
noticeable when standing and relieved by
recumbency
– Testicular atrophy, believed to be secondary to
loss of germ cell mass by induction of apoptosis
(programmed cell death) initiated by the
associated slightly increased scrotal temperature
– Decreased fertility
• A large number of infertile men are found to
have a varicocele on examination
• On the other hand, men with varicoceles may
have normal semen parameters and normal
fertility.
• Treatment is indicated for boys who
demonstrate retarded growth of the affected
(usually, left) testis and in young men who
develop testicular atrophy. There are data to
suggest that catch-up growth of the atrophic
testis is possible in some cases after surgery
and that return of testicular size
postoperatively directly correlates with
normal fertility potential
• in the younger infertile man with a clinically
apparent varicocele, it seems reasonable to
recommend surgical ligation
• Subclinical varicoceles are often discovered as
part of an infertility evaluation by
demonstrating retrograde flow to the scrotum
by Color Doppler ultrasonography. The role of
surgical ligation for subclinical varicoceles
associated with subfertility is not clear.
Epididymal cysts and spermatoceles
• Epididymal cysts are usually palpated in the
head (caput) of the epididymis and are
generally asymptomatic
• They occur with increased frequency in male
offspring of mothers who used
diethylstilbestrol during pregnancy. In
addition, epididymal cystadenomas are seen
in more than one-half of patients with Von
Hippel-Lindau disease and are often bilateral
• These are usually not mistaken for other
scrotal pathology, and they can be diagnosed
by scrotal ultrasonography if the clinical
examination is equivocal. No treatment is
required.
• The distinction between a spermatocele and an
epididymal cyst is mainly one of size; epididymal
cystic masses that are larger than 2 cm are called
spermatoceles.
• Spermatoceles are always located superior to the
testis and are palpated as distinct from the testis,
which differentiates them from hydroceles.
Spermatoceles generally range in size from 2 to 5
cm and rarely cause symptoms.
• Occasional patients require surgical excision for
chronic pain related to a spermatocele
Hydroceles
• A hydrocele is a collection
of peritoneal fluid between
the parietal and visceral
layers of the tunica
vaginalis, the investing
layer that directly
surrounds the testis and
spermatic cord
• Symptoms of pain and disability generally
increase with the size of the mass.
• Hydrocele fluid in the scrotal sac transilluminates
well, which differentiates the process from a
possible hematocele, hernia, or solid mass.
• A scrotal ultrasound should be considered if the
diagnosis is in question since a reactive hydrocele
can occur in the presence of a testicular
neoplasm or with acute inflammatory scrotal
conditions.
• Idiopathic hydroceles usually arise over a long
period of time and are the most common type
of hydrocele.
• Inflammatory conditions of the scrotal
contents (epididymitis, torsion, appendiceal
torsion) can produce an acute reactive
hydrocele, which often resolves with
treatment of the underlying condition.
• Thus, treatment is necessary only patients
who are symptomatic (pain, pressure) or for
the rare situation when scrotal skin integrity is
compromised from chronic irritation.
• Hydroceles discovered in infancy are usually
"communicating," since they are associated with
a patent processus vaginalis, which allows flow of
peritoneal fluid into the scrotal sac.
• They usually disappear in the recumbent position
and are often associated with herniation of
abdominal contents (indirect hernia) through the
processus vaginalis.
• Surgical repair is advised in these cases.
TESTICULAR CANCER
• Testicular cancer is relatively rare, but it is the
most common solid tumor in men between
the ages of 18 and 40.
• It usually presents as a painless mass
discovered by the patient or physician on
physical examination, although rapidly
growing germ cell tumors may cause acute
scrotal pain secondary to hemorrhage and
infarction
• On examination, intrascrotal malignancies are
usually firm, nontender masses that do not
transilluminate, although a reactive hydrocele
may be evident with transillumination.
• Scrotal ultrasound is the initial test of choice
to diagnose testicular cancer
• However, several conditions may mimic
neoplasia on ultrasound, including
inflammation, hematoma, infarct, fibrosis, and
tubular ectasia.
• In cases in which the ultrasound is
inconclusive, MRI may help differentiate
benign from malignant lesions
• Any patient suspected of having a testis
cancer should also have blood levels of alpha
fetoprotein (AFP) and the beta subunit of
human chorionic gonadotropin (beta-hCG)
measured.