Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
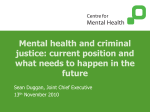
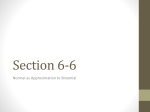
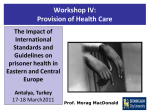
'UNDERSTANDING HEALTH NEEDS AND INEQUALITY IN HEALTH AND JUSTICE' By Dr. Éamonn O’Moore, Director for Health & Justice, Public Health England & Director WHO Collaborating Centre for Health in Prisons Programme, (European Region). and Dr Autilia Newton Deputy Director Health & Justice, PHE Hampton Hospital, September 12th, 2014 PHE Mission Statement on Health & Justice • Public Health England (PHE) will work in partnership with health & social care commissioners , service providers, academic & third sector organisations and international partners to identify and meet the health & social care needs of people in prisons and other prescribed detention settings, as well as those in contact with the criminal justice system (CJS) in the community. . • PHE will aim to reduce health inequalities, support people in living healthier lives, and ensure the continuity of care in the community. 2 Rampton Hospital, September 12th, 2014 Health Inequalities & CJS • Health inequalities experienced by people in contact with the criminal justice system (CJS) are well above the average experienced by the wider community. • As well as those in a custodial setting, this includes offenders serving community sentences, those who are in the community on licence and or ‘known to the police’. • Evidence that this group of people suffer from multiple and complex health issues, including mental and physical health problems, learning difficulties, substance misuse and increased risk of premature mortality. • These underlying health issues are often exacerbated by difficulties in accessing the full range of health and social care services available in the local community. 4. Rampton Hospital, September 12th, 2014 ‘Underserved’ NOT ‘hard to reach’ 4 • People in PPDs often described as belonging to ‘hard-to-reach’ populations; • This is NOT true- more accurately described as ‘under-served’ both in prisons and in the community; • ‘Hard-to-reach’ implies some active withdrawal by population whereas ‘underserved’ describes situation where services fail to meet needs of population in appropriate ways. • Need to stop blaming the patient for being ‘difficult’ and recognise instead difficult circumstances (personal, social and cultural) in which patient often lives as being a barrier to their accessing ‘conventionally delivered services’. . Rampton Hospital, September 12th, 2014 Role of PHE in Health & Justice: • PHE will gather and provide evidence and intelligence to inform and support the work of local and national commissioners and service providers; • PHE will provide expertise at local, national & international level (in our role as UK CC for WHO HIPP) on a broad range of health protection, health promotion and disease prevention activities working in close partnership with local commissioners and service providers. • PHE will support partners, including commissioners and providers of health and social care, in the development of care pathways which account for the movement of people around the detention estate and between prescribed detention settings and the community. 5 Rampton Hospital, September 12th, 2014 PHE Resources for Health & Justice: • PHE also has a dedicated resource to support work on understanding and managing the health needs of people in contact with the criminal justice system. • The national team sits within the Health & Wellbeing Directorate; • Ten Health & Justice Public Health Specialists are based in Public Health England Centres, working in the Operations Directorate, and ‘man-marking’ the ten NHS England AT Health & Justice Lead Commissioners; • These with the national team form the Health & Justice Network; . Rampton Hospital, September 12th, 2014 PHE Resources for Health & Justice: cont’d • A specialised Health Protection Prison Network composed of HP staff from each PHE Centre and chaired by the H&J DD, compliments the H&J Network and covers the specialised area of HP • The H&J DD works across 2 Directorates: Operations & Well Being, co-ordinating with WB and leading the H&J agenda across Ops • These resources within both NHSE and PHE at national and local level allow for effective horizontal and vertical integration within organisations and between organisations. 7 Rampton Hospital, September 12th, 2014 PHE Regions & Centres 8 Rampton Hospital, September 12th, 2014 Criminal Justice Estate- England & Wales 9 Rampton Hospital, September 12th, 2014 Prison Population Rate per 100,00 globally Rampton Hospital, September 12th, 2014 Population Factors 11 Rampton Hospital, September 12th, 2014 ‘Community Dividend’ for public health interventions in prison populations • Underserved populations passing through prison estate ~160,000 per year; • Often belong to wider social groups and networks contributing significantly to health inequalities generally; • Delivering health interventions in prisons not only benefits prisoners‘community dividend’ in addressing issues in underserved populations generally. 1.77 million individuals annually were dealt with by CJS; ~250K annually ~160K annually 12 Rampton Hospital, September 12th, 2014 Some examples… Hepatitis B vaccination programme in prison (started in 2003) has had a significant impact on the incidence of the infection amongst IDUs in England The opt-out BBVs policy has the potential to deliver the largest impact in the reduction of BBVs pathology, especially Hepatitis C , in England 13 Rampton Hospital, September 12th, 2014 Public Health Model for Health & Justice: 14 Rampton Hospital, September 12th, 2014 15 Balancing Act • A briefing for Directors of Public Health published Oct 2013 which suggests positive actions and approaches DsPH could use to tackle the health inequalities of people in contact with the criminal justice system residing in their local community; Rampton Hospital, September 12th, 2014 16 Higher Mortality Rates among people in • Data on all cause mortality contact with CJS among current and or ex-prisoners is difficult to identify and