Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
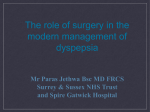
Exp. Anim. 60(2), 141–150, 2011 —Original— Histological Examination of the Relationship between Respiratory Disorders and Repetitive Microaspiration Using a Rat Gastro-Duodenal Contents Reflux Model Keisuke OUE1, 2), Ken-ichi MUKAISHO1), Tomoki HIGO1, 2), Yoshio ARAKI1), Masanori NISHIKAWA2), Takanori HATTORI1), Gaku YAMAMOTO2), and Hiroyuki SUGIHARA1) Departments of 1)Pathology and 2)Oral and Maxillofacial Surgery, Shiga University of Medical Science, Seta-tsukinowa-cho, Otsu, Shiga 520-2192, Japan Abstract: Microaspiration due to gastroesophageal reflux (GER) has been suggested as a factor contributing to the development and exacerbation of several respiratory disorders. To explore the relationship between GER and respiratory disorders, we histologically examined the bilateral lungs of a rat gastroduodenal contents reflux model, which was previously used to investigate the histogenesis of Barrett’s esophagus and esophageal carcinoma. GER was surgically induced in male Wistar rats. The bilateral lungs of the reflux rats were examined with hematoxylin and eosin (HE), PAS-Alcian blue, and Azan staining at 10 and 20 weeks after surgery. Immunohistochemical staining of CD68 and α-SMA was also performed. Aspiration pneumonia with severe peribronchiolar neutrophilic and lymphocytic infiltrates, goblet cell hyperplasia, prominence of blood vessels, and increased thickness of the smooth muscle layer were detected. Bronchiolitis obliterans (BO)-like lesions comprising granulation tissue with macrophages, spindle cells, and multinucleated giant cells in the lumen of respiratory bronchioles were observed in the bilateral lungs of the reflux animals. These findings suggest that the severe inflammation and the BO-like lesions may play a role in exacerbation of the forced expiratory volume in 1 second (FEV 1) in human cases. In conclusion, we speculate that repetitive microaspiration due to GER may contribute to the exacerbation of various respiratory diseases, particularly asthma and chronic obstructive pulmonary disease (COPD), and the development of BO syndrome following lung transplantation. The reflux model is a good tool for examining the causal relationships between GER and respiratory disorders. Key words: bronchiolitis obliterans, gastro-duodenal reflux, microaspiration, rat reflux model, respiratory disorder (Received 12 August 2010 / Accepted 25 November 2010) Address corresponding: K. Mukaisho, Department of Pathology, Shiga University of Medical Science, Seta-tsukinowa-cho, Otsu, Shiga 520-2192, Japan 142 K. Oue, ET AL. Introduction Gastroesophageal reflux disease (GERD) has become a common disorder in the USA and Western Europe in recent decades [16]. The manifestations can be divided into esophageal and extraesophageal syndromes, which affect various tissues and organ systems in addition to the esophagus [28, 41]. Among the various extraesophageal manifestations, causal relationships between GERD and cough, laryngitis, asthma, and dental erosion have been strongly suggested in the Montreal definition [42]. In addition, gastroesophageal reflux (GER) accompanied by regurgitation and microaspiration has been suggested as a contributory factor in several respiratory disorders. Idiopathic pulmonary fibrosis, cystic fibrosis, connective tissue disease, and obstructive lung disease have all been reported to be associated with GER [19, 39, 42]. Moreover, GER has been shown to worsen asthma through esophagobronchial reflex, and to heighten bronchial reactivity and microaspiration [2, 14, 20]. GER has also been reported to be accompanied by neutrophilic airway inflammation [10] and it has been suggested that patients with chronic obstructive pulmonary disease (COPD) along with GERD symptoms are more likely to experience exacerbations than those lacking these symptoms. GERD may also increase the tracheobronchial aspiration of gastric juice directly and/or disturb the clearance of swallowed contents from the pharynx to the esophagus indirectly, leading to frequent exacerbations. Therefore, GER may act as a confounding factor in COPD exacerbations through mechanisms similar to those seen in asthma and/or by