Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
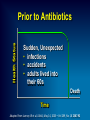
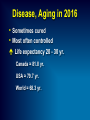
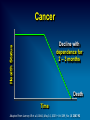
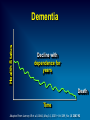
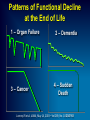
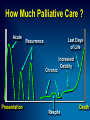
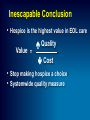
Palliative Care Interdisciplinary Curriculum A Joint Initiative of the Palliative Medicine Faculty & Staff of We gratefully acknowledge the support of Award Number R25CA134309 from the National Cancer Institute The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health Palliative Care is… Hospice Care is… Frank D Ferris, MD, FAAHPM, FAACE Palliative Care Interdisciplinary Curriculum Objectives • Modern illness experience • What are palliative & hospice care • Value of early referral Main Message Early referral to palliative & hospice care, delivers higher value & safety… Success of Modern Medicine… Illness in the Past . . . Health Status Prior to Antibiotics Sudden, Unexpected • infections • accidents • adults lived into their 60s Death Time Adapted from Lunney JR et al. JAMA, May 14, 2003—Vol 289, No. 18 2387-92 Health Status 1940s - 1980s Prolonged Dying • predictable decline Decline Death Time Adapted from Lunney JR et al. JAMA, May 14, 2003—Vol 289, No. 18 2387-92 Illness in 2016 . . . Disease, Aging in 2016 • Sometimes cured • Most often controlled Life expectancy 20 - 30 yr. Canada ≈ 81.8 yr. USA ≈ 79.7 yr. World ≈ 68.3 yr. Cancer Health Status Decline with dependence for 2 – 3 months Death Time Adapted from Lunney JR et al. JAMA, May 14, 2003—Vol 289, No. 18 2387-92 Kit, 58 year old Peripheral lung mass on routine chest x-ray • Wants best treatment for her cancer • Wants to be comfortable, with family Kit: Surgery • Subtotal pneumonectomy • Adenocarcinoma • Metastatic workup: No evidence other cancer • Post-thoracotomy pain syndrome Opioids + adjuvants to control pain What does Kit need ? Multiple Issues Cause Suffering Disease Management •Diagnosis •Prognostication •Management Physical •Pain, dyspnea & other symptoms •Function, fluids, nutrition Loss, grief •Emotional responses •Bereavement End of life / death management •Last hours of living •When death occurs Psychological •Anxiety •Depression •Distress Social •Family dynamics •Financial •Legal Practical •Caregiving •Teamwork •Volunteers Spiritual •Hope •Meaning, value •Existential Who is Affected Martha, 76, Pulmonary Fibrosis … Dr. Charles von Gunten, OhioHealth What does Martha need ? What are the Clinicians thinking ? Debrief… Martha… Dr. Charles von Gunten, OhioHealth What does Martha need ? What are the Clinicians thinking ? Organ Failure Health Status e.g., CHF, COPD, Renal, Liver Decline with dependence for months – years Crisis Death Time Adapted from Lunney JR et al. JAMA, May 14, 2003—Vol 289, No. 18 2387-92 Health Status Dementia Decline with dependence for years Death Time Adapted from Lunney JR et al. JAMA, May 14, 2003—Vol 289, No. 18 2387-92 Why Did Kit and Martha come to the Healthcare system ? Normal path of life with an anticipated future Illness path with an uncertain future Help me fix my broken story ( Brody ) Patients & Families Want… • Live life the way they want to ‘ Fix ’ disease, or not Prevent and relieve suffering, or not Don’t do treatments they don’t want • Negotiate goals for 1. Life 2. Medical care Death in North America • 90% want to die at home ( NHO Gallup survey ) • 25 % die at home • 75 % die in institutions ( Teno et al, 1997 ) 2 / 3 in hospitals 1 / 3 in nursing homes • 90% believe it is a family responsibility to provide care to a loved one What do You want your illness experience to be ? Patterns of Functional Decline at the End of Life 1 – Organ Failure 3 – Cancer 2 – Dementia 4 – Sudden Death Lunney JR et al. JAMA, May 14, 2003—Vol 289, No. 18 2387-92 Where Would You Like to Receive Your Care When You are Dependent ? 1. Acute care 2. Long-term care 3. Home Palliative Care is… Palliative Care is… • Prevent & relieve suffering • Promote quality of life and death • Any diagnosis • Any time there is need Adapted From: Ferris FD, Balfour HM, Bowen K, Farley J, Hardwick M, Lamontagne C, Lundy M, Syme A, West P. A Model to Guide Hospice Palliative Care. Ottawa, ON: Canadian Hospice Palliative Care Association, 2002. Historical Perspective Anti-disease Therapy Presentation End-of-Life Care 6m Death Bereavement Care Palliative Care 2016 2026 End-of-Life Care Anti-disease Therapy Palliative Care Presentation Therapies to 6m Death relieve suffering and / or Bereavement Care improve quality of life Domains of Care Disease management Physical Loss, grief End of life / death management Psychological Social Practical Spiritual Interdisciplinary Care Spiritual counselor Volunteers Nurse Family Doctor Patient Social worker Community Physio therapist Psychologist Pharmacist Bereavement counselor ICUs Acute Care