Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
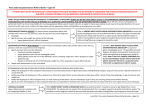
Upper GI Fast Track Referral – 2 Week Wait Please refer via the e-Referral Service Patient Details: Patient Name Address DOB Home Tel. No. Mobile Tel. No. Preferred Tel. No. Main Spoken Language Transport needed? NHS No. Gender Ethnicity Email Address Interpreter needed? Registered GP Details: Practice Name Registered GP Registered GP Address Tel No. Email Usual GP Fax No. Practice Code Please use separate children’s proforma for patients under 16 Dear Colleague, I would be grateful for your opinion on the patient named above who presents with clinical findings I consider suspicious of malignancy. I have discussed the possibility of cancer with this patient. Has the patient confirmed that they can be available to attend an appointment within the next two weeks? Yes No Order urgent direct access OGD (follow Gastroscopy Flow Chart v1.0 for decision making see below page 6) Tick if Criteria applies Dysphagia Aged ≥55y with weight loss with any of; Upper abdominal pain Reflux/ Dyspepsia Consider non – urgent direct access OGD (follow Gastroscopy Flow Chart v1.0 for decision making see below page 6) Tick if Criteria applies Haematemesis Aged ≥ 55y with: Treatment resistant dyspepsia Upper abdominal pain and low haemoglobin Raised platelet count AND any of; o Nausea o Vomiting o Weight loss o Reflux Form to be reviewed annually Page 1 of 5 Revised: August 2016 o Dyspepsia o Upper abdominal pain Nausea and vomiting AND any of; o Weight loss o Reflux o Dyspepsia o Upper abdominal pain Consider urgent direct access CT scan (or urgent USS if CT not available) Tick if Criteria applies ≥60y with weight loss and any of: Diarrhoea Back pain Abdominal pain Nausea/vomiting Constipation New onset diabetes Tick if Criteria Consider urgent direct access USS applies Upper abdominal mass consistent with an enlarged gallbladder Upper abdominal mass consistent with an enlarged liver Tick if Criteria 2ww Referral if: applies OGD findings suggest Oesophageal or gastric cancer CT or USS findings suggest Pancreatic cancer Refer using suspected cancer pathway if aged ≥40y and have jaundice (The evidence did not distinguish obstructive jaundice. Other causes of jaundice were considered more likely if <40y) USS findings suggest Gallbladder cancer USS findings suggest Liver cancer Clinical Information Medical History Current Medications Form to be reviewed annually Page 2 of 5 Revised: August 2016 Known Allergies Family History Patient Anxiety Level Patient information and support needs Information given to the patient Other information WHO performance status: (please tick) 0 – normal activity 1 – restrictive light work 2 – self-care but no work > 50% of working day 3 – limited self-care – confined to bed/chair > 50% of waking day 4 – completely disabled – totally confined to bed/chair To be completed by the Data Team Date of decision to refer Date of appointment Date of earliest offered appointment (if different to above) Specify reason if not seen at earliest offered appointment Periods of unavailability Booking number (UBRN) Final Diagnosis: Form to be reviewed annually Malignant Benign Page 3 of 5 Revised: August 2016 Summary of the NICE 2015 suspected cancer guidelines Gastrointestinal cancers Oesophageal and gastric cancer Consider cancer Upper abdominal mass consistent with stomach cancer. pathway referral Urgent direct Dysphagia access OGD Aged ≥55y with weight loss with any of upper abdominal pain/reflux/dysphagia. Consider nonurgent direct access OGD Pancreatic cancer Refer via cancer pathway Consider urgent direct access CT scan (or urgent USS if CT not available) Haematemesis (Clearly use your clinical judgement here!) Aged ≥55y with: o Treatment resistant dyspepsia. o Upper abdominal pain and low haemoglobin o Raised platelet count AND any of nausea/vomiting/weight loss/reflux/dyspepsia/upper abdominal pain. o Nausea and vomiting AND any of weight loss/reflux/ dyspepsia/upper abdominal pain. Refer using suspected cancer pathway if aged ≥40y and have jaundice. (The evidence did not distinguish obstructive from nonobstructive jaundice. Other causes of jaundice were considered more likely if <40y) ≥60y with weight loss and any of: o Diarrhoea. o Back pain. o Abdominal pain. o Nausea/vomiting. o Constipation. o New onset diabetes. (USS only images the head of the pancreas, CT images the whole pancreas and may detect other cancers.) Gallbladder cancer Consider urgent direct access USS Liver Cancer Consider urgent direct access USS Form to be reviewed annually Upper abdominal mass consistent with an enlarged gallbladder. Upper abdominal mass consistent with an enlarged liver. Page 4 of 5 Revised: August 2016 Form to be reviewed annually Page 5 of 5 Revised: August 2016