increasing airway inflammation [38]. Microaspiration due to GER has been most commonly observed in lung transplant patients in recent years. Lung transplantation has become a therapeutic option for appropriately selected patients with end-stage lung diseases in the last 20 years. However, successful approaches for managing chronic rejection of pulmonary allografts have not yet been developed. Long-term survival of patients with pulmonary allografts is currently hindered by bronchiolitis obliterans syndrome (BOS), a form of chronic rejection that is unique to lung transplantation. Clinical studies suggest that both immuneand non-immune-mediated factors contribute to BOS development. High GER levels with resultant aspiration have been implicated as a non-immune risk factor for BOS development following lung transplantation [15, 22, 31, 34, 35, 43]. GER is promoted after lung transplantation probably because of the potential for iatrogenic vagal nerve injury during lung transplantation and due to the use of immunosuppressive drugs such as calcineurin inhibitors, cyclosporine and tacrolimus that prolong gastric emptying [5, 15, 35]. In addition, bile acids in bronchoalveolar lavage fluid at three months after transplant were found to be associated with BOS development in a time- and dose-dependent manner [17]. These findings suggest that bile acids, not gastric juice in reflux contents, play an important role in BOS development following lung transplantation. In order to establish experimental evidence for causal relationships between GER and respiratory disorders, we examined both lungs of the reflux model, which had previously been used to investigate the histogenesis of Barrett’s esophagus and esophageal carcinoma [11, 12] and was recently used to examine the mechanism of development of extraesophageal syndromes including laryngitis and dental erosion [26, 30]. Materials and Methods All procedures complied with the ethical guidelines for animal experimentation and the care and use of laboratory animals at Shiga University of Medical Science, Japan. Animal models Gastro-duodenal reflux was induced in eight-week-old male Wistar rats (CLEA, Tokyo, Japan) according to a previously reported procedure [11, 12]. Shortly afterwards, the esophagogastric junction was transected, the distal cut end was closed, and the proximal cut end was anastomosed end-to-side to the upper jejunum, approximately 2 cm distal to the origin. After the esophagojejunostomy, a serosal suture (interrupted 7-0 nylon) was placed between the esophagus and jejunum to support the afferent loop side of the anastomosis. As a result, the serosal suture allowed ingested food to easily enter the efferent loop and prevented food from entering the afferent loop. The gastro-duodenal contents flowed through RESPIRATORY DISORDERS AND MICROASPIRATION IN RATS 143 the esophagojejunal stoma and back into the esophagus [11, 12] (Fig. 1). Sham-operated rats, which underwent a laparotomy with blunt manipulation of the abdominal contents under diethyl ether anesthesia, were used as control animals. The reflux animals that survived were euthanized with an overdose of diethyl ether at postoperative week 10 (n=7) or 20 (n=7). Sham-operated control rats were euthanized at similar time points (n=7 per group). Histological examination Resected bilateral lung tissue samples were weighed and fixed in 10% formalin in phosphate-buffered saline for 4 h and embedded in paraffin. Four-micrometer sections were made and stained with hematoxylin and eosin (HE). PAS-Alcian blue staining for detection of goblet cell metaplasia and Azan staining for fibrosis were also performed on the lung samples. The degree of positive cells for PAS-Alcian blue staining was recorded as weak (0), mild (1+), moderate (2+), or strong (3+). Immunohistochemical stainings of CD68 and α-SMA Immunohistochemical staining was performed with mouse monoclonal antibodies: CD68 (a marker for macrophages, Clone:ED1, 1:500, AbD Serotec, Oxford, UK) and α-SMA (a marker for α-smooth-muscle isoform of actin, Clone:ASM-1, 1:200, Progen Biotechnik, Heidelberg, Germany). The staining was performed on a Discovery XT Automated IHC Stainer using the Ventana DABMap detection kit (catalog No. 760-124, Ventana