Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
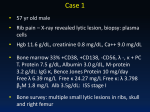
Cancer Therapy: Clinical A Phase I Trial of Lenalidomide in Patients with Recurrent Primary Central Nervous SystemTumors Howard A. Fine,1 Lyndon Kim,1 Paul S. Albert,3 J. Paul Duic,1 Hilary Ma,1 Wei Zhang,1 Tanyifor Tohnya,2 William D. Figg,2 and Cheryl Royce1 Abstract Purpose: Inhibition of angiogenesis represents a promising new therapeutic strategy for treating primary malignant brain tumors. Lenalidomide, a potent analogue of the antiangiogenic agent thalidomide, has shown significant activity in several hematologic malignancies, and therefore we chose to explore its tolerability and activity in patients with primary central nervous system tumors. Experimental Design: A phase I interpatient dose escalation trial of lenalidomide in patients with recurrent primary central nervous system tumors was conducted. Results: Thirty-six patients were accrued to the study, of which 28 were evaluable for toxicity, the primary end point of the trial. We show that lenalidomide can be given safely up to doses of 20 mg/m2, with the only toxicity being a probable increased risk of thromboembolic disease. Pharmacokinetic studies reveal good bioavailability, linear kinetics, and no effects of enzymeinducing antiepileptic drugs on the metabolism of lenalidomide. No objective radiographic responses were seen in any of the treated patients. In the group of 24 patients with recurrent glioblastoma, the median time to tumor progression was <2 months and only 12.5% of patients were progression-free at 6 months. Conclusion: Lenalidomide is well tolerated in patients with recurrent glioma in doses up to 20 mg/m2. Treatment may be associated with an increased risk of thromboembolic disease. Preliminary data suggest that single agent activity may be limited in patients with recurrent glioblastoma at the doses evaluated although larger studies will be needed to confirm these observations. Despite recent advances in neurosurgery, radiotherapy, and chemotherapy, the prognosis of patients with malignant gliomas remains poor (1). With the failure of most standard cytotoxic agents to dramatically alter the course of this disease, there is an increasing interest in developing new therapeutics with novel mechanisms of action. Preclinical and clinical studies have shown that gliomas are highly angiogenic and that antiangiogenic therapy represents a potentially promising new therapeutic strategy (2 – 7). Thalidomide was one of the first oral antiangiogenic agents evaluated in patients with recurrent malignant gliomas (8). As a single agent, thalidomide showed cytostatic activity against gliomas, as reflected by stabilization of disease in some patients (9). Unfortunately, ‘‘responses’’ to thalidomide were generally Authors’ Affiliations: 1Neuro-Oncology Branch and 2Medical Oncology Branch, National Cancer Institute; and 3Biometric Research Branch, The National Institute of Neurological Disorders and Stroke, Bethesda, Maryland Received 6/22/07; revised 8/29/07; accepted 9/7/07. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Requests for reprints: Howard A. Fine, Neuro-Oncology Branch, National Cancer Institute, 9030 Old Georgetown Road, Bethesda, MD 20892. Phone: 301-4026383; Fax: 301-480-2246; E-mail: hfine@ mail.nih.gov. F 2007 American Association for Cancer Research. doi:10.1158/1078-0432.CCR-07-1546 www.aacrjournals.org short-lived, leading to the search for similar but potentially more clinically active agents. Lenalidomide (Revlimid, CC-5013) is a potent thalidomide analogue based on in vitro anti-inflammatory and immunomodulatory assays (10 – 13). Lenalidomide has shown significant antitumor activity in patients with multiple myeloma and myelodysplastic syndrome with chromosome 5q deletions (14 – 18). Secondary to lenalidomide safety profile, proven activity in several other cancers, and the possible antiglioma activity of thalidomide, we elected to evaluate lenalidomide in patients with recurrent gliomas. Patients and Methods Study population and eligibility criteria. Patients 18 years or older with histologically confirmed diagnosis of progressive or recurrent primary central nervous system tumors who had failed prior radiation therapy were eligible for the study. Evaluable disease on magnetic resonance imaging scan, a Karnofsky performance status of