Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
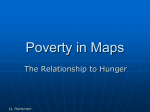
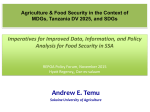
AGEC 340: International Economic Development Course slides for week 2 (Jan. 19 & 21) Poverty and Income Growth* • Your background & objectives for this class • A side note on the textbook, for those using it • Measuring poverty: -- Poverty, real income and income growth -- Poverty, health and nutrition * In the textbook, this material is covered in Chapters 1 & 2. Your background and objectives A side note on the textbook… what fact discussed in Chapter 1 is already outdated? ? Click image to read the article…or click here for the latest data: www.fao.org/worldfoodsituation/FoodPricesIndex What does “poverty” (or wealth) really mean? To measure and compare over all people, we add up all goods and services per person: Total production: Gross Domestic Product (GDP) = total value of activity done in a country Gross National Product (GNP) = total value of activity by a country’s people Production ≈ income, so: = Gross National Income (GNI) Measuring Poverty: The Textbook Picture (Table 1-1, p. 19) Gross National Income per Capita in Selected Countries, 2002 Source: World Bank, World Development Indicators 2002. How best to compare income levels across countries? We must convert values from local currency into a common measurement unit (US dollars), but how? – if we use market exchange rates (like Table 1-1) we measure income in terms of the goods they can buy in other countries but local services prices differ across countries, and currency exchange rates fluctuate over time, so… – we prefer to use purchasing power parity (PPP) prices measures income in terms of the goods they can buy in their own country for example, $1 at PPP prices ≈ about one day’s food Poor places have lower incomes at market exchange rates than in PPP terms Income per capita in the five poorest countries, 2007 Sorted by GDP in US$ at Market Exchange Rates Sorted by GDP in US$ at Purchasing Power Parity Prices Burundi 127 Burundi 705 D.R.Congo 161 Malawi 750 Guinea-Bissau 204 Guinea-Bissau 780 Ethiopia 206 Tanzania 869 Gambia 239 D.R.Congo 893 The D.R. Congo has a particularly low market exchange rate, so is less poor when measured in PPP terms Source: Calculated from IMF, International Financial Statistics. Rich places have higher incomes at market exchange rates than in PPP terms Income per capita in ten richest countries, 2007 Sorted by GDP in US$ at Market Exchange Rates Sorted by GDP in US$ at Purchasing Power Parity Prices Luxembourg Norway Qatar Iceland Ireland Denmark Switzerland United Kingdom Sweden United States Luxembourg Ireland Norway United States Iceland Hong Kong Switzerland Qatar Austria Denmark 102,284 79,154 70,754 62,976 58,883 57,035 56,711 47,300 47,069 46,780 87,400 47,169 47,098 44,765 41,680 41,614 40,590 38,672 38,478 38,438 The U.S. is 10th at market exchange rates, but 4th in PPP terms Source: Calculated from IMF, International Financial Statistics. How is this income earned? Who earns it? Who produces more per worker: farmers or other workers? …in poor countries? …in the U.S.? What about poverty? …Commonly defined as <$1/day, in PPP terms Number of people below $1/day poverty line (in millions) Pct. of people below $1/day poverty line (in %) Urban Rural Total Urban Rural Total 1993 241.5 1,038.1 1,279.6 13.84 36.64 27.95 1996 263.8 934.3 1,198.2 13.92 32.15 24.96 1999 282.3 949.0 1,231.3 13.76 32.18 24.65 2002 291.4 890.0 1,181.4 13.18 29.74 22.73 Source: Martin Ravallion, Shaohua Chen and Prem Sangraula, “New Evidence on the Urbanization of Global Poverty.” World Bank Policy Research Working Paper 4199, April 2007. The number of urban poor has risen due to rural-urban migration, but the prevalence of poverty in both rural and urban areas has declined. Poverty and Health: Our textbook picture Has health improved over time? Life Expectancy at Birth, 1950-2000 75 70 Europe 65 Lat.Am.