Medical Systems, Tucson, AZ, USA). Each step of the Ventana DABMap detection kit procedure was optimized on the Discovery XT instrument and preset. Antigen retrieval of tissue sections was performed with enzyme for CD68 and with heat for α-SMA. The sections were counterstained with haematoxylin. Slides of the negative control without the primary antibody and those of the positive control were processed in parallel. Thickness of smooth muscle layer of bronchioles The thickness of the bronchiolar smooth muscle layer was quantified by measuring the thickness of α-SMA positive layer at 4 points in randomly selected bronchiolar cross sections of the smallest diameters, 250–500 µm. The mean of the measurements in each groups was recorded. Fig. 1. Gastro-duodenal contents reflux model. A single serosal suture between the esophagus and jejunum was added after the esophagojejunostomy. B, Bile duct; E, esophagus; F, fore stomach; G, glandular stomach; D, duodenum; J, jejunum. pH analysis of the esophageal and gastric contents Following euthanasia, pH of the esophageal and gastric contents was estimated using a Compact pH meter (Horiba, Kyoto, Japan). Statistical analysis Absolute lung weights, the pH of esophageal and gastric contents, and the thickness of the smooth muscle layer of bronchioles are expressed as mean ± SE. Student’s t-test or Welch’s t-test were used for comparisons. P<0.05 was considered statistically significant. Results pH of the esophageal and gastric contents The pH of the gastric contents in the reflux rats was 3.75 ± 0.19 after 10 weeks and 4.11 ± 0.34 after 20 weeks compared to control rat values of 4.06 ± 0.30 after 10 weeks and 4.32 ± 0.49 after 20 weeks. The pH of the esophageal contents in the reflux rats was 7.07 ± 0.11 after 10 weeks and 6.48 ± 0.08 after 20 weeks. However, no comparable pH measurements were made in control rats at 10 and 20 weeks due to the small volume of esophageal contents in these animals. There were no significant differences in the pH of the stomach contents between the groups (Table 1). 144 K. Oue, ET AL. Table 1. Esophageal and gastric content pH Gastric pH Esophageal pH Control (10 w) Reflux model (10 w) Control (20 w) Reflux model (20 w) 4.06 ± 0.30 7.29 ± 0.06 3.75 ± 0.19 n.d. 4.32 ± 0.49 6.40 ± 0.08 4.11 ± 0.34 n.d. The data are shown as the mean ± SE. n.d., not determined; due to very little fluid in the esophagus of control animals. Table 2. Lung weights R. lung (g) L. lung (g) Control (10 w) Reflux model (10 w) Control (20 w) Reflux model (20 w) 0.812 ± 0.03 0.440 ± 0.02 0.822 ± 0.05 0.466 ± 0.04 0.864 ± 0.03 0.467 ± 0.01 0.854 ± 0.11 0.536 ± 0.09 The data are shown as the mean ± SE. Bilateral absolute lung weights Bilateral absolute lung weights are summarized in Table 2. At both 10 and 20 weeks, no significant increase of bilateral absolute lung weights from both control rats and reflux rats were noted. However, the left lung weights from reflux rats at 20 weeks were slightly higher than those of the controls. The lung weights appeared to correlate with the degree of inflammatory cell infiltrates in the lungs of the reflux animals. Macroscopic and under-loupe findings Both lungs of the reflux animals were partially consolidated compared to those of the control animals at 10 and 20 weeks following surgery (Fig. 2). HE-stained sections showed several areas of densely stained inflammatory cell infiltrates, and atelectasis was detected in the bilateral lung fields of the reflux animals (Fig. 3). These areas grew in size in a time-dependent manner. Microscopic findings Low-power views of both lungs showed partial consolidation in areas surrounding the bronchi and bronchioles of the reflux animals (Fig. 4a). High-power views of the lung alveolar spaces of reflux animals showed partly severe lymphocytic and neutrophilic infiltrates, macrophages, and multinucleated giant cells within the alveolar space (Fig. 4b and 4c). In addition, bile acids and food contents were occasionally found within multinucleated giant cells. In severe cases, the bronchioles were partially plugged with neutrophilic exudates (Fig. 4c and 4d). Neither congestion nor pulmonary edema was detected in any animal. A markedly increased number of goblet cells positive for