Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
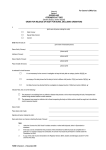
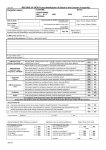
Coroner's Court Witness Claim for Loss of Earnings and Other Expenses N.B. Please read notes of guidance overleaf before completing this form in BLOCK CAPITALS Name: CASE CODE Payable To: Payee Address: Postcode: (mandatory) Contact Tel. No.: Bank Account No.: (mandatory) Third Party Reference: (if Sort Code: (mandatory) Account name: applicable) To be completed by the applicant, if self-employed, or the Witness’ employer, as applicable DAILY LOSS IF DETAINED Gross Loss of Earnings ………………….…… Less Income Tax .………………….….. Less National Insurance ……………...….…… Net loss of Earnings ________________ I certify that the applicant named above will incur the loss of earnings as stated by attending H M Coroner’s Court NAME OF COMPANY ……………..………………………………………………………………………………………. ADDRESS, INCLUDING POSTCODE …………………….…………………………………………....................... ……………………………………………………………………………………………………………………………….. JOB ROLE………………………………………………………..…………………..….. DATE…………..………... NAME…………………………………………………….. SIGNATURE………………..……………………………... HALF DAY FOR CORONER USE: FULL DAY TOTAL LOSS OF EARNINGS: £ P Give full details on continuation sheet & attach receipts. NOTE: payment will not be made without receipts and is subject to maximum limits set by the Ministry of Justice FOR COMPLETION BY AUTHORISING OFFICER NOTE: payment is subject to maximum limits set by the Ministry of Justice FOR COMPLETION BY AUTHORISING OFFICER NOTE: payment is subject to maximum limits set by the Ministry of Justice Out of Pocket Expenses Loss of Earnings Total Claimed TRAVEL Fares: Give full details on continuation sheet an attach receipts DETAILS OF DAILY TRAVEL STARTING DESTINATION POINT Mileage: HOME POSTCODE MODE INQUEST POSTCODE RETURN JOURNEY MILEAGE DAILY COST £ P £ P TOTAL TRAVEL COSTS: Name of Deceased ………………………………………… Date of Coroner’s Court(s) ………………………………..inc. I certify that I have incurred the expenditure as described above as a witness for …… days at (a) Coroner’s Court (s) held from………………..………………….…..to……………………..……………..…..inclusive and attach receipts where appropriate. Signature of claimant ……………………………………………….. Subjective 3 7 0 Cost 3 G P C R Centre 0 Amount Excl. VAT Analysis 0 0 0 8 8 8 Date …………………………………… VAT Incl. VAT Amount TOTAL PAYABLE 9 Approving Officer to Complete the Section Below I certify the attendance and approve the claim for a payment. The amounts claimed are calculated correctly and are within the limits prescribed Approving officer’s name………………..……………………………………… Date…………………………….……....… Signature…………………………………………………….…………………… Contact tel. no……………………...……. Coroner’s Court Witness Claim for Loss of Earnings and Other ExpensesContinuation Sheet NAME:__________________________ DATE OF ATTENDANCE:____________ Date Item Cost Receipt (Y/N)