Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
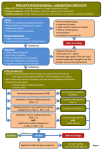
EUROPEAN UROLOGY 64 (2013) 228–243 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority – Collaborative Review – Benign Prostatic Hyperplasia Editorial by Herbert Lepor on pp. 244–246 of this issue Systematic Review of Combination Drug Therapy for Non-neurogenic Male Lower Urinary Tract Symptoms Claudius Füllhase a, Christopher Chapple b, Jean-Nicolas Cornu c, Cosimo De Nunzio d, Christian Gratzke a, Steven A. Kaplan e, Michael Marberger f, Francesco Montorsi g, Giacomo Novara h, Matthias Oelke i, Hartmut Porst j, Claus Roehrborn k, Christian Stief a, Kevin T. McVary l,* a Department of Urology, Klinikum Grosshadern, Ludwig-Maximilians-University, Munich, Germany; b Department of Urology, Royal Hallamshire Hospital, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK; c Department of Urology, Tenon Hospital, Assistance publique-Hopitaux de Paris, University Pierre et Marie Curie, Paris, France; d Department of Urology, Ospedale Sant’Andrea, University La Sapienza, Rome, Italy; e Iris Cantor Men’s Health Center, New York Presbyterian Hospital, and Weill Cornell Medical College, New York, NY, USA; f Department of Urology, Medical University of Vienna, Vienna, Austria; g Department of Urology, University Vita-Salute San Raffaele, Milan, Italy; h Department of Urology, University of Padua, Padua, Italy; i Department of Urology, Hannover Medical School, Hannover, Germany; j Private Institute of Urology/Andrology, Hamburg, Germany; k Department of Urology, University of Texas Southwestern Medical Center, Dallas, TX, USA; l Department of Urology, Southern Illinois University School of Medicine, Springfield, IL, USA Article info Abstract Article history: Accepted January 15, 2013 Published online ahead of print on January 25, 2013 Background: Several drugs are approved for the treatment of lower urinary tract symptoms (LUTS) in men, but these are mostly used by clinicians as monotherapies. The combination of different compounds, each of which targets a different aspect of LUTS, seems appealing. However, only few clinical trials have evaluated the effects of combination therapies. Objective: This systematic review analyzes the efficacy and adverse events of combination therapies for male LUTS. Evidence acquisition: PubMed and Cochrane databases were used to identify clinical trials and meta-analyses on male LUTS combination therapy. The search was restricted to studies of level of evidence 1b. A total of 49 papers published between January 1988 and March 2012 were identified. Evidence synthesis: The a1-adrenoceptor antagonist (a1-blocker)/5a-reductase inhibitor (5-ARI) combination provides the most data. This combination seems to be more efficacious in terms of several outcome variables in patients whose prostate volume is between 30 ml and 40 ml when treatment is maintained for >1 yr; when given for <1 yr, a1-blockers alone are just as effective. The combination of a1-blocker/5-ARI shows a slightly increased rate of adverse events. It remains unknown whether its safety and superiority over either drug as monotherapy are sustained after >6 yr. The a1-blocker/muscarinic receptor antagonist (antimuscarinic) combination was most frequently assessed as an add-on therapy to already existing a1-blocker therapy. Inconsistent data derive from heterogeneous study populations and different study designs. Currently, the a1-blocker/antimuscarinic combination appears to be a second-line add-on for patients with insufficient symptom relief after monotherapy. The combination seems to be safe in men with postvoid residual <200 ml. However, there are no trials >4 mo concerning safety and efficacy of this combination. The a1-blocker/phosphodiesterase type 5 inhibitor combination is a new treatment option with only preliminary reports. More studies are needed before definitive conclusions can be drawn. Conclusions: An a1-blocker/5-ARI combination is beneficial for patients whose prostate volume is between 30 ml and 40 ml when medical treatment is intended for >1 yr. Based on short-term follow-up studies, add-on of antimuscarinics to a1-blockers is an option when postvoid residual is <200 ml. # 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved. Keywords: Lower urinary tract symptoms Prostatic hyperplasia Adrenergic a1-receptor antagonists 5a-reductase inhibitors Muscarinic antagonists Please visit www.eu-acme.org/ europeanurology to read and answer questions on-line. The EU-ACME credits will then be attributed automatically. * Corresponding author. 301 N. 8th Street, PO Box 19665, Springfield, IL 62794-9665, USA. Tel. +217-545-8000; Fax: +217-545-7305. E-mail address: [email protected] (K.T. McVary). 0302-2838/$ – see back matter # 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.eururo.2013.01.018 EUROPEAN UROLOGY 64 (2013) 228–243 1. Introduction Lower urinary tract symptoms (LUTS) can be divided into storage, voiding, and postmicturition symptoms [1]. Depending on the severity threshold, the prevalence of male LUTS ranges from 10.3% to 25.1% [2–4]. It was estimated that in 2008, 917 million men worldwide were affected by benign prostatic hyperplasia (BPH)/LUTS [5]. There is a clear increase of LUTS prevalence with age [6]. The incidence of LUTS increases from 3 per 1000 per year among men aged 45–49 yr to 38 per 1000 per year among men aged 75–79 yr [2]. Traditionally, LUTS in adult men were attributed to benign prostatic enlargement, and terms such as prostatism or BPH were used synonymously. However, the bladder has also been recognized as a main contributor to male LUTS [7], and consequently, drugs targeting the bladder rather than the prostate could be added to the armamentarium of LUTS treatment. This philosophy was followed by most guidelines [8,9]. Several drugs for the treatment of male LUTS are available [8,9]: a1-adrenoceptor antagonists (a1-blockers), 5a-reductase inhibitors (5-ARIs), muscarinic receptor antagonists (antimuscarinics), and just recently approved in the United States and Europe, phosphodiesterase type 5 inhibitors (PDE5-Is). The use of different modes of action and targeting different symptom complexes by a drug combination seems appealing. In response to previous selective reviews on the topic, this systematic review summarizes, in a methodical, evidence-based medicine approach, the true evidence behind combination therapy for men with LUTS. 2. Evidence acquisition A systematic literature search in the PubMed and Cochrane databases was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis statement [10] to identify clinical trials, randomized controlled trials (RCTs), meta-analyses, and guidelines on male-LUTS combination therapy published from January 1988 to March 2012. In several search rounds, various algorithms including the following MeSH terms were used: lower urinary tract symptoms, prostatic hyperplasia, overactive urinary bladder, adrenergic alpha 1 receptor antagonists, 5 alpha reductase inhibitors, muscarinic antagonists, vasopressins, phosphodiesterase 5 inhibitors, adrenergic beta 3 receptor agonists, phytotherapy, botulinum toxin, and combination drug therapy. The limits used (ie, inclusion criteria) in all search rounds were clinical trial, meta-analysis, randomized controlled trial, guideline, male, humans, and English, French, German, or Italian. Exclusion criteria were the following: (1) articles reporting on neurogenic LUTS, (2) articles reporting on LUTS in women or children, (3) articles reporting on monotherapy and not on a combination of two drugs (or, if the drug combination was not from two different pharmacologic compound, eg, a combination of two phytotherapeutics), (4) review articles, and (5) guidelines, which in their latest updated version were >3 yr old. Each identified article was analyzed, classified, and labeled 229 according to the recommendations of the Centre for Evidence Based Medicine [11]. Studies below the level of evidence 1b (RCTs) were excluded; the agreement on such exclusions was formulated via the Delphi approach [12]. 3. Evidence synthesis A total of 49 papers published between January 1988 and March 2012 were identified (Fig. 1). 3.1. Combination of a1-blocker with 5a-reductase inhibitor The first clinical reports to combine the pharmacologic principles of a-adrenergic blockade with androgen antagonism to treat male LUTS were published at the end of the last century in Japan. At the time, the authors used compounds that no longer have any clinical relevance due to their lack of specificity and to their side effects [13,14]. Today, countless review articles and guidelines suggest that the combination of a1-blockers with 5-ARI is well established. Six RCTs have been published on a1-blocker/5-ARI combination therapy, five of which directly assessed the impact of medication on LUTS: the Veterans Affairs Cooperative Study (VA-COOP); the Alfuzosin, Finasteride, and Combination in the Treatment of BPH study (ALFIN); the Medical Therapy of Prostatic Symptoms study (MTOPS); the Prospective European Doxazosin and Combination Therapy study (PREDICT); and the Combination of Avodart and Tamsulosin study (CombAT) [15–31] (Table 1). The remaining study assessed whether the a1-blocker can be omitted after initial successful combination therapy [32]. Only the MTOPS and the CombAT trials had study durations >1 yr, a point that is important to remember given the longterm impact offered by the 5-ARI component of this combination therapy. 