z60%, and normal hematologic, liver, and renal function were required. The number or types of prior treatment regimens was not an exclusion criterion except for patients who had prior therapy with thalidomide. All participants signed a written informed consent approved by the National Cancer Institute Institutional Review Board. Treatment. Each 4-week treatment cycle consisted of lenalidomide administered p.o. once daily for 3 weeks followed by a 1-week rest period. A complete physical and neurologic examination was done 7101 Clin Cancer Res 2007;13(23) December 1, 2007 Downloaded from clincancerres.aacrjournals.org on August 11, 2017. © 2007 American Association for Cancer Research. Cancer Therapy: Clinical every 2 weeks for the first cycle and every 4 weeks thereafter. A magnetic resonance imaging scan was done before each cycle to assess response. Patients with stable or responding disease based on clinical and radiographic assessment continued on to an additional cycle of treatment. Three patients per dose level were treated, and if no dose-limiting toxicity (DLT) occurred, three subsequent patients were enrolled in the next higher dose. If, however, a DLT was encountered, three more patients would be added to that group. The maximum tolerated dose was considered to have been exceeded in the event of two DLTs (any drug-related nonhematologic grade z3 or hematologic grade z4 toxicity) in any given dose level. The six dose levels were 2.5, 5, 8, 11, 15, and 20 mg/m2/d. Based on existing data showing severe and life-threatening neutropenia with doses >40 mg/d, the maximum total daily dose was predetermined to be <40 mg. DLT was defined for only the first cycle of therapy (4 weeks) and patients had to have at least 4 weeks of treatment to be evaluable for toxicity and DLT. Patients were stratified into those not on enzyme-inducing antiepileptic drugs (EIAED; group A) and those on EIAED (group B), with each group proceeding through dose escalation independently. After the pharmacokinetic data from patients on the second dose level revealed that EIAEDs had no effects on lenalidomide metabolism, the protocol was amended to place all subsequent patients into a single stratum. Pharmacokinetic evaluation. Serial blood samples for the determination of lenalidomide were collected on the 1st and 15th days of the first cycle. Plasma concentrations of lenalidomide were measured using a high-performance liquid chromatography-mass spectrometry method and analyzed as previously described (19). Statistical considerations. The primary end point was to evaluate the toxicity and pharmacokinetics of lenalidomide in this dose-escalating phase I study. Using the dose escalation scheme described above, the probability of escalating to the next dose level, based on the true rate of DLT at the current dose, is given by the following (each group was considered independent of the other): True toxicity at a given dose Probability of escalating 10% 20% 30% 40% 50% 60% 0.91 0.71 0.49 0.31 0.17 0.08 Thus, if the true underlying proportion of DLTs is 50% at the current dose, there was a 17% chance of escalating to the next dose. The progression-free survival (PFS) and overall survival rate were estimated according to the method of Kaplan and Meier. Pharmacokinetic analysis. Any difference in dose-normalized AUC0-a between patients with and without coadministration of EIAEDs was determined by Mann-Whitney U test. Kruskal-Wallis one-way ANOVA was used to determine differences in CL/F (and dose-normalized AUC0-a) as dose was increased. Linear regression analysis was carried out on AUC0-a to determine dose proportionality. A Wilcoxon signedrank test was also used to determine if the ratio of accumulation is equal to 1.0. Statistical evaluations were done on the NCSS 2001 software package (J.L. Hintze). Results Patients. A total of 36 patients were accrued to this trial (23 males, 13 females). The median age for patients in both groups was 48 years (range, 20-82 years). The median Karnofsky performance status was 90%. Tumor histology included 24 glioblastomas, 7 anaplastic gliomas, 3 low-grade gliomas, 1 meningioma, and 1 hemangioblastoma. All patients had recurrent disease following radiation therapy at a minimum. The median number of prior chemotherapy regimens was 2 (range, 0-6). Only patients who completed the first 4 weeks of treatment or patients who experienced