PAS-Alcian blue and an increased number of peribronchiolar blood vessels were detected in the reflux animals compared to the control animals (Fig. 5a–d). PAS-Alcian blue staining showed a time-dependent increase in the number of goblet cells. Goblet cells accounted for a significantly greater number of bronchial and bronchiolar epithelial cells at 20 weeks after surgery than at 10 weeks. We detected strong (3+) proliferation of goblet cells, i.e., goblet cell hyperplasia, in the bronchial and bronchiolar epithelium in three of seven specimens at 10 weeks and all seven specimens at 20 weeks in the left lung, and five of seven specimens at 10 weeks and all seven specimens at 20 weeks in the right lung (Table 3). The thickness of the smooth muscle layer of the bronchiole in the bilateral lungs of the reflux animals was significantly greater than that of the control animals at 10 and 20 weeks after surgery (Table 4). Bronchioles of 250–500 µm representatives of the smallest diameters in the reflux and control animals are shown in Fig. 6. We also observed that many reflux animals had BO-like lesions, characterized by peribronchiolar lymphocytic infiltrates and luminal narrowing of the respiratory bronchioles due to polypoid granulation tissue composed of numerous macrophages positive for CD68, multinucleated giant cells, and spindle cells (Fig. 7a and 7b). Fibrous connective tissue, partially positive for Azan stain, was observed in the granulation tissue (Fig. 7c). BO-like RESPIRATORY DISORDERS AND MICROASPIRATION IN RATS 145 Fig. 2. Macroscopic views of lungs at 20 weeks postoperatively. a) sham-operated animal, b) reflux animal. Gross figure shows that the color of bilateral lungs in the reflux animals is markedly red and bilateral lungs in the reflux animals are partly consolidated compared to those of the control animals. Fig. 3. Loupe views of HE sections. a–c, left lung; d–f, right lung; a and d, control animal at 20 weeks; b and e, reflux animal at 10 weeks postoperatively; c and f, reflux animal at 20 weeks postoperatively. Several parts with dense inflammatory cell infiltrates were detected in bilateral lung fields. These infiltrates were more severe at 20 weeks than at 10 weeks after operation. Fig. 4. Microscopic findings in HE sections from the reflux animals at 20 weeks. a, Lowpower view; b–d, high-power view. a) Severe lymphocytic and neutrophilic infiltrates, macrophages, and multinucleated giant cells were detected. b) Many multinucleated giant cells were found in the alveolar spaces. c and d) Many neutrophilic infiltrates were found within the alveolar spaces and in the small airway. 146 K. OUE, ET AL. Fig. 5. Goblet hyperplasia and an increased number of blood vessels developed in the reflux animals at 20 weeks. a and d, HE staining; b and e, PAS-Alcian blue staining; c, and f, immunohistochemical staining of α-SMA; a–c, control animal; d–f, reflux animal. Marked goblet cell hyperplasia positive for PAS-Alcian blue was observed in the reflux animals compared to the control animals (a, b, d, e). Not only bronchiolar smooth muscle layer but also peribronchiolar blood vessels were positive for α-SMA (c and f). An increased number of blood vessels, and inflammatory cell infiltrates were also found in the reflux animals (a, c, d, f). Fig. 6. Comparison of the thickness of the bronchiolar smooth muscle layer of reflux animals and controls at 20 weeks after surgery. a) Control animal, b) Reflux model. We measured the thickness at 4 points in each cross-section of the smallest diameter bronchioles, 250–500 µm. The thickness of the smooth muscle layer in the reflux animals was significantly greater than in the controls. Fig. 7. Bronchiolitis obliterans-like lesions developed in the reflux animals at 20 weeks. a) HE staining, b) CD68, c) Azan staining. Bronchiolitis obliterans-like lesions comprising granulation tissue with macrophages positive for CD68, spindle cells, and a multinucleated giant cell in the lumen of respiratory bronchioles were observed in the reflux animals (a and b). Partially fibrous connective tissue positive for Azan staining was noted in the granulation tissue (c). 