Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
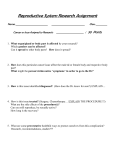
Title SYNCHRONOUS BILATERAL OVARIAN TORSION IN A NEONATE, LAPAROSCOPIC MANAGEMENT Authors Murat Alkan1, Ali Elbek2, Cuneyt Evruke3, Ahmet Eray Memec4, Bülent Aziz Özkan5, Hatice Gülin Sucak6, Ozgur Talat Erkan7 Affiliations Cukurova University Faculty of Medicine, Department of Pediatric Surgery and Division of Pediatric Urology1, Department of Obstetrics and Gynecology3, Adana, Turkey Medline Adana Hospital, Department of Pediatric Surgery2, Obstetrics and Gynecology4, Pediatrics5, Radiology6 and Anesthesiology7, Adana, Turkey Corresponding author Dr. Murat Alkan Cukurova University Faculty of Medicine Department of Pediatric Surgery, Division of Pediatric Urology, Balcalı, Adana Turkey Phone: 00905327402068 Fax: 00903223386428 1 Introduction Asynchronous bilateral ovarian torsion is stated as torsion of each ovary in different time periods. Synchronous bilateral ovarian torsion is an uncommon entity of which both ovaries twist at the same time or observed twisted during the surgical intervention. Both situations can be a destructive circumstance possibly leading to castration. Delay either in diagnosis or operation, ovarian torsion can result loss of ovarian tissue. We report a case of intrauterine bilateral ovarian torsion in a newborn, which successfully managed by laparoscopic approach. Case report A neonate born at term to a 26 year-old primigravida by elective cesarean delivery was diagnosed with an intra-abdominal cystic mass at 35th week of pregnancy. A conservative management plan was undertaken with repeated ultrasonographic evaluations every two weeks. The pregnancy, medical history of the patient and birth were unremarkable. A female full-term infant of 39+5 week of gestation was delivered with a birth weight of 4160 gram. Physical examination was unremarkable. Post-delivery ultrasonography revealed an anechoic uncomplicated cystic mass measuring 5x3.5 cm located in the right pelvis and another a semi-solid complicated cystic mass was located in the left pelvis with a measure of 5.4x3.8 cm, without any vascular signal. Both ovaries were not identified. Differential diagnoses were: omental cysts, mesenteric cysts, intestinal duplications and ovarian torsion. Bilateral unidentified ovaries with bilateral cystic masses in the pelvis called ‘bilateral ovarian torsion?’ into mind. We asked the parents to perform laparoscopy in order to preclude the possibility of bilateral torsion of the ovaries. We performed 2 laparoscopy after 16 hours of cesarean section. The initial laparoscopic finding revealed brown round smooth cystic mass with a tiny stalk nearly amputated from the left fallopian tube in the left pelvis. A loop of intestinal segment also twisted around this calcified tiny stalk of the mass (Figure 1). We then turned our attention to the right ovary. Right ovary was twisted with the cystic mass (Figure 2). The cyst nature was uncomplicated. The right ovary was untwisted 2 times (360 degree) and left in the pelvis after cyst aspiration without excision and ovarian fixation. Then the left ovary examined and seemed to be nearly amputated from the adnexa. The semisolid mass was aspirated, and muddy brownish fluid spreaded out to the peritoneal cavity. The tiny calcified stalk of the cyst leaded obstruction of a segment of small intestine. Calcified stalk separated and the adhesion with the segment of the intestinal loop released. The brownish ovary with cyst excised via aspiration. So, left oophorectomy was performed. The right ovary was re-examined. We decided not to perform oophoropexy or excise the cyst in order to salvage the rest of the ovarian tissue in the patient. The post-operative period was uneventful and the patient was discharged on the 2 nd post-operative day. Followup with ultrasonographic evaluations showed with a measure of 18 mm, 9 mm and no cyst in the right ovary in the first, second and third months, respectively. Discussion: The differential diagnosis of a cystic abdominal mass discovered by ultrasonography during pre-natal period derives from the omental cyst, mesenteric cyst, intestinal duplication, urachal cysts, renal cysts and ovarian cysts 1. Preoperative diagnosis of ovarian torsion is difficult not only in newborns or infants but also in pre pubertal ages of the children as well. The etiology of the ovarian cysts during pregnancy is related to the immature hypothalamus-pituitary-ovarian feedback that results gonadal hyperstimulation or 3 placental insufficiency with incomplete maturation of the gonadostat 2. In the early pubertal ages, functional ovarian cysts may be a predisposing cause of ovarian torsion 3. There are few reported patients of asynchronous bilateral adnexal torsion in children in the literature 4,5. These reports are all about the asynchronous ovarian torsions that internal between surgeries changes 6 week to 9 years time. Synchronous bilateral ovarian torsion has been reported with a case of a 26 year-old primigravida with a singleton pregnancy of 9 weeks gestation due to spontaneous ovarian hyperstimulation syndrome that was successfully managed by laparoscopic detorsion 6. When a post-natal radiological evaluation reveals a complicated ovarian cyst, irrespective of the size, surgical management recommended either by laparoscopy or laparotomy after delivery 7. Uncomplicated cysts, smaller than 5 cm diameter usually resolve spontaneously while the cysts exceeding 5 cm should be decompress via aspiration to prevent complications 8. When we searched the PubMed/Medline databases with the words ‘synchronous’, ‘bilateral ovarian torsion’, ‘newborn’ or ‘intrauterine’, the result is ‘no items found’. To the best of our knowledge, this is the first case of bilateral ovarian torsion diagnosed and managed laparoscopically in the neonatal period. This case highlights the importance of high index of suspicion and early diagnosis of bilateral ovarian torsion in the newborn that bilateral pelvic cysts detected in the pre-natal and post-natal period. References: 1. Mahomed A, Jibril A, Youngson G. Laparoscopic management of a large ovarian cyst in the neonate. Surg Endosc 1998 Oct; 12(10): 1272-1274. 2. Sedin G, Bergquist C, Lindgren PG. Ovarian hyperstimulation syndrome in preterm infants. 4 Pediatr Res 1985 Jun; 19(6): 548-552. 3. Davis AJ, Feins NR. Subsequent asynchronous torsion of normal adnexa in children. J Pediatr Surg 1990 Jun; 25(6): 687-689. 4. Ozcan C, Celik A, Ozok G, Erdener A, Balik E. Adnexal torsion in children may have a catastrophic sequel: asynchronous bilateral torsion. J Pediatr Surg 2002 Nov; 37(11): 1617-1620. 5. Dunnihoo DR, Wolff J. Bilateral torsion of the adnexa: a case report and a review of the world literature. Obstet Gynecol 1984 Sep; 64(3 Suppl): 55S-59S. 6. Munshi S, Patel A, Banker M, Patel P. Laparoscopic detorsion for bilateral ovarian torsion in a singleton pregnancy with spontaneous ovarian hyperstimulation syndrome. J Hum Reprod Sci 2014 Jan; 7(1): 66-68. 7. Templeman CL, Reynolds AM, Hertweck SP, Nagaraj HS. Laparoscopic management of neonatal ovarian cysts. J Am Assoc Gynecol Laparosc 2000 Aug; 7(3): 401-404. 8. Mittermayer C, Blaicher W, Grassauer D, Horcher E, Deutinger J, Bernaschek G, Ulm B. Fetal ovarian cysts: development and neonatal outcome. Ultraschall Med 2003 Feb; 24(1):21-26. 5 Figure Legends: 1. Figure 1: A loop of intestinal segment twisted around the calcified stalk of the left brownish ovary 2. Figure 2: Twisted right ovary 6