a drug-related DLT before completion of the first 4 weeks of treatment were considered evaluable for DLT and maximum tolerated dose determination, the primary end point of the trial. Twenty-seven of 36 patients were therefore evaluable for the primary end point. Pharmacokinetic analysis. Twenty-four patients had complete pharmacokinetic sampling done (Table 1). There was no statistically significant difference in dose-normalized AUC0-1 (P = 0.8) evident between the patients on EIAEDs and those who were not, and thus the EIAED and non-EIAED treatment groups were combined for further pharmacokinetic and other analyses. No difference (P = 0.27) was observed in CL/F (and dose-normalized AUC0-a) as dose increased. In the dose range investigated (2.5-20 mg/m2), lenalidomide exhibited apparent linear pharmacokinetics. Linear regression analysis indicated a dose-proportional increase in AUC0-a with a good correlation (Fig. 1). The lenalidomide concentration-time profiles were very similar between patients (Fig. 2) and were characterized by a rapid absorption with mean T max of 1.0 h and a monophasic decline with mean terminal half-life of 3.9 h. Toxicities. Seven patients experienced clinical and radiographic progression before their first 4-week evaluation and were therefore evaluable for toxicity but not maximum tolerated dose determination. The drug was generally very well tolerated with only one observed DLT (see Table 2). There were only two episodes of grade 2 thrombocytopenia, one episode each of grade 2 and grade 3 neutropenia. The one grade 3 neutropenia occurred in a patient previously treated with high-dose Table 1. Mean (SD) pharmacokinetic variable estimates of lenalidomide Dose (mg/m2) Variables 2.5 AUC(0-1) (ngh/mL) C max (ng/mL) T max* (h) t 1/2 (h) CL/F (mL/min/m2) V d/F (L/m2) 316 89.8 0.9 3.2 169 38.9 (155) (49.2) (0.5-2) (1.8) (103) (12.1) 5 8 11 622 (333) 114 (56.0) 1.5 (1-2) 4.5 (5.5) 206 (182) 50.5 (36.9) 385 (261) 109 (84.9) 0.5 (0.5) 2.3 (0.4) 451 (307) 85.1 (45.3) 923 (479) 229 (145) 1.0 (1-2) 5.6 (4.4) 258 (148) 89.5 (29.1) 15 1055 (252) 409 (263) 1.0 (0.5-1) 2.2 (0.8) 247 (61.3) 45.8 (16.4) 20 942 210 0.5 2.5 354 77.8 *T max values are median (range). Clin Cancer Res 2007;13(23) December 1, 2007 7102 www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on August 11, 2017. © 2007 American Association for Cancer Research. Lenalidomide in Recurrent Central Nervous SystemTumors Fig. 1. Dose-proportional increase in AUC0-a. chemotherapy and autologous bone marrow support. Mild to moderate fatigue was seen in 13 patients. The only clinically significant infection was a case of herpes zoster keritoconjunctivitis. There were five cases of venous thrombosis (18% of evaluable patients) including a case of retinal vein thrombosis in the patient on lenalidomide for the longest time (24 months). Adverse events did not seem to be dose related. Clinical efficacy. Twenty-seven of 36 patients completed the first 3 weeks of treatment and were therefore evaluable or maximum tolerated dose determination. Of the nine patients not evaluable, seven had rapid disease progression, one had a DLT (herpes zoster), and one required a non – brain tumor and non – study-related surgical procedure. No patient had an objective radiographic response. The 6-month PFS for all 27 evaluable patients was 14.8% [95% confidence interval (95% CI), 6.0-36.6%; Fig. 3A]. The median time to progression for this group of patients was 1.74 months (95% CI, 1.6-3.4) and the overall 6-month survival for all evaluable patients was 45.8% (95% CI, 30.1-69.8%; Fig. 3B). The median survival time was 5.95 months (95% CI, 4.4-11.4). The 24 patients with glioblastoma, 17 of whom where evaluable for response, represented a more homogeneous subgroup to study. The 6-month PFS of these patients was 17.7% (95% CI, 6.3-49.3%) and the median time to progression is 1.84 months (95% CI, 1.7-4.6; Fig. 4A). The 6-month overall survival was 47.1% (95% CI, 28.4-77.9%) with a median survival of 5.95 months (95% CI, 4.4-11.4; Fig. 4B). Seven glioblastoma multiforme patients were not evaluable for the primary end points of this study because they had disease progression before the end of the first cycle. If we include these patients in the overall tumor efficacy cohort, the overall 6-month PFS was 12.5%. There was no apparent correlation between clinical outcome and dose of