147 RESPIRATORY DISORDERS AND MICROASPIRATION IN RATS Table 3. Incidence of bronchiolitis obliterans-like lesion and goblet cell metaplasia in control and reflux animals Bronchiolitis obliterans-like lesion Control (10 w) Control (20 w) Reflux model (10 w) Reflux model (20 w) L. lung R. lung 0/7 0/7 4/7 7/7 0/7 0/7 2/7 7/7 Goblet cell metaplasia (3+) L. lung R. lung 0/7 0/7 3/7 7/7 0/7 0/7 5/7 6/7 Table 4. Thickness of smooth muscle layer Diameter of bronchiole Control (10 w) Control (20 w) Reflux model (10 w) Reflux model (20 w) L. lung R. lung 290.0 ± 24.2 313.7 ± 16.4 335.2 ± 16.7 295.0 ± 11.3 300.4 ± 10.0 297.5 ± 12.7 329.1 ± 21.6 321.6 ± 20.2 Thickness of smooth muscle bundles L. lung 12.7 ± 0.47* 10.9 ± 0.31** 17.5 ± 0.98* 17.3 ± 1.14** R. lung 11.7 ± 0.52* 9.52 ± 0.43** 21.3 ± 0.88* 15.3 ± 0.58** Data are shown as the mean ± SE. There were no significant differences among the groups in the thickness of the smooth muscle layer in the smallest diameter bronchioles examined. The mean thickness of bronchiolar smooth muscle layer was significantly greater in the reflux animals than in the control animals (* and **, P<0.0001; Student’s t-test). lesions were detected in four of seven specimens at 10 weeks and in all seven specimens at 20 weeks in the left lung, and in two of seven specimens at 10 weeks and all seven specimens at 20 weeks in the right lung (Table 3). Discussion We detected bronchopneumonia with foreign body reaction, namely aspiration pneumonia and peribronchial atelectasis and fibrosis following purulent inflammation with severe peribronchiolar neutrophilic and lymphocytic infiltrates in our reflux model. Goblet cell hyperplasia, prominence of blood vessels, and increased thickness of the smooth muscle layer were also detected in association with the continuous chronic inflammatory stimulation of GER. The most important findings of the present study were BO-like lesions characterized by luminal narrowing of the respiratory bronchioles due to polypoid granulation tissue composed of numerous macrophages, multinucleated giant cells, and spindle cells. Based on the abovementioned results, we hypothesize that GER may play an important role in the exacerbation of various respiratory diseases, especially asthma, COPD, and BOS following lung transplantation. In human asthma cases, GER appears to be associated with airway inflammation and has been recognized as an important causative factor in asthma attacks [21, 23]. However, the mechanism by which GER may provoke airway inflammation is doubtful. A key role seems to be played by the vagally-mediated neurogenic reflex or by the microaspirated refluxate that probably mediates airway inflammation [9, 24]. Irrespective of the active mechanism, airway inflammation in GER can be the linkage by which GER eventually exacerbates asthma. A recent study showed that GER associated with asthma is characterized by an increase in the numbers of eosinophils and neutrophils, while GER alone presents a neutrophilic pattern of inflammation. In addition, GER appears to exacerbate already existing oxidative stress [10]. These findings are consistent with the pattern of aspiration pneumonia with severe peribronchiolar neutrophilic and lymphocytic infiltrates found in the present animal model. Therefore, the inflammation caused by GER can be a causative factor of exacerbation of asthma. Moreover, it has also been reported that a marked increase in the goblet cells in the airways is a characteristic feature of patients with bronchial asthma who have 148 K. Oue, ET AL. died of severe acute attacks. The discovery of goblet cell hyperplasia could be used as a marker to identify patients with bronchial asthma who are at risk of severe attacks [1]. Considering these results, the goblet cell hyperplasia observed in the present study may also play a role in worsening asthma in human cases. COPD exacerbations are characterized by acute and chronic deterioration in respiration [3, 7]. One of the most common causes of COPD exacerbations is tracheobronchial infection. The most frequent route for bacterial infection of the tracheobronchial tree is the silent aspiration of oropharyngeal secretions [36]. Studies on the relationship between the swallowing function and GERD have revealed that subjects presenting with cough and GERD have significantly reduced laryngopharyngeal