3.1.1. Subjective outcomes of a1-blocker/5a-reductase inhibitor combination therapy In the VA-COOP study, 1229 patients with LUTS were treated with terazosin, finasteride, or placebo for 1 yr. Patients receiving the combination treatment showed a significant reduction from the baseline American Urological Association symptom score (AUA-SS) of 6.2, which was significantly higher than the reduction by the 5-ARI (AUASS: 3.2) or placebo (AUA-SS: 2.6) alone but not significantly different from the a1-blocker alone (AUA-SS 6.1) [15] (Table 1). The reduction of symptom scores was reached after 13 wk of treatment and did not change within the 39 wk thereafter [15]. As such, the VA-COOP study does not report a subjective advantage of combination therapy compared to a1-blockers alone. In the ALFIN trial, 1051 patients with LUTS received either alfuzosin or finasteride or a combination of both over 6 mo. Starting at 1 mo after treatment, patients receiving the combination had a significant reduction from baseline International Prostate Symptoms Score (IPSS) of 6.1, which was significantly higher than the reduction with finasteride alone (IPSS: 5.2) but not different from alfuzosin alone (IPSS: 6.3) [17]. Similar to the VA-COOP study, the ALFIN 230 EUROPEAN UROLOGY 64 (2013) 228–243 [(Fig._1)TD$IG] Initial search (n = 1097) After exclusion of duplicates (n = 462) After exclusion of reviews, and of reports on monotherapies, neurogenic LUTS, women and children, and studies with level of evidence <1b (n = 48) Continuous consultations among the coauthors (Delphi approach) to obtain greatest agreement upon exclusion of papers Inclusion of one paper via manual search *1 n = 49 papers α1-Blocker + 5-ARI n = 29 papers α1-Blocker + antimuscar inic 18 papers reporting on 6 studies 13 papers reporting on 8 studies 6 studies, of which 1 assessed aspects other than direct clinical outcomes n=6 add-on studies and n=2 studies α1-Blocker + PDE5I n = 1 (meta analysis) α1-Blocker + phytotherap eutic Guidelines n=5 n = 1 paper n=5 studies Fig. 1 – Flow chart of study selection for inclusion in this review. *1 Five papers were included via manual search. Three of those do not report on combination therapy, but were considered relevant by the authors (Andriole et al., Marberger et al., Bent et al.). One was published in Japanese, and only available as a translated reprint (Saito et al.). And one was published in a journal (LUTS) that is not listed in PubMed yet (Nishizawa et al.). Table 1 – a1-Adrenoceptor antagonists and 5a-reductase inhibitor combination trial characteristics and subjective outcome measures Trial Years trial was performed Patients, no. Drug (dose) Trial duration, mo Primary end point Age of patients and size of prostate at baseline, mean SD 1992–1995 1229 Terazosin (10 mg) finasteride (5 mg) 12 AUA-SS and Qmax 65 7 yr and 37 1 ml ALFIN [17] 1994–1996 1051 Alfuzosin (2 x 5 mg) finasteride (5 mg) 6 IPSS and Qmax 63 6 yr and 41 24 ml PREDICT [22] 2001–2007 1095 Doxazosin (4–8 mg) finasteride (5 mg) 12 IPSS and Qmax 63 7 yr and 36 14 ml (assessed by DRE) MTOPS [19] 1995–2001 3047 Doxazosin (4–8 mg) finasteride (5 mg) 54–72 62 7 yr and 36 20 ml CombAT [28] 2003–2009 3195–3822 Tamsulosin (0.4 mg) dutasteride (0.5 mg) 24–48 Clinical progression (as defined by, eg, an AUA score increase of 4 points) Time to first AUR or BPHrelated surgery 66 7 yr and 55 23 ml Change of symptom score from baseline (IPSS or AUA-SS) a1-Blocker Age 45–80 yr AUA-SS >8 PSA 10 ng/ml Qmax 4–15 ml/s No limits on prostate size Age 50–75 yr IPSS >7 PSA 10 ng/ml Qmax 5–15 ml/s No limits on prostate size Age 50–80 yr IPSS >12 PSA 10 ng/ml Qmax 5–15 ml/s Prostatic enlargement assessed by DRE Age >50 yr AUA-SS 8–30 PSA 10 ng/ml Qmax 4–14 ml/s No limits on prostate size Age >50 yr IPSS >12 PSA 1.5–10 ng/ml Qmax 5–15 ml/s Prostate size >30 ml 5-ARI Placebo Combination S6.1 Significant vs baseline vs 5-ARI vs placebo S3.2 Significant vs baseline S2.6 Significant vs baseline S6.2 Significant vs baseline vs 5-ARI vs placebo S6.3 Significant vs baseline vs 5-ARI S5.2 Significant vs baseline n.a. n.a. S6.1 Significant vs baseline vs 5-ARI S8.3 Significant vs baseline vs 5-ARI vs placebo S6.6 Significant vs baseline S5.7 Significant vs baseline S8.5 Significant vs baseline vs 5-ARI vs placebo S6.6 Significant vs baseline vs placebo vs 5-ARI S5.6 Significant vs baseline vs placebo S4.9 Significant vs baseline S7.4 Significant vs baseline vs placebo vs 5-ARI vs a1-blocker S3.8 Significant vs baseline S5.3 Significant vs baseline vs a1-blocker n.a. n.a. S6.3 Significant vs baseline vs 5-ARI vs a1-blocker EUROPEAN UROLOGY 64 (2013) 228–243 VA-COOP [15] Inclusion criteria a1-blocker = a1-adrenoceptor antagonist; 5-ARI = 5a-reductase inhibitor; ALFIN = Alfuzosin, Finasteride, and Combination in the Treatment of Benign Prostatic Hyperplasia; AUA-SS = American Urological Association symptom score; AUR = acute urinary retention; BPH = benign prostatic hyperplasia; CombAT = Combination of Avodart and Tamsulosin; DRE = digital rectal examination; IPSS = International Prostate Symptom Score; MTOPS = Medical Therapy of Prostatic Symptoms; Qmax = maximum flow rate of urine; PSA = prostate-specific antigen; n.a. = not assessed; PREDICT = Prospective European Doxazosin and Combination Therapy; SD = standard deviation; VA-COOP = Veteran Affairs Cooperative Study. 231 232 EUROPEAN UROLOGY 64 (2013) 228–243 trial did not support combination therapy over a1-blocker monotherapy with regard to subjective outcome measures. In the PREDICT trial, 1095 patients received either doxazosin, finasteride, or a combination of both over 1 yr. Patients receiving combination therapy or doxazosin alone had a significantly higher IPSS reduction (IPSS: 8.5 and 8.3, respectively) than patients receiving either finasteride (IPSS: 6.6) or placebo (IPSS: 5.7) alone [22]. The VA-COOP, ALFIN, and PREDICT studies all failed to show a subjective advantage of a1-blocker/5-ARI combination over a1-blocker monotherapy. However, none of the three studies accounted for effects that might have occurred after receiving therapy for >1 yr. The MTOPS trial tested either doxazosin or finasteride, alone or in combination, against placebo for 4–6 yr in 3047 symptomatic patients. Finasteride alone reduced the AUA-SS by 5.6 points, doxazosin alone by 6.6 points, and the combination by 7.4 points [19]. Thus, MTOPS was the first trial with a long-term follow-up (mean: 4.5 yr) in which an advantage of combination therapy over either monotherapy was demonstrated, especially in subjective outcome parameters. Similarly, the CombAT trial, another trial with a duration of 4 yr, reported after 4 yr of treatment a significantly larger IPSS reduction for combination therapy (IPSS: 6.3) than for either tamsulosin (IPSS: 3.8) or dutasteride (IPSS: 5.3) alone [28]. The different outcomes between the MTOPS and CombAT studies can be explained by different study populations. Whereas the MTOPS study recruited men suffering from LUTS without any limitation in prostate size, the CombAT study only included men with a prostate volume >30 ml. This means that the results of the CombAT study cannot be extrapolated to every man suffering from LUTS. At the CombAT interim analysis 2 yr after onset of treatment, IPSS values were reduced by 6.2 points in patients receiving combination therapy, by 4.3 points for those receiving tamsulosin, and by 4.9 points for dutasteride-alone group [23]. During the first 9–12 mo of treatment, tamsulosin alone also showed a larger IPSS reduction than dutasteride alone, but this significant difference vanished after 12 mo of treatment. After 18 mo of treatment, patients in the dutasteride group had a significantly higher reduction of voiding symptoms within the IPSS than patients in the tamsulosin group [27]. The significantly higher IPSS reduction achieved with combination therapy was apparent after 3 mo versus dutasteride and 9 mo versus tamsulosin [23,30]. The apparent superiority of the 5-ARI arm over the a1-blocker arm after the 18-mo period in the CombAT study was likely related to the effect of patient enrolment: Patients were selected for larger prostate volumes not previously tested in any combination trial. In addition to the longer treatment periods of the MTOPS and CombAT studies, their informative value is more sensitive because they used statistically better-defined, primary, study end points than the VA-COOP, ALFIN, or PREDICT studies (Table 1). Whereas the latter three used IPSS and maximum flow rate of urine (Qmax) as primary end points, the MTOPS study used a composite end point for BPH progression, including as primary end points a somewhat arbitrary 4-point IPSS worsening (confirmed at 2 wk), acute urinary retention (AUR), urinary tract infection (UTI), worsening of renal function attributed to obstruction, and urinary incontinence that was socially unacceptable. The MTOPS study was also unique in defining this composite BPH progression as the end point rather than the classic degree of symptom improvement used in all studies previously. This slight variation in treatment perspective transforms LUTS treatment from a process of symptom treatment to one of disease management. Having had or not having had BPH-related