lenalidomide or pharmacokinetic profiles. prolonged disease stabilization in patients with recurrent gliomas. In patients with newly diagnosed glioblastoma, overall median survival was equivalent to that seen when carmustine is used in the postradiation adjuvant setting. The lack of clear convincing evidence of significant antiglioma activity, yet the hint of some clinical benefit, has led to the search for drug combinations incorporating thalidomide and more potent thalidomide analogues. Lenalidomide is a potent IMiDS (immunomodulatory drugs), a class of drugs that are structural and functional analogues of thalidomide. Lenalidomide has more immunomodulating and antiangiogenic activities than thalidomide in various preclinical assays (10, 12, 23, 24). The precise antiangiogenic mechanism of lenalidomide is unclear, although it has been shown that lenalidomide can inhibit vascular endothelial growth factor – , basic fibroblast growth factor – , and tumor necrosis factor-a – induced endothelial cell migration (11). Additionally, it has been suggested that thalidomide analogues like lenalidomide can inhibit tumorand stroma cell – mediated secretion of vascular endothelial growth factor and basic fibroblast growth factor in preclinical models of multiple myeloma (25). Thus, lenalidomide is a drug of interest to investigate in patients with malignant gliomas. Lenalidomide has shown significant activity in multiple myeloma and in myelodysplasia with chromosome 5q deletion (18). Dose and toxicity information from these trials may not, however, be relevant to brain tumor patients because bone marrow reserve is generally normal in these patients compared with those with hematologic malignancies. To this end, at least two single agent phase I trials of lenalidomide in patients with solid tumors have partially been reported. Bartlett et al. (13) conducted a phase I trial of lenalidomide in patients with solid tumors using an intrapatient weekly dose escalation schema of 2 mg/d escalating to 50 mg/d over 4 weeks, although treatment was formally suspended after 4 weeks secondary to toxicity. Thus, dose versus toxicity data were difficult to determine. Tohnya et al. (17) conducted a phase I trial of lenalidomide in patients with refractory solid tumors using a more standard modified Fibonacci design with dose escalation from 5 to 40 mg/d. The investigators observed a significant incidence of grade 1 and grade 2 fatigue, rash, nausea, myalgias, and neutropenia. A number of grade 3 and 4 toxicities, including neutropenia, resulted in modifying the Discussion Thalidomide has been evaluated in a number of phase II trials in patients with recurrent high-grade gliomas and in patients with newly diagnosed glioblastomas in combination with and following standard fractionated radiotherapy (9, 20 – 22). There was a suggestion of some antiglioma activity with a few minor radiographic responses and several cases of www.aacrjournals.org Fig. 2. Concentration-time profile for a patient with recurrent high-grade glioma on 11mg/m2 of oral lenalidomide. 7103 Clin Cancer Res 2007;13(23) December 1, 2007 Downloaded from clincancerres.aacrjournals.org on August 11, 2017. © 2007 American Association for Cancer Research. Cancer Therapy: Clinical Table 2. Toxicity Toxicity/adverse event Grade 2/3/4 Common Toxicity Criteria toxicity Dose level 1 Alanine aminotransferase Platelets Leukopenia Hypokalemia Neutropenia Thrombosis/vascular (DVT) Thrombocytopenia Hypophosphatemia Seizure Fatigue Vomiting Nausea Constipation Diarrhea Urinary tract infection Herpes zoster Keratitis Rash Dental abcess Retinal vein occlusion 2 3 4 5 6 1/0/0 1/0/0 1/0/0 0/2/0 1/0/0 0/1/0 1/1/0 0/1/0 1/0/0 1/0/0 3/0/1 1/1/0 2/0/0 5/0/0 1/1/0 1/1/0 2/0/0 2/0/1 1/0/0 0/1/0 2/1/0 5/0/0 1/1/0 0/1/0 0/1/0 0/1/0 2/0/0 1/0/0 1/0/0 treatment regimen to administering lenalidomide for 21 days on a 28-day cycle. Based on these and other trials showing that continuous dosing and higher doses of lenalidomide are not well tolerated, we designed our phase I trial to use the accepted 21 days on and 7 days off dose administration schedule. Our pharmacokinetic analysis revealed that lenalidomide exhibited rapid absorption and displayed relatively good linear kinetics relative to the dose administered and AUC. Additionally, no accumulation of drug in the plasma was observed after multiple doses due to the short