&Car. 60 World 55 India 50 Pakistan 45 Bangladesh Africa 40 35 1950- 1955- 1960- 1965- 1970- 1975- 1980- 1985- 1990- 19951955 1960 1965 1970 1975 1980 1985 1990 1995 2000 Source: Computed from UN Population Division, 2004 <http://esa.un.org/unpp> Slide 12 How does health change with income? Source: Angus Deaton, “Health, Inequality, and Economic Development.” Journal of Economic Literature, XLI(1), March 2003: 113–158. Note: Circle size is proportional to population. Slide 13 Poverty and Health To see this relationship, there’s nothing better than gapminder’s view of the world: Click image to open www.gapminder.org/world. Now, let’s add in nutrition: Our textbook picture Note: availability = production ± trade Malnutrition is more than just calories! Undernutrition is falling, except in Africa Data Trends, projections and MDGs for prevalence andof projections childhood underweighton children underunderweight, 5, 1995-2015 1995-2015 30 25 Percent of children 20 15 10 5 0 Africa Asia 1995 2000 Lat. Am. & Caribbean 2005 Developing Countries 2010 2015 World MDG Source: UN Standing Committee on Nutrition (2004), Fifth Report on the World Nutrition Situation. New York: UN SCN. Note: Data show estimated percentage of children aged 0-5 who are underweight, defined as <2 s.d. below median NCHS weight for age. Slide 17 Children being underweight from too little food is still the world’s worst health threat Worldwide disease burden from m ajor risk factors, 2000 Underweight Unsafe sex Blood pressure Water & sanitation Tobacco Indoor smoke from fuels Cholesterol Alcohol Zinc deficiency Vitamin A deficiency Iron deficiency Low fruit and vegetable intake Overweight Annual loss of disability-adjusted life-years (millions of DALYs) 0 20 40 60 80 100 120 Source: WHO (2002), World Health Report 2002, available online at w ww .w ho.int. 140 Slide 18 The shortfall leading to underweight occurs between 4 and 14 months of age Mean weight-for-age z scores, relative to the NCHS reference Latin America Africa Asia Source: R. Shrimpton et al., 2001. “Worldwide Timing of Growth Faltering: Implications for Nutritional Interventions” Pediatrics 107:e75. Reprinted from W.A. Masters (2005), “Paying for Prosperity. JIA 58(2): 35-64. Slide 19 Being underweight contributes to many diseases Attribution of disease burden to major risk factors in high-mortality developing countries Risk factor % DALYs Underweight 14.9 Unsafe sex 10.2 Unsafe water, sanitation and hygiene 5.5 Indoor smoke from solid fuels 3.7 Zinc deficiency 3.2 Iron deficiency 3.1 Vitamin A deficiency 3.0 Blood pressure 2.5 Tobacco 2.0 Cholesterol 1.9 Subtotal for under-nutrition 24.3 Disease or injury HIV/AIDS Lower respiratory infections Diarrhoeal diseases Childhood cluster diseases Low birth weight Malaria Unipolar depressive disorders Ischaemic heart disease Tuberculosis Road traffic injury % DALYs 9.0 8.2 6.3 5.5 5.0 4.9 3.1 3.0 2.9 2.0 Notes: Arrows are roughly proportional to attribution rates. Risk factors and diseases associated with under-nutrition are in italics. The selected risk factors cause diseases in addition to those relationships illustrated, and additional risk factors are also important for the diseases illustrated. Data shown are totals for 69 countries defined by the WHO as having both high child mortality and high adult mortality. Source: WHO (2002), World Health Report 2002, Annex Table 14 (p. 232), www.who.int/whr. Reprinted from W.A. Masters (2005), “Paying for Prosperity. Journal of Intl. Affairs 58(2): 35-64. Slide 20 Risk factors vary by income level Contribution to global burden of disease by risk factor and region Slide 21 Some conclusions on poverty, health and nutrition • Nutrition and health have improved greatly in recent years, in all regions except Africa • …but undernutrition remains the world’s greatest single health risk factor, by affecting preschool children. • The recent food price spike could have worsened malnutrition and health, but income matters even more. • Up next: how prices and income affect consumption