surgery was a secondary end point. Similarly, the CombAT study used a well-defined scenario of clinical progression as the primary end point after 4 yr. Assessing quality of life (QoL) (eg, IPSS question 8, BPH Impact Index, or the Patient Perception of Study Medication questionnaire) in the combination arm of the CombAT trial showed a higher satisfaction rate than tamsulosin alone starting from month 15 and dutasteride alone starting at 3 mo [25]. Improved QoL with combination therapy compared to each monotherapy was maintained throughout the 4 yr of treatment [29]. After finishing the trial, 64% of patients receiving combination therapy, 58% of the dutasteride-only group, and 55% of the tamsulosin-only group wished to continue the study medication [29]. However, these numbers also indicate that 36–45% of patients were not satisfied with their medical treatment. In summary, the results favor combination therapy when subjective outcome measures (AUA-SS, IPSS) were assessed, treatment lasted >1 yr (Table 1), and the patient selected for treatment had some critical level of prostate enlargement. When combination treatment was used for <1 yr or for LUTS regardless of prostate volume, there were no significant differences compared to a1-blocker monotherapy. Whether the combination therapy is still more efficacious than 5-ARI monotherapy after >6 yr or if the difference disappears between the drug combination and 5-ARI has not yet been thoroughly assessed and remains to be elucidated. 3.1.2. Objective outcomes of a1-blocker and 5a-reductase inhibitor combination therapy Trials with a duration of <1 yr (ie, the VA-COOP, ALFIN, and PREDICT studies) reported a Qmax increase of 2.3–3.8 ml/s for combination therapy, 1.4 ml/s for placebo, 1.6–1.8 ml/s for 5-ARI alone, and 1.8–3.6 ml/s for a1-blocker alone [15,17,22]. The differences were significantly different between combination and 5-ARI or placebo alone, but not from a1-blocker alone [15,22]. However, long-term trials (ie, MTOPS and CombAT) showed a significant Qmax increase of 2.4–3.7 ml/s for combination therapy, 2.0–2.2 ml/s for 5-ARI alone, 0.7–2.5 ml/s for a1-blocker alone, and 1.4 ml/s for placebo [19,28]; however, the different prostate sizes in the trials have to be considered (Table 1). Prostate size was reduced by 7 ml with combination therapy and by 6.1 ml with finasteride but increased by 0.5 ml with terazosin or placebo in the VA-COOP study [15]; in the ALFIN study, prostate size decreased by 4.3 ml with combination therapy, by 4.9 ml with finasteride, and by 0.2 ml with alfuzosin [17]. It should be kept in mind that the effect on prostate size in the VA-COOP, ALFIN, and PREDICT EUROPEAN UROLOGY 64 (2013) 228–243 233 studies is limited by their short study periods and the methods used to measure volume, which vary greatly. Over 4 yr with combination therapy and 5-ARI monotherapy, prostate sizes were equally reduced by 19–28%, whereas prostate size increased by 4.6–24% with a1-blockers alone. The increase in prostate size with a1-blocker therapy represents the natural growth of the prostate as shown by the same size increase in placebo groups [19,28] (Table 2). During the PREDICT study, AUR and need for surgery occurred within 1 yr of treatment in 2.6% of patients treated with placebo, in 1.9% of those treated with finasteride, and in 0.4% of those receiving doxazosin, but in no patient receiving combination therapy [22]. Clinical progression, as defined by an increase in 4 AUA-SS points, AUR, renal insufficiency, recurrent UTIs, or self-reported, unacceptable incontinence occurred in 4.5% of patients per year in placebo-treated patients of the MTOPS study. Of all progression parameters, symptom deterioration occurred most frequently (78%). The number needed to treat (NNT) to prevent one instance of overall clinical progression was 13.7 for doxazosin, 15.0 for finasteride, and 8.4 for combination therapy (relative risk [RR] reduction for disease progression was 39% for doxazosin, 34% for finasteride, and 66% for combination therapy). Within 4 yr, 17% of those treated with placebo, 10% with doxazosin, 10% with finasteride, and 5% with combination therapy experienced clinical disease progression [19]. However, the risk for AUR and/or invasive therapy was equally reduced by finasteride monotherapy and combination therapy, whereas doxazosin alone did not significantly affect AUR or the need for invasive therapy [19]. As such, 5-ARIs reduce disease progression (ie, prevent AUR or surgery), whereas a1-blockers only delay but do not prevent BPH progression. Similarly, the CombAT study showed a RR reduction for AUR or surgery of 65.8% for combination therapy compared to tamsulosin alone but was not significantly different from dutasteride alone. The benefit of the prevention of AUR or surgery in those receiving combination or dutasteride became apparent at month 8 [28]. In analogy to subjective outcome parameters, a1blocker/5-ARI combination therapy is superior in increasing Qmax and delaying disease progression to either monotherapy when given for >8 mo. Whether the combination therapy is more efficacious than 5-ARI alone in the long term (>6 yr) is not yet clear. (>40 ml) have a higher risk of having invasive therapy later. In the MTOPS study, the overall NNT to prevent one patient from invasive therapy was 25.9 for combination therapy. In patients with an initial PSA level >4 ng/ml or prostate size >40 ml, the NNT was 23.1 and 15.9, respectively [19]. In the CombAT study, the RR reduction of AUR or of BPH-related surgery with combination therapy was only significant (compared to tamsulosin alone) when prostate volume at baseline was >42 ml [31]. RR reduction with combination therapy (compared to tamsulosin) was 69.3% for patients with an initial prostate size of 42.0–57.8 ml and 72.6% for patients with initial prostate size >57.8 ml [31]. Combination therapy in the CombAT study was more efficacious than any monotherapy with respect to IPSS reduction. However, the onset at which these differences became apparent was dependent on prostate size at baseline. In patients whose prostate volume was <42 ml, combination therapy compared to tamsulosin was more efficacious in IPSS reduction starting at month 21. However, in patients with prostate volume of 42–58 ml at baseline, the differences occurred after only 6 mo, and after 3 mo in patients with prostate volume >58 ml [24]. Dutasteride alone was only significantly efficacious in reducing IPSS compared to tamsulosin alone in patients with an initial prostate size >49 ml [24]. Different degrees of outcomes in the MTOPS and CombAT trials are most likely attributable to different prostate sizes, PSA values, and age at baseline (Table 1). The MTOPS study, which included patients with an average prostate size of 36 20 ml, reported only a moderate advantage of combination therapy compared to monotherapies. In contrast, the CombAT study, which only included patients with a minimum prostate size of 30 ml and had an average prostate size of 55 23 ml at baseline, reported a more pronounced advantage of combination therapy over monotherapies, indicating that patients with enlarged prostates (>40 ml) especially benefit from a1-blocker/5-ARI combination therapy. In summary, the subgroup analyses revealed that, in particular, patients with enlarged prostates (>30–40 ml, or a PSA value >4 ng/ml as proxy parameter for an enlarged prostrate) benefit from a1-blocker/5-ARI combination when treatment is given for a prolonged period. The impact of combination treatment is linearly related to prostate volume. 3.1.3. 3.1.4. Subgroup analyses of a1-blocker and 5a-reductase inhibitor Adverse events of a1-blocker and 5a-reductase inhibitor combination therapy combination therapy In the VA-COOP study, no significant change in Qmax was shown for 5-ARI monotherapy. However, when patients with a baseline prostate volume >50 ml were separately analyzed, Qmax increase (2.7 ml/s) was significant and not different from combination therapy or terazosin alone [16]. Similarly, in the ALFIN trial, Qmax increase in alfuzosin or combination therapies became more pronounced when patients with an initial Qmax <10 ml/s were analyzed [17]. It should be kept in mind that these subgroup findings were post hoc analyses, limiting their scientific validity. Patients with elevated, baseline, serum prostate-specific antigen (PSA) concentrations (>4 ng/ml) and/or prostate volumes A1-adrenoceptor-specific adverse events (AEs), such as dizziness, hypotension, or rhinitis occurred significantly more frequently in a1-blocker and combination therapy than in 5-ARI therapy (Table 3). Antiandrogenic AEs, such as erectile dysfunction (ED), decreased libido, or reduction of semen volume, occurred significantly more often in 5-ARI and combination treatments than in a1-blocker therapy groups [15,19,22] (Table 3). Consequently, AEs were more prevalent in patients with combination therapy than in any monotherapy group. AEs seem to be additive and not synergistic. Severe AEs were not observed in either treatment group [15,19,22] and discontinuation rates were 234 Table 2 – a1-Adrenoceptor antagonists and 5a-reductase inhibitor combination objective outcome measures* Change in Qmax from baseline (ml/s) a1-Blocker +2.7 ALFIN [17] (alfuzosin/finasteride) +1.8 PREDICT [22] (doxazosin/finasteride) +3.6 MTOPS [19] (doxazosin/finasteride) +2.5 