terminal half-life of the agent. Finally, EIAEDs, known to induce CYP450 enzymes such as CYP3A4, did not have any effect on lenalidomide metabolism or exposure. We found that lenalidomide was well tolerated at all doses evaluated. Despite the relatively high doses of lenalidomide used in this trial, we did not observe the neutropenia commonly reported in other trials of lenalidomide. This likely reflects the fact that most glioma patients are less heavily pretreated with chemotherapy and thus have relatively better bone marrow reserve than patients with multiple myeloma and myelodysplastic syndrome, those patients most commonly treated with lenalidomide. Despite the immunosuppressive activity of lenalidomide, we did not see any significant clinical infections except for one case of herpes zoster of the trigeminal nerve. This infection, however, occurred in a patient on long-term, high-dose glucocorticoids, and thus the relationship of the infection to lenalidomide is uncertain. We did, however, observe five cases of venous thrombosis in patients treated with lenalidomide. Although thalidomide and lenalidomide are known to increase the risk of thromboembolic events in other disease settings, glioma patients are at inherent high risk of developing thromboembolic events independent of treatment (26). Thus, it is impossible to know for certain whether lenalidomide contributed to any of the thrombotic events observed in this trial. Nevertheless, the fact that 18% of patients experienced a Clin Cancer Res 2007;13(23) December 1, 2007 thromboembolic event during their relatively short duration of exposure to lenalidomide is of concern and strongly suggests a possible contribution of lenalidomide to the high thrombotic rate seen in this trial. Twenty-four glioblastoma patients with good performance status (i.e., potentially phase II trial eligible) were treated on this trial, allowing us to carry out an exploratory efficacy analysis of the data despite the fact that the trial was not formally designed to evaluate the antitumor efficacy of lenalidomide. Because there were no objective radiographic responses and no clear improvement in patient symptoms, PFS in conjunction with clinical stability was our major determinant of clinical benefit. As shown in Fig. 3A, the median PFS for all evaluable glioblastoma patients was 1.84 months and the 6-month PFS was 17.7%. If one includes all patients with glioblastoma, including those who had tumor progression during the first cycle, the 6-month PFS was 12.6% (Fig. 4A). This compares to a historical 15% and 9% 6-month PFS for patients accrued to phase I/II single institution and cooperative group trials of drugs subsequently determined to be inactive in glioblastoma, respectively (27, 28). Thus, these preliminary data are not encouraging for the antitumor activity of lenalidomide for recurrent glioblastoma. The lack of objective radiographic responses and a 6-month PFS of 12.5% are disappointing; however, it remains plausible that a study with a larger cohort of less heavily pretreated patients might give a more favorable outcome. Nevertheless, there are few data to suggest that prior exposure to standard chemotherapeutic agents (almost exclusively alkylating agents) lessens one’s likelihood of responding to an antiangiogenic agent. Indeed, one of our few long-term responders was one of our most heavily pretreated patients, having had four prior chemotherapeutic regimens before his enrollment on this trial. In addition to prior extensive prior treatment, another possible explanation for the low response rate is that most patients were treated at a dose of lenalidomide below the 7104 www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on August 11, 2017. © 2007 American Association for Cancer Research. Lenalidomide in Recurrent Central Nervous SystemTumors maximum tolerated dose. Nevertheless, a true dose-response relationship was not seen in our cohort of patients and has never been shown for thalidomide or lenalidomide. Indeed, one of the few long-term stable disease patients in this study was treated at our lowest dose (2.5 mg/m2). Given that all patients on this trial were treated at doses of lenalidomide that have proved active in lenalidomide-sensitive tumors, there is little compelling data to believe that dose escalations higher than the 20 mg/m2 we achieved in this trial would result