Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
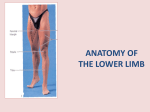
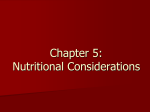
The Evaluation of The Athlete With Buttock Pain: An Approach To Diagnosis And Management AAPM&R Annual Assembly October 2nd, 2015 Matthew Smuck, MD Chief, Physical Medicine & Rehabilitation Associate Professor, Department of Orthopaedics Director, Wearable Health Lab Stanford University DISCLOSURES Cytonics - Research support ($ - paid to institution) Lumo BodyTech - Advisor (stock options) BlueJay Mobile Health - Advisor (stock options) Vivametrica - Founder (20% owner) State Farm Auto Insurance - Expert Witness ($ - hourly) SIS - Board of Directors ($ - travel/honoraria) The Spine Journal - Executive Editorial Board ($ - travel) Evaluation of The Athlete With Buttock Pain CASE 1 – “A CHALLENGE FOR THE 4 DIAGNOSTIC SENSES” 60 yo competitive cyclist with acute onset right buttock pain, followed by right leg symptoms. Day 1 Day 2-3 Day 4 Day 5 – acute pain onset while cycling uphill – leg pain and numbness improved with rest – buttock pain with thigh and calf cramping when walking – visit with PCP, lumbar MRI and PM&R consult Evaluation of The Athlete With Buttock Pain CASE 1 – “A CHALLENGE FOR THE 4 DIAGNOSTIC SENSES” 60 yo competitive cyclist with acute onset right buttock pain, followed by right leg symptoms. PM&R visit: – Look - MRI shows no herniaiton, no stenosis – Listen - Claudication with activity, not while standing – Feel - localized gluteal tenderness, no other provocation – Feel - normal neuro, diminished pedal pulses on the right Evaluation of The Athlete With Buttock Pain CASE 1 – “A CHALLENGE FOR THE 4 DIAGNOSTIC SENSES” 60 yo competitive cyclist with acute onset right buttock pain, followed by right leg symptoms. WHAT DO YOU DO NEXT? Evaluation of The Athlete With Buttock Pain CASE 1 – “A CHALLENGE FOR THE 4 DIAGNOSTIC SENSES” 60 yo competitive cyclist with acute onset right buttock pain, followed by right leg symptoms. Vascular Surgery visit: – ABI = 0.6/1.0 (right/left) – CT angiogram = dissection and partial occlusion of the common iliac artery SURGERY THE FOLLOWING DAY Evaluation of The Athlete With Buttock Pain VASCULAR BUTTOCK PAIN Aneurysms and pseudoaneurysms - Iliac arteries (common, internal, external) - Sciatic artery - Gluteal arteries (superior, inferior) Dissections and AV Fistulas - Iliac arteries Endofibrosis and kinking - Iliac arteries Evaluation of The Athlete With Buttock Pain VASCULAR BUTTOCK PAIN Evaluation of The Athlete With Buttock Pain VASCULAR BUTTOCK PAIN Evaluation of The Athlete With Buttock Pain CASE 1 – Look Feel “A CHALLENGE FOR THE 4 DIAGNOSTIC SENSES” Listen Evaluation of The Athlete With Buttock Pain CASE 1 – “A CHALLENGE FOR THE 4 DIAGNOSTIC SENSES” Look Listen Feel Smell Evaluation of The Athlete With Buttock Pain CASE 2 – “LET IT HEAL OR LET IT GO” 15 yo competitive baseball player with severe left upper gluteal pain when batting. July 13 Sept 13 Nov 13 Dec 13 Feb 14 – pain onset, continued play – MRI shows pars stress reaction, restricted play – pain free return to play – MVC with return of pain – first presents to our clinic with the following images Evaluation of The Athlete With Buttock Pain CASE 2 – “LET IT HEAL OR LET IT GO” 15 yo competitive baseball player with severe left upper gluteal pain when batting. Evaluation of The Athlete With Buttock Pain CASE 2 – “LET IT HEAL OR LET IT GO” 15 yo competitive baseball player with severe left upper gluteal pain when batting. WHAT DO YOU DO NEXT? Evaluation of The Athlete With Buttock Pain CASE 2 – “LET IT HEAL OR LET IT GO” 15 yo competitive baseball player with severe left upper gluteal pain when batting. Feb 14 – first presents to our clinic LET IT HEAL! April 14 – pain free with progressive training, but left-sided pain returned with recent attempt to resume batting The following images were obtained: Evaluation of The Athlete With Buttock Pain CASE 2 – “LET IT HEAL OR LET IT GO” 15 yo competitive baseball player with severe left upper gluteal pain when batting. LET IT GO! Thanks to D.J. Kennedy! Evaluation of The Athlete With Buttock Pain CASE 2 – “LET IT HEAL OR LET IT GO” DX: Pars Stress Fractures STANDARD EXAM Inspection, Palpation, ROM, Neurovascular, Special tests ONE LEGGED HYPEREXTENSION “No association between test and presence or absence of active spondylolysis” Masci 2006 Thanks to D.J. Kennedy! Evaluation of The Athlete With Buttock Pain CASE 2 – “LET IT HEAL OR LET IT GO” DX: Pars Stress Fractures MRI - BEST DEMONSTRATION OF OTHER PATHOLOGY - LACKS SENSITIVITY? Case reports of missed lesions Spect vs MRI › 40 pars fractures › MRI positive in 39/40 › Correctly graded only 29/40 › Several false positives Campbell 2006 Thanks to D.J. Kennedy! Imaging Algorithm History & Physical Plain Films • AP and Lateral (Spondylolisthesis) Treat presumptively Only Advance Imaging if: No response to treatment, red flags ,etc If no response • MRI (eval for bone edema) If still no response and negative MRI • Bone Scan Thanks to D.J. Kennedy! CT Correlating with boney union LIKELIHOOD TO HEAL L4 L5 - (22/35) = 63% Listhesis > 5˚ Listhesis < 5˚ - (3/65) - (18/204) = 8.8% Fujii 2004 = 4.6% - (37/174) = 21% Thanks to D.J. Kennedy! Why CT scan? VERY GOOD BONY ANATOMY Sensitivity less than bone scan Early CORRELATION WITH BONY UNION 134 pts with 239 pars - Early (31/50) = 62% - Progressive (9/103) = 8.7% - Terminal (0/86) = 0% Terminal Fujii 2004 Thank You! Matthew Smuck, MD Chief, Physical Medicine & Rehabilitation Associate Professor, Orthopaedic Surgery Director, Wearable Health Lab Stanford University [email protected]