CombAT [28] (tamsulosin/dutasteride) +0.7 Placebo Combination Significant vs baseline vs 5-ARI vs placebo Significant vs baseline +1.6 Significant vs baseline +1.4 Significant vs baseline +3.2 +1.8 Significant vs baseline n.a. n.a. +2.3 Significant vs baseline vs 5-ARI vs placebo Significant vs baseline vs placebo +1.8 Significant vs baseline +1.4 Significant vs baseline +3.8 +2.2 Significant vs baseline vs placebo +1.4 Significant vs baseline +3.7 +2.0 Significant vs baseline vs a1-blocker n.a. n.a. +2.4 Significant vs baseline a1-Blocker Significant vs baseline vs 5-ARI vs placebo Significant vs baseline +0.5 ml Significant vs baseline vs 5-ARI vs placebo Significant vs baseline vs placebo vs 5-ARI vs a1-blocker Significant vs baseline vs 5-ARI vs a1-blocker n.a. n.a. +24% n.r. +4.6% Significant vs baseline 0.2 ml 5-ARI Significant vs baseline 6.1 ml n.s. 4.3 ml Combination +0.5 ml Significant vs baseline 7 ml n.a. n.a. 4.9 ml n.a. n.a. n.r. +24% n.r. 19% n.r. Significant vs baseline vs a1-blocker n.a. n.a. 27.3% Significant vs baseline vs 5-ARI vs a1-blocker Significant vs baseline vs 5-ARI vs placebo Significant vs baseline vs a1-blocker n.a. 19% 28% n.a. Placebo n.a. Significant vs baseline vs 5-ARI vs placebo Significant vs baseline vs a1-blocker n.a. Qmax = maximum flow rate of urine; 5-ARI = 5a-reductase inhibitor; a1-blocker = a1-adrenoceptor antagonist; ALFIN = Alfuzosin, Finasteride, and Combination in the Treatment of Benign Prostatic Hyperplasia; AUR = acute urinary retention; CombAT = Combination of Avodart and Tamsulosin; MTOPS = Medical Therapy of Prostatic Symptoms; n.a. = not assessed; n.r. = not reported; PREDICT = Prospective European Doxazosin and Combination Therapy; VA-COOP = Veteran Affairs Cooperative Study. * Prostate size was given only as percentage value in some trials. EUROPEAN UROLOGY 64 (2013) 228–243 VA-COOP [15] (terazosin/finasteride) 5-ARI Change in prostate size from baseline Table 3 – a1-Adrenoceptor antagonists and 5a-reductase inhibitor combination selected side effects 3 7 1 5 n.r. n.r. 1.9 n.r. 5 1.7 0.6 2.2 27 1.7 7.8 0.6 1.2 1.2 1.7 6.7 26 2.9 5.9 0.3 n.a. n.a. n.a. n.a. n.a. n.a. n.a. n.a. 1.4 2.3 15.6 3.6 5.8 n.r. n.r. 11.6 0.4 n.r. 8 3.4 4.9 n.r. n.r. 13.6 1.9 n.r. 7.4 1.9 10.5 n.r. n.r. 11.9 2.6 n.r. 13.6 2.3* 2.3* 4.5* 24 n.r. n.r. <1 n.r. 2.2* 1.4* 3.3* n.r. n.r. n.r. 2 n.r. 3 7 21 <1 4 2.7 n.a. n.a. n.a. n.a. n.a. n.a. n.a. n.a. n.r. n.r. 4.4* 1.5* 3.5* 27 n.r. n.r. 1 n.r. n.r. 2 2 5 19 <1 4 6.8 n.r. <1 n.r. n.r. 9.4 n.r. 2 7.4 26 2.3 8.1 0.3 2.1 3.3 n.r. n.r. 12.6 0 5.3* 2.5* 5.1* 18 n.r. n.r. <1 2 4 9 28 <1 6 2.2 Impotence 9 21 Loss of libido 5 Dizziness and hypotension AUR n.r. Discontinuation rate due to side effects AUR 6.1 Severe side effects Discontinuation rate due to side effects n.r. Side effects total Severe side effects n.r. Headache Side effects, total 9 Impotence AUR 5 Loss of libido Discontinuation rate due to side effects 8 Dizziness and hypotension Severe side effects 6 Headache Side effects, total n.r. Impotence 7.0 Loss of libido n.r. Dizziness and hypotension n.r. Headache AUR 6 Impotence 3 26 Loss of libido Discontinuation rate due to side effects n.r. Combination, % Severe side effects 2 Placebo, % Side effects, total 6 5ARI, % EUROPEAN UROLOGY 64 (2013) 228–243 VA-COOP [15] (terazosin/finasteride) ALFIN [17] (alfuzosin/finasteride) PREDICT [22] (doxazosin/finasteride) MTOPS [19] (doxazosin/finasteride) CombAT [28] (tamsulosin/dutasteride) Dizziness and hypotension Headache a1-Blocker, % a1-Blocker = a1-adrenoceptor antagonist; 5-ARI = 5a-reductase inhibitor; ALFIN = Alfuzosin, Finasteride, and Combination in the Treatment of Benign Prostatic Hyperplasia; AUR = acute urinary retention; CombAT = Combination of Avodart and Tamsulosin; MTOPS = Medical Therapy of Prostatic Symptoms; n.a. = not assessed; n.r. = not reported; PREDICT = Prospective European Doxazosin and Combination Therapy; VA-COOP = Veteran Affairs Cooperative Study. * Rate per 100 person-years of follow-up. 235 236 EUROPEAN UROLOGY 64 (2013) 228–243 similar between treatment groups (6–12.6%), depending on study duration [22]. Within 2 yr of treatment, drug-related AEs occurred more often in the combination therapy group (24%) than in the tamsulosin (16%) or dutasteride (18%) groups. However, the occurrence of a serious drug-related AE (<1% in each treatment arm) or withdrawal rates from the CombAT trial (<5% in each treatment arm) were similar among the groups [23]. After 4 yr of treatment, 6% of patients receiving combination therapy, 4% receiving tamsulosin, and 4% receiving dutasteride discontinued the study due to drugrelated AEs [28]. In summary, AEs do not seem to be the key criterion for or against combination therapy (Table 3). It should also be mentioned that 60–80% of LUTS/BPH patients are sexually active [33]. Both 5-ARI and a1-blockers might cause sexually related side effects (eg, loss of libido with 5-ARI therapy or ejaculation dysfunction [EjD] with a1-blockers). When a1-blockers and 5-ARI are combined, these potential side effects might be additive and affect patients’ sexual life. The effect of a1-blockers on sexual function in men with LUTS is variable during a short period, with men reporting either no change or a modest improvement of unknown significance. However, the effect of a1-blocker on EjD in men with LUTS is significantly affected by tamsulosin and silodosin, whereas the other commonly used a1-blockers have little or no impact on EjD. The effect of 5-ARI on sexual function in men with LUTS is modest but global, with effects on penile erection, ejaculation, and sexual desire. There seems to be no significant difference between the two agents that are currently available. The veracity of reports on persistence of the sexual side effects following cessation of 5-ARIs when these drugs have been used to treat male pattern baldness is unclear. The impact of drug therapies for LUTS on sexual function should not be overlooked in discussing potential side effects with individual patients. 3.1.5. Additional aspects of a1-blocker and 5a-reductase inhibitor combination therapy Although they are outside of the scope of this review, the authors would like to mention two additional aspects of a1-blocker/5-ARI combination therapy that are still controversially debated. It should be noted that both of these aspects are just mentioned here to raise awareness; they are not discussed in detail. For further details please refer to the cited studies. The first concept is that of a1-blocker withdrawal after initial successful combination therapy. The Symptom Management After Reducing Therapy (SMART) trial suggests that after 6 mo the a1-blocker might be omitted without symptom deterioration [32]. Similar results were reported from a Canadian study in which the a1-blocker was omitted after 9 mo [34]. However, current scientific data on this topic are insufficient. The second aspect is the possible effects of the a1-blocker/ 5-ARI combination on prostate cancer (PCa) diagnosis and PSA serum levels. It seems important to mention that the Reduction by Dutasteride of Prostate Cancer Events (REDUCE) trial, performed subsequently to CombAT, suggests that dutasteride over a 4-yr period might reduce the risk of PCa [35]. Similarly, the Prostate Cancer Prevention Trial (PCPT) reported that finasteride prevents or delays the appearance of PCa [36]. However, it should also be noted that although 5-ARI might reduce the likelihood of total PCa diagnosis, it seems to concurrently increase the likelihood of a high-grade PCa diagnosis. As a consequence, the US Food and Drug Administration issued a warning in September 2011 and obliged pharmaceutical companies to change their warning and precaution labels for 5-ARIs accordingly [37]. In addition, the physician prescribing a 5-ARI should be aware that these compounds affect PSA serum levels and, consequently, PCa screening. Several articles provide insight into the interpretation and use of PSA serum levels under 5-ARI therapy [38,39]. 3.2. Combination of a1-blockers and muscarinic receptor antagonists The first clinical study on combination therapy with a1blockers and muscarinic receptor antagonists (antimuscarinics) was published by Saito and coworkers in 1999 [40]. They administered tamsulosin and propiverine to patients with enlarged prostates and increased frequency of any cause (including neurogenic bladder). Following this study, clinical studies with more homogeneous study populations were performed on a1-blocker/antimuscarinic combinations [41–53] (Table 4). The majority are add-on studies, in which antimuscarinics have been added to baseline a1-blocker therapy. Only one trial prospectively compared the antimuscarinic with placebo, a1-blocker, and a1-blocker/ antimuscarinic combination (the Tolterodine and Tamsulosin in Men With LUTS Including OAB: Evaluation of Efficacy and Safety [TIMES] study) [42]. All studies defined an upper limit of postvoid residual (PVR) and a lower limit of Qmax at initiation; therefore, conclusions concerning efficacy and safety are only valid for patients with PVR <200 ml and Qmax >5 ml/s. All studies on a1-blocker/antimuscarinic combination therapy have only a short follow-up (usually 12 wk), and no study assessed the outcomes of this combination for >4 mo. Therefore, it is currently unknown if long-term a1-blocker/ antimuscarinic combination is useful, safe, and/or effective. 