sensitivity, potentially resulting in an increased risk of aspiration via the impairment of the swallowing reflex [32]. A recent study suggested that swallowing abnormalities, probably via GERD comorbidity, were associated with frequent COPD exacerbations [37]. Our previous study using the same rat reflux model as the present study showed that the reflux of gastro-duodenal contents causes severe laryngitis [30]. Inflammation of the larynx must play a role in impairment of the swallowing reflex. BOS is a major long-term complication and a leading cause of death after lung transplantation; it affects 50– 70% of transplant recipients [4, 6, 25]. The histological hallmark of BOS is BO [8]. BOS was originally defined as a decrease in forced expiratory volume in 1 second (FEV 1) [13]. In the present study, we detected BO-like lesions associated with repetitive microaspiration caused by GER. These lesions may play an important role in exacerbation of FEV 1 subsequent to COPD exacerbations, unlike true constrictive BO that is fused to the bronchiolar wall and obliterates the lumen. In a recent experimental study, Li et al. [29] reported histological evidence consistent with BO development in lung allografts after inducing chronic gastric fluid aspiration in a rat model that utilized immunosuppression to avoid acute rejection. However, the BO-like lesions observed in the present reflux animal lungs did not result from lung transplants or cyclosporine treatments. Thus, as previously suggested by Li et al., our results imply that GER plays an important role in BO-like lesion develop- ment and that alloimmune injury following bone marrow transplantation may promote BO development. Another issue to be investigated with regard to refluxate in GER involves the determiation of the degree of harm and importance of gastric juice and bile acids in the pathogenesis of BO. The refluxates of the reflux animals in the present study contained not only gastric juices but also duodenal contents including bile acids. D’Ovidio et al. examined bile acids in the bronchoalveolar lavage fluid of 120 post-transplant patients in a cross-sectional study and found a 17% prevalence of elevated bile acid concentrations. Furthermore, the highest concentrations were found in patients with early onset BOS [18]. Bile aspiration secondary to duodenoGER has been associated with severe pulmonary injury. Cytotoxicity may result in disruption of cellular membranes or alteration of cellular cationic permeability depending on the bile acid concentration [27, 33, 40]. These findings suggest that refluxates, including bile acids, play an important role in BO pathogenesis in lung transplant patients. In summary, we detected bronchopneumonia with foreign body reaction and peribronchial atelectasis and fibrosis in conjunction with purulent inflammation with severe peribronchiolar neutrophilic and lymphocytic infiltrates in our reflux-induced rats. We also noted goblet cells and smooth muscle hyperplasia. From these findings, we speculate that repetitive microaspiration due to GER contributes to the exacerbation of various respiratory diseases, especially asthma and COPD. BO-like lesions were also observed in reflux animal lungs without lung transplantation or cyclosporine treatment. These findings confirm that GER including bile acids plays an important role in the development of BO as a nonimmune-mediated factor in lung transplant patients. The gastro-duodenal contents reflux model was originally used in studies of Barrett’s esophagus; however, the model is a good tool for studying the development of extraesophageal syndromes and respiratory disorders based on GER. Acknowledgment We thank Mr. Michiharu Nasu for excellent technical assistance. RESPIRATORY DISORDERS AND MICROASPIRATION IN RATS References 1. Aikawa, T., Shimura, S., Sasaki, H., Ebina, M., and Takishima, T. 1992. Marked goblet cell hyperplasia with mucus accumulation in the airways of patients who died of severe acute asthma attack. Chest 101: 916–921. 2. Alexander, J.A., Hunt, L.W., and Patel, A.M. 2000. Prevalence, pathophysiology, and treatment of subjects with asthma and gastroesophageal reflux disease. Mayo Clin. Proc. 75: 1055–1063. 