Office Home Inpatient Unit Other, eg, Jails Long-Term Care Inpatient Unit Specialized Units D A Y H O S P I T A L Fact Our ability to relieve the pain, symptoms and the distress of serious illness has never been greater Goals of Palliative Care Help to • Eat well • Sleep well • Maintain function • Reduce stress Live better Live longer “ Add life to days and days to life ” Hospice Care is… Hospice Care is… Anti-disease Therapy End-of-Life / Hospice Care = Enhanced Palliative Care Hospice Care Presentation Therapies to 6m Death relieve suffering and / or Bereavement Care improve quality of life In the USA Since 1982, Hospice Care is • Medicare insurance benefit • Carved out of Medicare Part A • Adopted by Medicaid Commercial insurers Eligibility • 2 physicians certify Referring physician Hospice medical director “ I believe the patient has a prognosis of ≤ 6 months if the illness runs its normal course ” ‘ More likely than not ’ = 51 % probabililty Benefit Periods Initial Certification 2 physicians Referring Hospice Medical Director 90 d 90 d F 2 F 60 d F 2 F 60 d F 2 F 60 d Recertification 1 physician Hospice Medical Director F 2 Unlimited F 60 d Medicare Hospice Benefit includes… • Patients & their families • Treat & prevent issues that cause suffering • Promote quality of life during illness & bereavement Facilitate transitions Achieve full potential – finish life story Rebuild lives Medicare Hospice Benefit includes… • Services Skilled nursing Medical counseling Chaplaincy • Medications / therapies • Medical equipment • Supplies Healthcare Aides Volunteers 24 hr Triage Bereavement support ≥ 13 months • Palliative Medicine physicians …Medicare Hospice Benefit in Central Ohio • Routine care ~ $150 / day • Respite care ( 5 days ) ~ $150 / day • Continuous care ( crises ) ~ $800 / day Home Extended care facility • General Inpatient Care ( GIP ) ~ $800 / day Hospice Hospital Value of early Palliative Care… Quality Value = Cost Safety = minimize risk of harm & don’t Rx without benefit Key Elements of Palliative Care • Communication & negotiation of goals of life & care • Symptom management • Distress How Much Palliative Care ? Acute Last Days of Life Recurrence Chronic Presentation Increased Debility Respite Death Impact of COPD Pilot Program Hospitalizations per 1000 patient exposure days 39 % Reduction in Re-hospitalizations COPD Pilot Program Hospitalization Density Pre Index Discharge vs. Post Index Discharge 10.00 9.48 9.00 8.00 7.00 6.00 6.69 6.77 7.24 6.57 5.76 5.00 4.00 3.00 2.00 1.00 0.00 Enrolled 50 patients (p=.03) Not enrolled 202 patients (p=.91) Pre Post All Patients (p=.31) 2010 Benefits of Early Palliative Care Survival • Longer • Better • Understanding prognosis • Goals of care Less IV chemo in last 60 days Quality of Life • Improved mood American Society of Clinical Oncology recommends… Concurrent palliative care for seriously ill cancer patients – from the beginning 2012 Palliative Care at Kaiser, Los Angeles • 484 Seriously ill, inpatient palliative care consult • 10 % readmitted within 30 days Enguidanos et al, J Palliat Medicine 2012; 15(12): 1356 Value of early Hospice Care… ‘ Excellent ’ Quality of EOL Care 80 n = 1578 percent 70 60 50 40 Excellent 30 20 10 0 Home Care Hospice NH Hospital Teno et al JAMA 2004; 291: 88-93 Outcomes in Last Place of Care percent n = 1578 Teno et al JAMA 2004; 291: 88-93 Cost with Hospice Care • Significant savings when compared with no hospice care Kelley AS et al, Health Affairs 2013; 552: 561 Inescapable Conclusion • Hospice is the highest value in EOL care Value = Quality Cost • Stop making hospice a choice • Systemwide quality measure How do we get everyone to incorporate palliative care into practice early ? Fully Integrate Palliative Care Ambulatory Outpatient Clinics Hospital Consultation Services Specialty Inpatient Long-term Care Units Home Care Value for Martha Hospice Care for 2 years… Value for Kit… Kit: 6 Months • Recurrence in axillary lymph nodes • Chemo: partial response • XRT: partial response • Chemo: stable disease • Resection ? • Progression Kit: 21 months • Hospice care 3 months • Oncologist attending • Resolution • Gifts • Surprises Main Message Early referral to palliative & hospice care, delivers higher value & safety… What Experience . . . your patients & families, your loved ones, and ultimately yourselves? “ The standards of practice we create And the people we train Will look after us When it’s our turn to receive care… Will Ohio be ready for you ? ” Gandhi… You need to be the change you want to see in the world… Kobacker House Columbus, Ohio Palliative Care Interdisciplinary Curriculum A Joint Initiative of the Palliative Medicine Faculty & Staff of We gratefully acknowledge the support of Award Number R25CA134309 from the National Cancer Institute The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Cancer Institute or the National Institutes of Health