3.2.1. Subjective outcomes of a1-blocker/antimuscarinic combination therapy Add-on studies reported significant IPSS reductions when patients were treated with a1-blocker/antimuscarinic combination instead of an a1-blocker only, especially reductions of the IPSS storage subscore (questions 2, 4, and 7) [49,50,53]. A reduction in IPSS of 3 points was observed in 74.4% of patients when oxybutinin was given as an add-on but only in 65% of patients receiving placebo add-ons [45]. Reports on antimuscarinics as add-on therapy regarding the patients’ QoL are controversial, but most studies concluded that addon therapy does not significantly improve QoL compared to placebo [49,50,53]. However, different inclusion criteria in the studies and different time periods regarding duration of previous a1-blocker use make outcome parameters difficult to compare (Table 4). Another flaw of several studies Table 4 – a1-Adrenoceptor antagonist and antimuscarinic combination: International Prostate Symptom Score outcome and trial characteristics Trial Level of Patients, evidence no. Drug (dose) Duration, mo Inclusion criteria Time during which an a1-blocker was given prior to add-on antimuscarinic, wk Total IPSS reduction from baseline (IPSS storage symptom reduction, where assessed separately) a1-Blocker 7.8 (3.4) Significant vs baseline vs placebo Placebo 6.8 (3.4) Significant vs baseline 6.2 (2.8) Significant vs baseline 7.4 (3.8) Significant vs baseline 7.3 (2.9) Significant vs baseline 4 6.9 (3.7) Significant vs baseline vs placebo 5.2 (2.4) Significant vs baseline 4 5.4 (2.8) Significant vs baseline 4.9 (2.3) Significant vs baseline 4 4.8 (2.7) Significant vs baseline vs placebo 4.3 (2.2) Significant vs baseline 6 3.5 (2.4) Significant vs baseline vs placebo 3.1 (1.8) Significant vs baseline 8 (2.2) Significant vs baseline (1.1) Significant vs baseline Significant vs baseline Significant vs baseline 4.6 Significant vs baseline Significant vs baselin Unknown 15 ml/s 5.1 Unknown <15 ml/s 5.3 3.7 Combination 8.0 (4.2) Significant vs baseline vs placebo 237 a1-Blocker = a1-adrenoceptor antagonist; ADAM = Add-on study of Detrol LA to Alpha-blockers in men; ASSIST = Add-on therapy of Solifenacin Succinate in men for BPH with OAB symptoms treated by Tamsulosin; BPH = benign prostatic hyperplasia; IPSS = International Prostate Symptom Score; LUTS = lower urinary tract symptoms; OAB = overactive bladder; PVR = postvoid residual; PSA = prostate-specific antigen; Qmax = maximum flow rate of urine; TAABO = Trial of combination treatment of an Alpha-blocker plus an Anticholinergic for BPH with OAB; TIMES = Tolterodine and Tamsulosin in men with LUTS; VICTOR = Vesicare in combination with Tamsulosin in OAB residual symptoms. EUROPEAN UROLOGY 64 (2013) 228–243 Studies in which a1-blocker, antimuscarinic, or a combination of both was tested from the start TIMES [42] 1b 879 Tamsulosin 3 Age >40 yr (0.4 mg) Qmax >5 ml/s tolterodine PVR <200 ml (4 mg) IPSS >12 >8 voids/24 h PSA 10 ng/ml Studies in which a1-blocker/antimuscarinic or a1-blocker/placebo was tested from the start Lee et al. [41] 1b 228 Doxazosin 2 Age 50–80 yr (4 mg) propiverine >8 voids/24 h (20 mg) urodynamically obstructed (Abrams-Griffith >20) PVR <30% bladder capacity Studies in which antimuscarinic or placebo was tested as add-on to an a1-blocker MacDiarmid 1b 409 Tamsulosin 3 Age >45 yr et al. [45] (0.4 mg) Qmax >8 ml/s oxybutinin PVR <150 ml (10 mg) IPSS >13 IPSS storage subset >8 PSA 4 ng/ml VICTOR [48] 1b 397 Tamsulosin 4 Age >45 yr (0.4 mg) Qmax >5 ml/s solifenacin (5 mg) PVR <100 ml IPSS >13 >8 voids/24 h PSA 10 ng/ml ADAM [49] 1b 652 Any a1-blocker 3 Age >45 yr tolterodine (4 mg) no limit on Qmax PVR <200 ml >8 voids/24 h >1 urgency episode/24 h PSA 10 ng/ml 3 Age >50 yr ASSIST [50] 1b 638 Tamsulosin Qmax >5 ml/s (0.2 mg) solifenacin PVR <50 ml (2.5–5 mg) >8 voids/24 h >2 urgency episodes/24 h 3 Age >50 yr TAABO [53] 1b 214 Tamsulosin Qmax 5–15 ml/s (0.2 mg) propiverine PVR <100 ml (10–20 mg) IPSS >8 >8 voids/24 h >1 urgency episodes/24 h 3 Age >40 yr Oelke et al. [52] 1b 1849 Propiverine Qmax >10 ml/s (30 mg) with or without a1-blocker PVR <100 ml (any) IPSS <20 >8 voids/24 h prostate size<40 ml Antimuscarinic 238 EUROPEAN UROLOGY 64 (2013) 228–243 assessing a1-blocker/antimuscarinic combinations by using IPSS questionnaires only is that antimuscarinics target mainly those OAB symptoms that are not adequately assessed by the IPSS questionnaires. Regardless of initial PSA values, the effects of add-on tolterodine were dependant on prostate size [51]. Another study reported that IPSS reduction with propiverine was more pronounced in patients with Qmax <15 ml/s at baseline [52]. However, data on specific patient groups that might profit from add-on treatment are scarce. Particularly, low case numbers and high patient heterogeneity in existing trials make it difficult to determine which LUTS patient benefits most from an add-on antimuscarinic therapy. The TIMES study was the only one that included an antimuscarinic alone and showed that patients treated with combination therapy, but not with tamsulosin, tolterodine, or placebo alone, had a significant treatment benefit as defined by the patient perception questionnaire (80% vs 71%, 65%, and 62%, respectively) [42]. Similarly, following the 12 wk of treatment, only combination therapy significantly improved total IPSS and QoL; tolterodine alone did not differ from the placebo. Interestingly, after the same treatment period, tamsulosin alone did improve total IPSS but without significant effects on the IPSS QoL item [42]. Furthermore, the IPSS storage subscore was only significantly reduced in the combination group [46]. However, in men with a PSA value <1.3 ng/ml or prostate size <29 ml, tolterodine alone was also able to significantly reduce storage symptoms [44,47]. As such, the TIMES study indicated that in the short term, especially men with enlarged prostates benefit from a1-blocker/antimuscarinic combination therapy. In men with small prostates, antimuscarinics alone appear to be just as efficacious [37]. 3.2.2. Objective outcomes of a1-blocker/antimuscarinic combination therapy Studies in which antimuscarinics were assessed as add-ons to a1-blockers showed no significant differences in Qmax between treatment groups [41,49,53]. Add-on combination therapy, when compared to a1-blockers alone, showed a significantly higher reduction in 24-h voiding frequency [41,49,50,52,53] (eg, 23.5% vs 14.3% [41]) and urgency episodes per day [48–50,52] (eg, 2.9 vs 1.8 [49]). The TIMES study reported that in patients with prostate size >29 ml, only combination therapy significantly reduced 24-h voiding frequency (2.8 vs 1.7 with tamsulosin alone, 1.4 with tolterodine alone, or 1.6 with placebo). In patients with prostate size <29 ml, tolterodine alone also reduced 24-h voiding frequency (tamsulosin/tolterodine combination: 2.2 voids, tolterodine: 1.9, placebo: 1.1, and tamsulosin: 1.6) [47]. The significant frequency reduction began 1 wk after the start of treatment [42]. The a1-blocker/antimuscarinic combination does not seem to influence Qmax but improves other objective outcome parameters such as 24-h frequency and urgency episodes. Similar to other subjective outcome parameters, combination therapy appears to be as efficacious as antimuscarinics alone in men with small prostate volume (<30 ml). 3.2.3. Adverse events of a1-blocker/antimuscarinic combination therapy Although some studies found a statistically significant increase in PVR with antimuscarinics (alone or in combination), most studies did not find a significant increase in AUR with antimuscarinics [41,42,45,49,52,53] (Table 3). For example, when oxybutinin was given to patients who had already received tamsulosin, mean PVR increased by 18.2 ml, whereas placebo increased PVR by 7.8 ml. No AUR occurred either in the oxybutinin/tamsulosin or in the placebo/ tamsulosin group [45]. Only a few studies reported a higher frequency of AUR in patients treated with antimuscarinic add-on compared to placebo add-on, ranging from 1.9% to 3% versus 0% after a treatment period of 3 mo [48,50]. Nevertheless, other studies including placebo groups reported an AUR incidence of approximately 1.8% (Table 5). When considering the natural incidence of AUR in untreated LUTS patients, the AUR rate with antimuscarinics appears to be similar or only slightly increased. However, it should be kept in mind that a selected group of patients was investigated who had an upper PVR limit of 200 ml and Qmax >5 ml/s at the time of inclusion and men with increased risk for AUR were excluded from the trials (a man with a PVR >200 ml is already at considerable risk for developing AUR) (Table 5). Results from these trials and subsequent recommendations can only be applied to patients with a similar risk profile. In general, caution (ie, regular evaluation of PVR) is recommended when prescribing antimuscarinics to patients with increased risk of developing AUR [8,9]. Interestingly, prostate size and serum PSA concentration at study initiation had no influence on AUR development during antimuscarinic treatment [47,51]. Study discontinuation occurred more frequently in patients with add-on combination therapy than in patients with placebo add-on (4.7–7% and 1.5–4%, respectively [41,48,50]). Other studies found no difference in discontinuation rates due to drug-related AEs [42,45] (Table 5). Antimuscarinic AEs, such as dry mouth or constipation, occurred in the combination therapy group more often than in patients receiving a1-blocker monotherapy [41,42,48–50]. For example, dry mouth occurred in 15.3% of patients taking oxybutinin or combination but in only 4.8% of patients taking tamsulosin or placebo [45]. In most studies, side effects were mild and disappeared upon drug discontinuation [41,48]. Similar to a1-blocker/5-ARI combination therapy, AEs do not seem to be a decisive criterion, since the type of AEs are identical with either monotherapy and do not potentiate. 