3. Anthonisen, N.R., Manfreda, J., Warren, C.P., Hershfield, E.S., Harding, G.K., and Nelson, N.A. 1987. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann. Intern. Med. 106: 196–204. 4. Arcasoy, S.M. and Kotloff, R.M. 1999. Lung transplantation. N. Engl. J. Med. 340: 1081–1091. 5. Berkowitz, N., Schulman, L.L., McGregor, C., and Markowitz, D. 1995. Gastroparesis after lung transplantation. Potential role in postoperative respiratory complications. Chest 108: 1602–1607. 6. Boehler, A. and Estenne, M. 2000. Obliterative bronchiolitis after lung transplantation. Curr. Opin. Pulm. Med. 6: 133– 139. 7. Burge, S. and Wedzicha, J.A. 2003. COPD exacerbations: definitions and classifications. Eur. Respir. J. 21: 46–53S. 8. Burke, C.M., Theodore, J., Dawkins, K.D., Van Kessel, A., Jamieson, S.W., and Oyer, P.E. 1984. Post-transplant obliterative bronchiolitis and other late lung sequelae in human heart-lung transplantation. Chest 86: 824–829. 9. Canning, B.J. 2001. Role of nerves in asthmatic inflammation and potential influence of gastroesophageal reflux disease. Am. J. Med. 111: 13–17S. 10. Carpagnano, G.E., Resta, O., Ventura, M.T., Amoruso, A.C., Di, Gioia, G., Giliberti, T., Refolo, L., and Foschino-Barbaro, M.P. 2006. Airway inflammation in subjects with gastrooesophageal reflux and gastro-oesophageal reflux-related asthma. J. Intern. Med. 259: 323–331. 11. Chen, K.H., Mukaisho, K., Ling, Z.Q., Shimomura, A., Sugihara, H., and Hattori, T. 2007. Association between duodenal contents reflux and squamous cell carcinoma— Establishment of an esophageal cancer cell line derived from the metastatic tumor in a rat reflux model. Anticancer Res. 27: 175–181. 12. Chen, K.H., Mukaisho, K., Sugihara, H., Araki, Y., Yamamoto, G., and Hattori, T. 2007. High animal-fat intake changes the bileacid composition of bile juice and enhances the development of Barrett’s oesophagus and oesophageal adenocarcinoma in a rat duodenal-contents reflux model. Cancer Sci. 98: 1683–1688. 13. Cooper, J.D., Billingham, M., Egan, T., Hertz, M.I., Higenbottam, T., Lynch, J., Mauer, J., Paradis, I., Patterson, G.A., and Smith, C. 1993. A working formulation for the standardization of nomenclature and for clinical staging of chronic dysfunction in lung allografts: International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 12: 713–716. 14. Cuttitta, G., Cibella, F., Visconti, A., Scichilone, N., Bellia, V., and Bonsignore, G. 2000. Spontaneous gastroesophageal 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 149 reflux and airway patency during the night in adult asthmatics. Am. J. Respir. Crit. Care Med. 161: 177–181. Davis, R.D. Jr., Lau, C.L., Eubanks, S., Messier, R.H., Hadjiliadis, D., Steele, M.P., and Palmer, S.M. 2003. Improved lung allograft function after fundoplication in patients with gastroesophageal reflux disease undergoing lung transplantation. J. Thorac. Cardiovasc. Surg. 125: 533–542. Dent, J., El-Serag, H.B., Wallander, M.A., and Johansson, S. 2005. Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut 54: 710–717. D’Ovidio, F., Mura, M., Ridsdale, R., Takahashi, H., Waddell, T.K., Hutcheon, M., Hadjiliadis, D., Singer, L.G., Pierre, A., Chaparro, C., Gutierrez, C., Miller, L., Darling, G., Liu, M., Post, M., and Keshavjee, S. 2006. The effect of reflux and bile acid aspiration on the lung allograft and its surfactant and innate immunity molecules SP-A and SP-D. Am. J. Transplant. 6: 1930–1938. D’Ovidio, F., Mura, M., Tsang, M., Waddell, T.K., Hutcheon, M.A., Singer, L.G., Hadjiliadis, D., Chaparro, C., Gutierrez, C., Pierre, A., Darling, G., Liu, M., and Keshavjee, S. 2005. Bile acid aspiration and the development of bronchiolitis obliterans after lung transplantation. J. Thorac. Cardiovasc. Surg. 129: 1144–1152. Feigelson, J., Girault, F., and Pecau, Y. 1987. Gastrooesophageal reflux and esophagitis in cystic fibrosis. Acta Paediatr. Scand. 76: 989–990. Field, S.K., Evans, J.A., and Price, L.M. 1998. The effects of acid perfusion of the esophagus on ventilation and respiratory sensation. Am. J. Respir. Crit. Care Med. 157: 1058–1062. Garcia, G., Adler, M., and Humbert, M. 2003. Difficult asthma. Allergy 58: 114–121. Hadjiliadis, D., Davis, R.D., Steele, M.P., Messier, R.H., Lau, C.L., and Eubanks, S.S. 2003. Gastroesophageal reflux disease in lung transplant recipients. Clin. Transplant. 