in greater clinical benefit. Nevertheless, given the preliminary nature of our efficacy data, a larger formal phase II trial of lenalidomide in less heavily pretreated patients using the 20 mg/m2 dose, or a higher dose as yet to be established, might be considered reasonable. We were unable to identify any radiographic or clinical variables that could allow us to prospectively identify patients likely to benefit from lenalidomide. Because the true in situ antitumor and antiangiogenic mechanism of action of lenalidomide remains obscure, no obvious biological end points could be evaluated. Recently, it has been suggested that peripheral endothelial cell and endothelial cell progenitor cells may be surrogate end points of angiogenesis in vivo; however, these assays had not been identified at the time this trial was conducted. The utility of such assays may represent a potential area of exploration should additional trials of lenalidomide be conducted in patients with recurrent glioma. Fig. 4. A, PFS for evaluable glioblastoma multiforme (GBM) patients with 95% CIs. B, overall survival for evaluable glioblastoma multiforme patients with 95% CIs. Fig. 3. A, PFS for all evaluable patients with 95% CIs. B, overall survival for all evaluable patients with 95% CIs. www.aacrjournals.org The minimal antitumor efficacy of lenalidomide observed in our trial suggests that if lenalidomide ultimately does prove to have significant clinical activity, trials with large numbers of patients will likely be required to definitively show such modest activity in a statistically rigorous way. The extensive monetary and patient resources necessary for such a trial might be better used on definitive trials of other more highly active antiangiogenic agents that have recently shown significant radiographic responses and clinical benefit in ongoing clinical trials of patients with recurrent gliomas (i.e., bevacizumab). A more promising approach for the development of lenalidomide in gliomas might be to consider trials of lenalidomide in combination with other chemotherapeutic agents (i.e., temozolomide and nitrosoureas), although additive myelosuppresion may ultimately limit the utility of such combinations. In summary, lenalidomide is generally well tolerated in patients with recurrent primary central nervous system tumors at doses up to and including 20 mg/m2, with the only major toxicity being an increased risk of thromboembolic disease. Although confirmatory phase II data may be necessary, lenalidomide does not seem to be a highly effective single agent for patients with recurrent glioblastoma at the doses evaluated. Trials of lenalidomide in combination with other agents may be worth exploring. 7105 Clin Cancer Res 2007;13(23) December 1, 2007 Downloaded from clincancerres.aacrjournals.org on August 11, 2017. © 2007 American Association for Cancer Research. Cancer Therapy: Clinical References 1. DeAngelis LM. Brain tumors. N Engl J Med 2001;344: 114 ^ 23. 2. Plate KH, Breier G,Weich HA, et al.Vascular endothelial growth factor is a potential tumour angiogenesis factor in human gliomas in vivo. Nature 1992;359: 845 ^ 8. 3. Zagzag D, Miller DC, Sato Y, et al. Immunohistochemical localization of basic fibroblast growth factor in astrocytomas. Cancer Res 1990;50:7393 ^ 8. 4. Takahashi JA, Mori H, Fukumoto M, et al. Gene expression of fibroblast growth factors in human gliomas and meningiomas: demonstration of cellular source of basic fibroblast growth factor mRNA and peptide in tumor tissues. Proc Natl Acad Sci U S A 1990;87:5710 ^ 4. 5. Millauer B, Shawver LK, Plate KH, et al. Glioblastoma growth inhibited in vivo by a dominant-negative Flk-1 mutant. Nature 1994;367:576 ^ 9. 6. Maxwell M, Naber SP, Wolfe HJ, et al. Expression of angiogenic growth factor genes in primary human astrocytomas may contribute to their growth and progression. Cancer Res1991;51:1345 ^ 51. 7. Purow B, Fine HA. Antiangiogenic therapy for primary and metastatic brain tumors. Hematol Oncol Clin North Am 2004;18:1161 ^ 81, x. 8. D’Amato RJ, Loughnan MS, Flynn E, et al. Thalidomide is an inhibitor of angiogenesis. Proc Natl Acad Sci U S A 1994;91:4082 ^ 5. 9. Fine HA, Figg WD, Jaeckle K, et al. Phase II trial of the antiangiogenic agent thalidomide in patients with recurrent high-grade gliomas. J Clin Oncol 2000;18: 708 ^ 15. 