3.3. Combination of a1-blockers with phosphodiesterase type 5 inhibitors Only small, clinical, pilot studies were conducted to assess a1-blocker/PDE5-I for the treatment of LUTS/BPH. These data were pooled in a meta-analysis [54]. Preliminary clinical studies testing a1-blocker therapy with intermittent PDE5-I (as a treatment for ED) focused primarily on safety (particularly on hemodynamic side effects), but they did not report any urologic outcome with regard to LUTS [55–59]. In conclusion, the combination of Table 5 – a1-Adrenoceptor antagonist and antimuscarinic combination side effects, postvoid residual volume increase, and acute urinary retention Acute urinary retention Study discontinuation due to side effects Side effects (dry mouth) 2.3 16.8 (2.2) 0 ( 3.6) 1.8 3.1 47.1 (20.8) 42.7 (18.3) 42.6 (15.3) 0 (6.4) 1.4 (20.7) 2.9 (18) 0.8 0 0 8.8 4.9 10.3 18.9 (5.8) 42.6 (4.8) 0 (n.r.) 0.5 (7) 0 0 1.4 9.7 <200 ml and >5 ml/s <30% bladder capacity <150 ml and >8 ml/s 45 (7) 34.7 (9.7) 55.9 (11.3) 13.1 (3.2) n.r. ( 13.5) 0 (13.6) 6.1 (22.6) 2.4 (n.r.) 3 0.9 1.9 0.8 7 4 4.7 7.4 39 (3) 27.6 (5.6) 42.1 (2.8) 0 (0) n.r. (0) 0 (1) 0.9 (5.9) 0 (n.r.) 0 0.6 0 0 4 2.5 2.8 0 <100 ml and >5 ml/s <200 ml and no Qmax limit <50 ml and >5 ml/s <100 ml and 5–15 ml/s Side effects (dry mouth) Study discontinuation due to side effects ClinicalIy significant* increase in PVR (mean increase, ml) 1.8 Acute urinary retention Side effects (dry mouth) 0 (5.2) ClinicalIy significant* increase in PVR (mean increase, ml) Study discontinuation due to side effects 19.9 (7.4) PVR and Qmax limitations of study patients Study discontinuation due to side effects Acute urinary retention 3.2 a1-Blocker/placebo, % Acute urinary retention ClinicalIy significant* increase in PVR (mean increase, ml) 0 ClinicalIy significant* increase of PVR (mean increase, ml) Side effects (dry mouth) a1-Blocker/antimuscarinic, % Acute urinary retention 0 (0.1) Placebo alone, % Study discontinuation due to side effects Clinically significant* increase in PVR (mean increase, ml) 27.9 (6.9) Antimuscarinic alone, % EUROPEAN UROLOGY 64 (2013) 228–243 TIMES [42] Lee et al. [45] MacDiarmid et al. [45] VICTOR [48] ADAM [49] ASSIST [50] TAABO [53] a1-Blocker alone, % Side effects (dry mouth) Trial a1-Blocker = a1-adrenoceptor antagonist; ADAM = Add-on study of Detrol LA to Alpha-blockers in men; ASSIST = Add-on therapy of Solifenacin Succinate in men for BPH with OAB symptoms treated by Tamsulosin; BPH = benign prostatic hyperplasia; IPSS = International Prostate Symptom Score; LUTS = lower urinary tract symptoms; n.r. = not reported; OAB = overactive bladder; PVR = postvoid residual; PSA = prostate-specific antigen; Qmax = maximum flow rate of urine; TAABO = Trial of combination treatment of an Alpha-blocker plus an Anticholinergic for BPH with OAB; TIMES = Tolterodine and Tamsulosin in men with LUTS; VICTOR = Vesicare in combination with Tamsulosin in OAB residual symptoms. * Clinically significant increase in PVR depending on the study, defined as increase requiring catheterization or increase >300 ml or increase >50% of initial PVR or over the initially defined PVR threshold for exclusion. 239 240 EUROPEAN UROLOGY 64 (2013) 228–243 PDE5-I and a1-blocker is safe, and slight hemodynamic changes seem to be of no clinical relevance [55–59]. Kaplan et al. compared the daily use of alfuzosin, sildenafil, or the combination of the two in 62 patients with LUTS and ED. Alfuzosin reduced IPSS by 15.6%, sildenafil reduced IPSS by 11.8%, and the combination reduced IPSS by 24.1%. These differences were only significant when compared to baseline; they were not significant between groups. Alfuzosin and the combination with sildenafil increased Qmax by 11.7% and 21.1%, respectively, whereas sildenafil alone increased Qmax by only 6.2%, a difference without statistical significance. There appeared to be no differences between groups regarding AEs [60]. In 66 patients with LUTS/BPH and ED treated for 12 wk with either alfuzosin, tadalafil, or the combination, the latter showed significantly greater increase in IPSS (41.6%), Qmax (29.6%), and QoL (49.5%) than either monotherapy (alfuzosin alone: 27.2%, 21.7%, and 27.2%, respectively; tadalafil alone: 8.4%, 9.5%, and 28.8%, respectively), but again, these differences lacked statistical significance between groups [61]. In a crossover pilot study, 30 patients with LUTS/BPH (but not necessarily with concomitant ED) experienced higher IPSS reductions with tamsulosin/tadalafil (9.2 points) than with tamsulosin/placebo (6.7 points); this difference was significant compared to the baseline and between the groups [62]. The meta-analysis of these studies, which also included some additional pilot studies [63,64], evaluated a total of 278 patients with PDE5-I/a1-blocker combination therapy [54] and demonstrated increases of IPSS (1.8 points), International Index of Erectile Function (3.6 points), and Qmax (1.5 ml/s) when compared to a1-blockers alone. AEs with combination therapy occurred in 6.8% of patients and in 5.1% of patients receiving a1-blockers. Overall, there were no serious AEs, and combination treatment was well tolerated [54]. Treating LUTS and ED concurrently is already possible by tadalafil monotherapy (it was recently approved for that specific indication). This aspect seems particularly interesting because, according to the Multinational Survey of the Aging Male-7, 60–80% of patients suffering from BPH/LUTS are simultaneously affected by ED [65]. Improvement in symptoms of LUTS has been shown with PDE5-I, either alone or in combination with a1-blockers. However, whether the a1-blocker/PDE5-I combination is more efficacious in the treatment of LUTS ED is still to be elucidated. 3.4. Currently, none of these combination therapies have been recommended for the treatment of patients in clinical routine. 4. Conclusions The number of adequate and high-level clinical trials assessing combination therapy in male LUTS is surprisingly low. The a1-blocker/5-ARI combination has been examined the most thoroughly and provides sufficient scientific evidence for the treatment of particular patient groups. This combination appears to supersede either monotherapy where longterm treatment is intended (>1 yr). Patients with an enlarged prostate (volume >30–40 ml) and who are high risk for disease progression benefit most from this combination therapy. It remains unknown if the favorable effects of combination therapy are maintained when treatment is continued for >6 yr. Effects of 5-ARI on PCa screening and diagnosis should be considered. The present review did not include cost-effectiveness analyses of a1-blocker/5-ARI combinations, which might be of relevance in some countries [72,73]. The a1-blocker/antimuscarinic combination was mostly assessed as add-on therapy to a1-blocker therapy. This is in line with the target group, which comprises men with persistent symptoms after a1-blocker therapy. The combination therapy is a second-line, add-on treatment rather than a first-line treatment. Exclusion of patients with an increased risk of AEs (eg, high PVR) in existing studies weakens the informative value on AUR occurrence. In patients with increased PVR, an a1-blocker/antimuscarinic combination should be used with caution and regular measurements of PVR is advised. Currently, there is no scientific evidence that a1-blocker/antimuscarinic combination therapy is efficacious or safe when used for >4 mo. Only preliminary reports exist on the a1-blocker/PDE5-I combination therapy. Further research should explore if a 5-ARI is just as effective as an a1-blocker/5-ARI combination on a long-term basis (>6 yr), and at what time point the a1-blocker should be omitted. Studies on a1-blocker/ antimuscarinic combinations should verify the long-term safety and efficacy of this combination. Larger and longer studies are needed to assess the value of PDE5-I combinations. Combinations of 5-ARI/antimuscarinics, 5-ARI/PDE5I, antimuscarinics/PDE5-I, or even triple therapy might be of value for certain patients. Other combinations Author contributions: Kevin T. McVary had full access to all the data in Only one RCT was identified that assessed the combination of saw palmetto, a plant extract, with tamsulosin (the Tamsulosin With or Without Serenoa repens in Benign Prostatic Hyperplasia [OCOS] trial) [66]. Although the value of saw palmetto in the treatment of LUTS remains ambiguous [67], the study did not report a significant advantage for combination therapy. Other combinations, with antiinflammatory drugs, antihypertensive drugs, and statins or 5-ARIs/antimuscarinics, for example, are still experimental and have included only small study populations [68–71]. the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: Roehrborn, Marberger, McVary, Stief, Oelke, Füllhase, Novara, Chapple. Acquisition of data: Oelke, Füllhase, De Nunzio. Analysis and interpretation of data: Porst, Roehrborn, Marberger, McVary, Oelke, Füllhase, Chapple, Gratzke, Kaplan. Drafting of the manuscript: McVary, Stief, Oelke, Füllhase, Chapple. Critical revision of the manuscript for important intellectual content: Porst, Roehrborn, Marberger, McVary, Stief, Oelke, Novara, Cornu, De Nunzio, Chapple, Gratzke, Kaplan. 