17: 363–368. Harding, S.M. 2005. Gastroesophageal reflux: a potential asthma trigger. Immunol. Allergy Clin. North Am. 25: 131–148. Harmanci, E., Entok, E., Metintas, M., Vardareli, E., and Elbek, O. 2001. Gastroesophageal reflux in the patients with asthma. Allergol. Immunopathol. 29: 123–128. Hertz, M.I., Taylor, D.O., Trulock, E.P., Boucek, M.M., Mohacsi, P.J., Edwards, L.B., and Keck, B.M. 2002. The registry of the International Society for Heart and Lung Transplantation: nineteenth official report-2002. J. Heart Lung Transplant. 21: 950–970. Higo, T., Mukaisho, K., Ling, Z.Q., Oue, K., Chen, K.H., Araki, Y., Sugihara, H., Yamamoto, G., and Hattori, T. 2009. An animal model of intrinsic dental erosion caused by gastro-oesophageal reflux disease. Oral Dis. 15: 360–365. Hills, B.A. 1985. Gastric mucosal barrier: stabilization of hydrophobic lining to the stomach by mucus. Am. J. Physiol. 249: G342–349. Hungin, A.P., Raghunath, A.S., and Wiklund, I. 2005. Beyond heartburn: a systematic review of the extraoesophageal spectrum of reflux-induced disease. Fam. Pract. 150 K. Oue, ET AL. 22: 591–603. 29. Li, B., Hartwig, M.G., Appel, J.Z., Bush, E.L., Balsara, K.R., Holzknecht, Z.E., Collins, B.H., Howell, D.N., Parker, W., Lin, S.S., and Davis, R.D. 2008. Chronic aspiration of gastric fluid induces the development of obliterative bronchiolitis in rat lung transplants. Am. J. Transplant. 8: 1614–1621. 30. Ling, Z.Q., Mukaisho, K., Hidaka, M., Chen, K.H., Yamamoto, G., and Hattori, T. 2007. Duodenal contents reflux-induced laryngitis in rats: possible mechanism of enhancement of the causative factors in laryngeal carcinogenesis. Ann. Otol. Rhinol. Laryngol. 116: 471– 478. 31. Palmer, S.M., Miralles, A.P., Howell, D.N., Brazer, S.R., Tapson, V.F., and Davis, R.D. 2000. Gastroesophageal reflux as a reversible cause of allograft dysfunction after lung transplantation. Chest 118: 1214–1217. 32. Phua, S.Y., McGarvey, L.P., Ngu, M.C., and Ing, A.J. 2005. Patients with gastrooesophageal reflux disease and cough have impaired laryngopharyngeal mechanosensitivity. Thorax 60: 488–491. 33. Porembka, D.T., Kier, A., Sehlhorst, S., Boyce, S., Orlowski, J.P., and Davis, K. Jr. 1993. The pathophysiologic changes following bile aspiration in a porcine lung model. Chest 104: 919–924. 34. Reid, K.R., McKenzie, F.N., Menkis, A.H., Novick, R.J., Pflugfelder, P.W., Kostuk, W.J., and Ahmad, D. 1990. Importance of chronic aspiration in recipients of heart-lung transplants. Lancet 336: 206–208. 35. Rinaldi, M., Martinelli, L., Volpato, G., Pederzolli, C., Silvestri, M., Pederzolli, N., Arbustini, E., and Vigano, M. 1995. Gastro-esophageal reflux as cause of obliterative 36. 37. 38. 39. 40. 41. 42. 43. bronchiolitis: a case report. Transplant. Proc. 27: 2006– 2007. Sethi, S., Maloney, J., Grove, L., Wrona, C., and Berenson, C.S. 2006. Airway inflammation and bronchial bacterial colonization in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 173: 991–998. Terada, K., Muro, S., Ohara, T., Kudo, M., Ogawa, E., Hoshino, Y., Hirai, T., Niimi, A., Chin, K., and Mishima, M. 2010. Abnormal swallowing reflex and COPD exacerbations. Chest 137: 326–332. Terada, K., Muro, S., Sato, S., Ohara, T., Haruna, A., Marumo, S., Kinose, D., Ogawa, E., Hoshino, Y., Niimi, A., Terada, T., and Mishima, M. 2008. Impact of gastrooesophageal reflux disease symptoms on COPD exacerbation. Thorax 63: 951–955. Tobin, R.W., Pope, C.E. 2nd., Pellegrini, C.A., Emond, M.J., Sillery, J., and Raghu, G. 1998. Increased prevalence of gastroesophageal reflux in patients with idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 158: 1804–1808. Vaezi, M.F. and Richter, J.E. 2001. Duodenogastroesophageal reflux and methods to monitor nonacidic reflux. Am. J. Med. 111: 160–168S. Vakil, N. 2006. The frontiers of reflux disease. Dig. Dis. Sci. 51: 1887–1895. Vakil, N., van. Zanten, S.V., Kahrilas, P., Dent, J., Jones, R., and Global Consensus Group. 2006. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am. J. Gastroenterol. 101: 1900–1920. Young, L.R., Hadjiliadis, D., Davis, R.D., and Palmer, S.M. 2003. Lung transplantation exacerbates gastroesophageal reflux disease. Chest 124: 1689–1693.