10. Sampaio EP, Sarno EN, Galilly R, et al. Thalidomide selectively inhibits tumor necrosis factor a production by stimulated human monocytes. J Exp Med 1991; 173:699 ^ 703. 11. Dredge K, Horsfall R, Robinson SP, et al. Orally administered lenalidomide (CC-5013) is anti-angiogenic in vivo and inhibits endothelial cell migration and Akt phosphorylation in vitro. Microvasc Res 2005;69:56 ^ 63. 12. Haslett PA, Corral LG, Albert M, et al. Thalidomide costimulates primary humanT lymphocytes, preferentially inducing proliferation, cytokine production, and cytotoxic responses in the CD8+ subset. J Exp Med 1998;187:1885 ^ 92. 13. Bartlett JB, Michael A, Clarke IA, et al. Phase I study to determine the safety, tolerability and immunostimulatory activity of thalidomide analogue CC-5013 in patients with metastatic malignant melanoma and other advanced cancers. BrJCancer 2004;90:955 ^ 61. 14. Chanan-Khan A, Miller KC, Musial L, et al. Clinical efficacy of lenalidomide in patients with relapsed or refractory chronic lymphocytic leukemia: results of a phase II study. J Clin Oncol 2006;24:5343 ^ 9. 15. Choueiri TK, Dreicer R, Rini BI, et al. Phase II study of lenalidomide in patients with metastatic renal cell carcinoma. Cancer 2006;107:2609 ^ 16. 16. Richardson PG, Blood E, Mitsiades CS, et al. A randomized phase 2 study of lenalidomide therapy for patients with relapsed or relapsed and refractory multiple myeloma. Blood 2006;108:3458 ^ 64. 17. TohnyaTM, Ng SS, Dahut WL, et al. A phase I study of oral CC-5013 (lenalidomide, Revlimid), a thalidomide derivative, in patients with refractory metastatic cancer. Clin Prostate Cancer 2004;2:241 ^ 3. 18. List A, Dewald G, Bennett J, et al. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N Engl J Med 2006;355:1456 ^ 65. 19. TohnyaTM, Hwang K, Lepper ER, et al.Determination of CC-5013, an analogue of thalidomide, in human plasma by liquid chromatography-mass spectrometry. Clin Cancer Res 2007;13(23) December 1, 2007 7106 J Chromatogr B AnalytTechnol Biomed Life Sci 2004; 811:135 ^ 41. 20. Fine HA, Wen PY, Maher EA, et al. Phase II trial of thalidomide and carmustine for patients with recurrent high-grade gliomas. J Clin Oncol 2003;21: 2299 ^ 304. 21. Chang SM, Lamborn KR, Malec M, et al. Phase II study of temozolomide and thalidomide with radiation therapy for newly diagnosed glioblastoma multiforme. Int J Radiat Oncol Biol Phys 2004;60:353 ^ 7. 22. Groves MD, Puduvalli VK, Chang SM, et al. A North American brain tumor consortium (NABTC 99-04) phase II trial of temozolomide plus thalidomide for recurrent glioblastoma multiforme. J Neurooncol 2007; 81:271 ^ 7. 23. Bartlett JB, Dredge K, Dalgleish AG. The evolution of thalidomide and its IMiD derivatives as anticancer agents. Nat Rev Cancer 2004;4:314 ^ 22. 24. Dredge K, Marriott JB, Macdonald CD, et al. Novel thalidomide analogues display anti-angiogenic activity independently of immunomodulatory effects. Br J Cancer 2002;87:1166 ^ 72. 25. Gupta D,Treon SP, ShimaY, et al. Adherence of multiple myeloma cells to bone marrow stromal cells upregulates vascular endothelial growth factor secretion: therapeutic applications. Leukemia 2001;15:1950 ^ 61. 26. Walsh DC, Kakkar AK. Thromboembolism in brain tumors. Curr Opin Pulm Med 2001;7:326 ^ 31. 27.Wong ET, Hess KR, Gleason MJ, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II trials. J Clin Oncol 1999;17:2572 ^ 8. 28. Ballman KV, Buckner JC, Brown PD, et al. The relationship between six-month progression-free survival and 12-month overall survival end points for phase II trials in patients with glioblastoma multiforme. NeuroOncol 2007;9:29 ^ 38. www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on August 11, 2017. © 2007 American Association for Cancer Research. A Phase I Trial of Lenalidomide in Patients with Recurrent Primary Central Nervous System Tumors Howard A. Fine, Lyndon Kim, Paul S. Albert, et al. Clin Cancer Res 2007;13:7101-7106. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://clincancerres.aacrjournals.org/content/13/23/7101 This article cites 28 articles, 11 of which you can access for free at: http://clincancerres.aacrjournals.org/content/13/23/7101.full#ref-list-1 This article has been cited by 5 HighWire-hosted articles. Access the articles at: http://clincancerres.aacrjournals.org/content/13/23/7101.full#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on August 11, 2017. © 2007 American Association for Cancer Research.