collect; • However, in jurisdictions where such collections are possible, dramatic differences are evident between current or former prisoners and general population in relation to all cause mortality as well as accidental death and suicide. • Data from the UK is shown as example. Rampton Hospital, September 12th, 2014 17 Substance Misuse Among People in Contact with CJS: Rampton Hospital, September 12th, 2014 Mortality Rates: Drug Related Death Rates Rampton Hospital, September 12th, 2014 19 Mortality Rates: Suicide • Suicide rates are higher in prison populations than among peers in the community. • WHO data shows a suicide rate which ranges from 0 (0.0%) to almost 300 (0.3%) per 100,000 prisoners, with an average of about 60 (0.06%) per 100,000 in the 47 WHO European Member States that belong to the Council of Europe. • Data from the UK is shown as an example. Rampton Hospital, September 12th, 2014 20 High prevalence of diseases: Mental Health Prisoners often have higher prevalence of mental health problems and behaviours, including personality disorder, depression and psychosis. Rampton Hospital, September 12th, 2014 21 Learning Disabilities Rampton Hospital, September 12th, 2014 Smoking Prevalence 22 Rampton Hospital, September 12th, 2014 Physical Health Needs: cont’d 23 Rampton Hospital, September 12th, 2014 24 Infectious Diseases: BBV/HIV infection • Many prison populations have high prevalence of infection with blood-borne viruses (BBVs) (Hepatitis B & C) and HIV due to large numbers of injecting drug users (IDUs) among incarcerated populations; • Some evidence of onward transmission of infection in some European states due to injecting of drugs, tattooing and unprotected sexual activityalthough definitive data is difficult to find. Rampton Hospital, September 12th, 2014 New commissioning context • Section 15 of the Health and Social Care Act 2012 gives the Secretary of State the power to require NHS England to commission certain services instead of CCGs. These include ‘services or facilities for persons who are detained in a prison or other accommodation of a prescribed description.’ • NHS England assumed these powers from April 1 2013. • NHS England is responsible for ensuring that services are commissioned to consistently high standards of quality across the country, promote the NHS Constitution and deliver the requirements of the Secretary of State’s Mandate and the section 7a agreement with the NHS England. 25 Rampton Hospital, September 12th, 2014 NHS Resources for Health & Justice 26 • NHS England is structured with a national team, 4 regions and 27 Area Teams (ATs). • Nine ATs and a regional team for London have been designated to support commissioning of preventive and public health services as set out in the Section 7a agreement with SoS, in respect of persons detained in prison, or in other secure accommodation. • The ATs and London regional team work with the NHS England national team. • Commissioning intentions and structures were published by NHS in ‘Securing Excellence in Commissioning for Offender Health’ published in February 2013. Rampton Hospital, September 12th, 2014 Benefits of new system • The rationalisation of a large number of local commissioners to one single national commissioner provides the opportunity to implement nationally consistent evidence-based commissioning specifications and quality standards appropriate to the patient population and integrated in community-based services. • The is an opportunity to improve the continuity of care as detainees move around the detention estate and / or back into communities. • There are significant opportunities to improve the health and wellbeing of people in detention and in turn, the wider community. 27 Rampton Hospital, September 12th, 2014 28 Rampton Hospital, September 12th, 2014 29 Public Health Outcome Indicators • Indicators directly related to offending behaviours: Rampton Hospital, September 12th, 2014 • Indicators relating to adult populations in contact with CJS (in custody & in the community) Care inside and ‘through the gate’ • Primary care services are the major health services that individual’s access in detention but specialist services including sexual health, drugs & alcohol, and mental health services are also provided according to need. • Such services provide a prime opportunity to deliver therapeutic and prevention services and to begin care which can be continued around the detention estate and into the community. • People in prison use primary care services at greater frequency and intensity than their peers in the community, especially young men. This is completely reversed on return to the community, where their use of services is much lower than that of their peers. • Challenge is to ensure care started inside continues ‘through the gate’. 30 Rampton Hospital, September 12th, 2014 Transforming Rehabilitation 1. Reconfiguration of the Prison Estate to create network of 70 Resettlement Prisons (short sentences & last 3 months) 2. Creation of National Probation Service 3. Tendering for rehabilitation providers in package areas who will operate ‘Through the Gate’ 4. Supervision extended to short sentences 6. New providers paid by their results 5. Providers will provide, and signpost to/work in partnership with, wider services to reduce reoffending Conclusions: • Public health challenges associated with detention settings are significant and increasing; • Prisons & other places of detention represent an opportunity to address health inequalities in these settings specifically and society generally. • Challenge to ensure that work commenced in prisons and other detention settings is appropriately continued on return to the community- avoid ‘cliff edge’; • In England, opportunity in new public health system and NHS to address these issues more effectively especially with advent of a single commissioner (NHS England) for all prescribed detention settings in England; • Health and Justice organisations must work in ‘co-production’ mode to ensure effective design & delivery of services in prisons and beyond the prison walls. 32 Rampton Hospital, September 12th, 2014