241 EUROPEAN UROLOGY 64 (2013) 228–243 Statistical analysis: None. [11] Howick J, Chalmers I, Glasziou P., OCEBM Levels of Evidence Working Obtaining funding: None. Group. 2011 levels of evidence system. Centre for Evidence Based Administrative, technical, or material support: Oelke, Gratzke, Kaplan. Medicine Supervision: Roehrborn, McVary, Oelke, Chapple. Accessed May 1, 2012. Other (specify): None. Web site. http://www.cebm.net/index.aspx?o=5513. [12] Jones J, Hunter D. Consensus methods for medical and health services research. BMJ 1995;311:376–80. Financial disclosures: Kevin T. McVary certifies that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: Kevin McVary has been a consultant, investigator, and speaker for Eli Lilly and Company and Bayer Healthcare. Matthias Oelke has received lecturer and/or consultant honoraria in the field of male LUTS from Astellas, GlaxoSmithKline, Lilly, Pfizer, Recordati, and Sophiris. Giacomo Novara has served as an advisory board member, consultant, researcher, and speaker for Astellas, GlaxoSmithKline, Lilly, Pierre Fabre, Recordati, and Takeda. Jean-Nicolas Cornu has been a consultant for Pfizer and Takeda. Christopher Chapple has been a consultant for AMS and Lilly, a consultant and researcher for ONO, and a consultant, researcher, and speaker for Allergan, Astellas, Pfizer, and Recordati. Support and role of the sponsor: None. [13] Okada H, Kawaida N, Ogawa T, Arakawa S, Matsumoto O, Kamidono S. Tamsulosin and chlormadinone for the treatment of benign prostatic hyperplasia. The Kobe University YM617 Study Group. Scand J Urol Nephrol 1996;30:379–85. [14] Kuo HC. Comparative study of therapeutic effect of dibenyline, finasteride, and combination drugs for symptomatic benign prostatic hyperplasia. Urol Int 1998;60:85–91. [15] Lepor H, Williford WO, Barry MJ, et al. The efficacy of terazosin, finasteride, or both in benign prostatic hyperplasia. Veterans Affairs Cooperative Studies Benign Prostatic Hyperplasia Study Group. N Engl J Med 1996;335:533–9. [16] Lepor H, Williford WO, Barry MJ, Haakenson C, Jones K. The impact of medical therapy on bother due to symptoms, quality of life and global outcome, and factors predicting response. Veterans Affairs Cooperative Studies Benign Prostatic Hyperplasia Study Group. J Urol 1998;160:1358–67. [17] Debruyne FMJ, Jardin A, Colloi D, et al. Sustained-release alfuzosin, finasteride and the combination of both in the treatment of benign References prostatic hyperplasia. European ALFIN Study Group. Eur Urol 1998; 34:169–75. [1] Abrams P, Cardozo L, Fall M, et al. The standardisation of terminol- [18] Johnson II TM, Jones K, Williford WO, Kutner MH, Issa MM, Lepor H. ogy in lower urinary tract function: report from the standardisation Changes in nocturia from medical treatment of benign prostatic sub-committee of the International Continence Society. Urology hyperplasia: secondary analysis of the Department of Veterans 2003;61:37–49. Affairs Cooperative Study Trial. J Urol 2003;170:145–8. [2] Verhamme KMC, Dieleman JP, Bleumink GS, van der Lei J, [19] McConnell JD, Roehrborn CG, Bautista OM, et al. The long-term Sturkenboom MCJM, Triumph Pan European Expert Panel. Inci- effect of doxazosin, finasteride, and combination therapy on the dence and prevalence of lower urinary tract symptoms suggestive clinical progression of benign prostatic hyperplasia. N Engl J Med of benign prostatic hyperplasia in primary care—the Triumph project. Eur Urol 2002;42:323–8. [3] Boyle P, Robertson C, Mazzetta C, et al. The prevalence of lower urinary tract symptoms in men and women in four centres. The UrEpik study. BJU Int 2003;92:409–14. 2003;349:2387–98. [20] Johnson II TM, Burrows PK, Kusek JW, et al. The effect of doxazosin, finasteride and combination therapy on nocturia in men with benign prostatic hyperplasia. J Urol 2007;178:2045–50, discussion 2050–1. [21] Kaplan SA, McConnell JD, Roehrborn CG, et al. Combination therapy [4] Coyne KS, Sexton CC, Thompson CL, et al. The prevalence of lower with doxazosin and finasteride for benign prostatic hyperplasia in urinary tract symptoms (LUTS) in the USA, the UK and Sweden: patients with lower urinary tract symptoms and a baseline total results from the Epidemiology of LUTS (EpiLUTS) study. BJU Int prostate volume of 25 ml or greater. J Urol 2006;175:217–20, 2009;104:352–60. discussion 220–1. [5] Irwin DE, Kopp ZS, Agatep B, Milsom I, Abrams P. Worldwide [22] Kirby RS, Roehrborn C, Boyle P, et al. Efficacy and tolerability of prevalence estimates of lower urinary tract symptoms, overactive doxazosin and finasteride, alone or in combination, in treatment bladder, urinary incontinence and bladder outlet obstruction. BJU of symptomatic benign prostatic hyperplasia: the Prospective Int 2011;108:1132–8. European Doxazosin and Combination Therapy (PREDICT) trial. [6] Irwin DE, Milsom I, Hunskaar S, et al. Population-based survey of Urology 2003;61:119–26. urinary incontinence, overactive bladder, and other lower urinary [23] Roehrborn CG, Siami P, Barkin J, et al. The effects of dutasteride, tract symptoms in five countries: results of the EPIC study. Eur Urol tamsulosin and combination therapy on lower urinary tract symp- 2006;50:1306–15, discussion 1314–5. toms in men with benign prostatic hyperplasia and prostatic en- [7] Roosen A, Chapple CR, Dmochowski RR, et al. A refocus on the bladder as the originator of storage lower urinary tract symptoms: a systematic review of the latest literature. Eur Urol 2009;56: 810–20. largement: 2-year results from the CombAT study. J Urol 2008; 179:616–21, discussion 621. [24] Roehrborn CG, Siami P, Barkin J, et al. The influence of baseline parameters on changes in international prostate symptom score with [8] Oelke M, Bachmann A, Descazeaud A, et al. EAU guidelines on the dutasteride, tamsulosin, and combination therapy among men with treatment and follow-up of non-neurogenic male lower urinary symptomatic benign prostatic hyperplasia and an enlarged prostate: tract symptoms including benign prostatic obstruction. Eur Urol 2013;64:118–40. 2-year data from the CombAT study. Eur Urol 2009;55:461–71. [25] Barkin J, Roehrborn CG, Siami P, et al. Effect of dutasteride, tamsu- [9] McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA guideline losin and the combination on patient-reported quality of life and on the management of benign prostatic hyperplasia. J Urol treatment satisfaction in men with moderate-to-severe benign 2011;185:1793–803. prostatic hyperplasia: 2-year data from the CombAT trial. BJU Int [10] Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 2009;62:1006–12. 2009;103:919–26. [26] Chung BH, Roehrborn CG, Siami P, et al. Efficacy and safety of dutasteride, tamsulosin and their combination in a subpopulation 242 EUROPEAN UROLOGY 64 (2013) 228–243 of the CombAT study: 2-year results in Asian men with moderateto-severe BPH. Prostate Cancer Prostatic Dis 2009;12:152–9. pollakiuria and/or urinary incontinence. Jpn J Urol Surg 1999;12: 525–36. [27] Becher E, Roehrborn CG, Siami P, Gagnier RP, Wilson TH, Montorsi F. [41] Lee KS, Choo MS, Kim DY, et al. Combination treatment with The effects of dutasteride, tamsulosin, and the combination on propiverine hydrochloride plus doxazosin controlled release storage and voiding in men with benign prostatic hyperplasia and gastrointestinal therapeutic system formulation for overactive prostatic enlargement: 2-year results from the Combination of Avo- bladder and coexisting benign prostatic obstruction: a prospec- dart and Tamsulosin study. Prostate Cancer Prostatic Dis 2009; tive, randomized, controlled multicenter study. J Urol 2005;174: 12:369–74. 1334–8. [28] Roehrborn CG, Siami P, Barkin J, et al. The effects of combination [42] Kaplan SA, Roehrborn CG, Rovner ES, Carlsson M, Bavendam T, therapy with dutasteride and tamsulosin on clinical outcomes in Guan Z. Tolterodine and tamsulosin for treatment of men men with symptomatic benign prostatic hyperplasia: 4-year with lower urinary tract symptoms and overactive bladder: a results from the CombAT study. Eur Urol 2010;57:123–31. randomized controlled trial. JAMA 2006;296:2319–28. [29] Montorsi F, Henkel T, Geboers A, et al. Effect of dutasteride, tam- [43] Rovner ES, Kreder K, Sussman DO, et al. Effect of tolterodine sulosin and the combination on patient-reported quality of life and extended release with or without tamsulosin on measures of treatment satisfaction in men with moderate-to-severe benign urgency and patient reported outcomes in men with lower urinary prostatic hyperplasia: 4-year data from the CombAT study. Int J Clin Pract 2010;64:1042–51. tract symptoms. J Urol 2008;180:1034–41. [44] Roehrborn CG, Kaplan SA, Kraus SR, Wang JT, Bavendam T, Guan Z. [30] Montorsi F, Roehrborn C, Garcia-Penit J, et al. The effects of dutaste- Effects of serum PSA on efficacy of tolterodine extended release ride or tamsulosin alone and in combination on storage and voiding with or without tamsulosin in men with LUTS, including OAB. symptoms in men with lower urinary tract symptoms (LUTS) and Urology 2008;72:1061–7, discussion 1067. benign prostatic hyperplasia (BPH): 4-year data from the Combi- [45] MacDiarmid SA, Peters KM, Chen A, et al. Efficacy and safety of nation of Avodart and Tamsulosin (CombAT) study. BJU Int 2011; extended-release oxybutynin in combination with tamsulosin for 107:1426–31. treatment of lower urinary tract symptoms in men: randomized, [31] Roehrborn CG, Barkin J, Siami P, et al. Clinical outcomes after combined therapy with dutasteride plus tamsulosin or either double-blind, placebo-controlled study. Mayo Clin Proc 2008; 83:1002–10. monotherapy in men with benign prostatic hyperplasia (BPH) by [46] Kaplan SA, Roehrborn CG, Chancellor M, Carlsson M, Bavendam T, baseline characteristics: 4-year results from the randomized, Guan Z. Extended-release tolterodine with or without tamsulosin double-blind Combination of Avodart and Tamsulosin (CombAT) in men with lower urinary tract symptoms and overactive bladder: trial. BJU Int 2011;107:946–54. effects on urinary symptoms assessed by the International Prostate [32] Barkin J, Guimarães M, Jacobi G, Pushkar D, Taylor S, van Symptom Score. BJU Int 2008;102:1133–9. Vierssen Trip OB. a-Blocker therapy can be withdrawn in the [47] Roehrborn CG, Kaplan SA, Jones JS, Wang JT, Bavendam T, Guan Z. majority of men following initial combination therapy with the Tolterodine extended release with or without tamsulosin in men dual 5alpha-reductase inhibitor dutasteride. Eur Urol 2003;44: with lower urinary tract symptoms including overactive bladder 461–6. symptoms: effects of prostate size. Eur Urol 2009;55:472–81. [33] Rosen RC, Wei JT, Althof SE, Seftel AD, Miner M, Perelman MA. [48] Kaplan SA, McCammon K, Fincher R, Fakhoury A, He W. Safety Association of sexual dysfunction with lower urinary tract symp- and tolerability of solifenacin add-on therapy to alpha-blocker toms of BPH and BPH medical therapies: results from the BPH treated men with residual urgency and frequency. J Urol 2009; Registry. Urology 2009;73:562–6. 182:2825–30. [34] Nickel JC, Barkin J, Koch C, Dupont C, Elhilali M. Finasteride mono- [49] Chapple C, Herschorn S, Abrams P, Sun F, Brodsky M, Guan Z. therapy maintains stable lower urinary tract symptoms in men Tolterodine treatment improves storage symptoms suggestive of with benign prostatic hyperplasia following cessation of alpha overactive bladder in men treated with a-blockers. Eur Urol blockers. Can Urol Assoc J 2008;2:16–21. 2009;56:534–43. [35] Andriole GL, Bostwick DG, Brawley OW, et al. Effect of dutaste- [50] Yamaguchi O, Kakizaki H, Homma Y, et al. Solifenacin as add-on ride on the risk of prostate cancer. N Engl J Med 2010;362: therapy for overactive bladder symptoms in men treated for lower 1192–202. urinary tract symptoms—ASSIST, randomized controlled study. [36] Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med 2003;349:215–24. Urology 2011;78:126–33. [51] Chapple CR, Herschorn S, Abrams P, Wang JT, Brodsky M, Guan Z. Efficacy and safety of tolterodine extended-release in men with [37] US Food and Drug Administration. FDA Drug Safety Communica- overactive bladder symptoms treated with an alpha-blocker: effect tion: 5-alpha reductase inhibitors (5-ARIs) may increase the risk of of baseline prostate-specific antigen concentration. BJU Int 2010; a more serious form of prostate cancer. US Food and Drug Administration Web site. http://www.fda.gov/Drugs/DrugSafety/ ucm 258314.htm. Accessed May 1, 2012. 106:1332–8. [52] Oelke M, Murgas S, Baumann I, Schnabel F, Michel MC. Efficacy of propiverine ER with or without alpha-blockers related to maximum [38] Marberger M, Freedland SJ, Andriole GL, et al. Usefulness of urinary flow rate in adult men with OAB: results of a 12-week, prostate-specific antigen (PSA) rise as a marker of prostate cancer multicenter, non-interventional study. World J Urol 2011;29: in men treated with dutasteride: lessons from the REDUCE study. BJU Int 2012;109:1162–9. 217–23. [53] Nishizawa O, Yamaguchi O, Takeda M, Yokoyama O. Randomized [39] Thompson IM, Chi C, Ankerst DP, et al. Effect of finasteride on the controlled trial to treat benign prostatic hyperplasia with sensitivity of PSA for detecting prostate cancer. J Natl Cancer Inst overactive bladder using an alpha-blocker combined with anticho- 2006;98:1128–33. linergics. LUTS 2011;3:29–35. [40] Saito H, Yamada T, Oshima H, et al. A comparative study of the [54] Gacci M, Corona G, Salvi M, et al. A systematic review and meta- efficacy and safety of tamsulosin hydrochloride (Harnal capsules) analysis on the use of phosphodiesterase 5 inhibitors alone or in alone and in combination with propiverine hydrochloride (BUP-4 combination with a-blockers for lower urinary tract symptoms due tablets) in patients with prostatic hypertrophy associated with to benign prostatic hyperplasia. Eur Urol 2012;61:994–1003. EUROPEAN UROLOGY 64 (2013) 228–243 243 [55] Giuliano F, Kaplan SA, Cabanis MJ, Astruc B. Hemodynamic inter- [64] Tuncel A, Nalcacioglu V, Ener K, Aslan Y, Aydin O, Atan A. Sildenafil action study between the alpha1-blocker alfuzosin and the citrate and tamsulosin combination is not superior to monotherapy phosphodiesterase-5 inhibitor tadalafil in middle-aged healthy in treating lower urinary tract symptoms and erectile dysfunction. male subjects. Urology 2006;67:1199–204. World J Urol 2010;28:17–22. [56] Auerbach SM, Gittelman M, Mazzu A, Cihon F, Sundaresan P, [65] Rosen R, Altwein J, Boyle P, et al. Lower urinary tract symptoms and White WB. Simultaneous administration of vardenafil and tamsu- male sexual dysfunction: the multinational survey of the aging losin does not induce clinically significant hypotension in patients with benign prostatic hyperplasia. Urology 2004;64:998–1003, discussion 1003–4. [57] Kloner RA, Jackson G, Emmick JT, et al. Interaction between the phosphodiesterase 5 inhibitor, tadalafil and 2 alpha-blockers, doxazosin and tamsulosin in healthy normotensive men. J Urol 2004;172:1935–40. male (MSAM-7). Eur Urol 2003;44:637–49. [66] Glemain P, Coulange C, Billebaud T, Gattegno B, Muszynski R, Loeb G. Tamsulosin with or without Serenoa repens in benign prostatic hyperplasia: the OCOS trial [in French]. Prog Urol 2002; 12:395–403, discussion 404. [67] Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med 2006;354:557–66. [58] Ng CF, Wong A, Cheng CW, Chan ES, Wong HM, Hou SM. Effect of [68] Di Silverio F, Bosman C, Salvatori M, et al. Combination therapy vardenafil on blood pressure profile of patients with erectile dysfunc- with rofecoxib and finasteride in the treatment of men with lower tion concomitantly treated with doxazosin gastrointestinal therapeu- urinary tract symptoms (LUTS) and benign prostatic hyperplasia tic system for benign prostatic hyperplasia. J Urol 2008;180: 1042–6. (BPH). Eur Urol 2005;47:72–9, discussion 78–9. [59] Nieminen T, Tammela TL, Koobi T, Kahonen M. The effects of [69] Ozdemir I, Bozkurt O, Demir O, Aslan G, Esen AA. Combination tamsulosin and sildenafil in separate and combined regimens on therapy with doxazosin and tenoxicam for the management of detailed hemodynamics in patients with benign prostatic enlargement. J Urol 2006;176:2551–6. lower urinary tract symptoms. Urology 2009;74:431–5. [70] Liu H, Liu P, Mao G, et al. Efficacy of combined amlodipine/terazosin [60] Kaplan SA, Gonzalez RR, Te AE. Combination of alfuzosin and silden- therapy in male hypertensive patients with lower urinary tract afil is superior to monotherapy in treating lower urinary tract symp- symptoms: a randomized, double-blind clinical trial. Urology toms and erectile dysfunction. Eur Urol 2007;51:1717–23. 2009;74:130–6. [61] Liguori G, Trombetta C, De Giorgi G, et al. Efficacy and safety of [71] Chung DE, Te AE, Staskin DR, Kaplan SA. Efficacy and safety of combined oral therapy with tadalafil and alfuzosin: an integrated tolterodine extended release and dutasteride in male overactive approach to the management of patients with lower urinary tract bladder patients with prostates >30 grams. Urology 2010;75: symptoms and erectile dysfunction. Preliminary report. J Sex Med 2009;6:544–52. 1144–8. [72] Verheggen BG, Lee R, Lieuw On MM, et al. Estimating the quality-of- [62] Bechara A, Romano S, Casabe A, et al. Comparative efficacy assess- life impact and cost-effectiveness of alpha-blocker and anti- ment of tamsulosin vs. tamsulosin plus tadalafil in the treatment of muscarinic combination treatment in men with lower urinary tract LUTS/BPH. Pilot study. J Sex Med 2008;5:2170–8. symptoms related to benign prostatic hyperplasia and overactive [63] Jin Z, Zhang ZC, Liu JH, et al. An open, comparative, multicentre bladder. J Med Econ 2012;15:586–600. clinical study of combined oral therapy with sildenafil and [73] Bjerklund Johansen TE, Baker TM, Black LK. Cost-effectiveness doxazosin GITS for treating Chinese patients with erectile dysfunc- of combination therapy for treatment of benign prostatic tion and lower urinary tract symptoms secondary to benign pros- hyperplasia: a model based on the findings of the Combination tatic hyperplasia. Asian J Androl 2011;13:630–5. of Avodart and Tamsulosin trial. BJU Int 2012;109:731–8.