Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
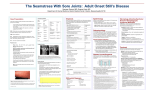
ARTHRITIS & RHEUMATOLOGY Vol. 66, No. 6, June 2014, pp 1659–1665 DOI 10.1002/art.38398 © 2014, American College of Rheumatology Efficacy of Tocilizumab in Conventional Treatment–Refractory Adult-Onset Still’s Disease Multicenter Retrospective Open-Label Study of Thirty-Four Patients Francisco Ortiz-Sanjuán,1 Ricardo Blanco,1 Vanesa Calvo-Rio,1 Javier Narvaez,2 Esteban Rubio Romero,3 Alejandro Olivé,4 Santos Castañeda,5 Adela Gallego Flores,6 M. Victoria Hernández,7 Cristina Mata,1 Inmaculada Ros Vilamajo,8 Walter Alberto Sifuentes Giraldo,9 Miguel A. Caracuel,10 Mercedes Freire,11 Catalina Gómez Arango,12 José Llobet,13 Sara Manrique Arija,14 Carlos Marras,15 Concepción Moll-Tuduri,16 Chamaida Plasencia-Rodriguez,17 Rosa Roselló,18 Ana Urruticoechea,19 Maria L. Velloso-Feijoo,20 Jordi del Blanco,21 M. Carmen González-Vela,1 Javier Rueda-Gotor,1 Trinitario Pina,1 Javier Loricera,1 and Miguel A. González-Gay1 Objective. Adult-onset Still’s disease (AOSD) is frequently refractory to standard therapy. Tocilizumab (TCZ) has demonstrated efficacy in single cases and in small series of patients with AOSD. The aim of this multicenter study was to assess the efficacy of TCZ in patients with AOSD refractory to conventional treatment. Methods. This was a retrospective open-label study of TCZ treatment in 34 patients with AOSD who had experienced an inadequate response to corticosteroids and at least 1 standard synthetic immunosuppressive drug and also, in many cases, biologic agents. Results. The mean ! SD age of the patients (8 men and 26 women) was 38.7 ! 16.1 years. The median duration of AOSD before TCZ was initiated was 4.2 years (interquartile range [IQR] 1–9 years). The initial dosages of intravenous TCZ were 8 mg/kg every 4 weeks in 22 patients, 4 mg/kg every 4 weeks in 2 patients, and 8 mg/kg every 2 weeks in 10 patients. TCZ treatment Supported in part by the Instituto de Salud Carlos III, Spain (RETICS Programs; RD08/0075 [RIER] and RD12/0009/0013). Presented in part at the 77th Annual Scientific Meeting of the American College of Rheumatology, San Diego, CA, October 2013. 1 Francisco Ortiz-Sanjuán, MD, Ricardo Blanco, MD, PhD, Vanesa Calvo-Rio, MD, Cristina Mata, MD, M. Carmen GonzálezVela, MD, Javier Rueda-Gotor, MD, Trinitario Pina, MD, Javier Loricera, MD, Miguel A. González-Gay, MD, PhD: Hospital Universitario Marqués de Valdecilla and Instituto de Investigación Marqués de Valdecilla (IDIVAL), Santander, Spain; 2Javier Narváez, MD, PhD: Hospital Universitario de Bellvitge, Hospitalet, Barcelona, Spain; 3Esteban Rubio Romero, MD: Hospital Universitario Virgen del Rocı́o, Seville, Spain; 4Alejandro Olivé, MD, PhD: Hospital Universitario Germans Trias i Pujol, Badalona, Spain; 5Santos Castañeda, MD, PhD: Hospital Universitario de La Princesa, IIS Princesa Madrid, Madrid, Spain; 6Adela Gallego Flores, MD: Hospital de Mérida, Mérida, Spain; 7M. Victoria Hernández, MD, PhD: Hospital Clinic of Barcelona, Barcelona, Spain; 8Inmaculada Ros Vilamajo, MD: Hospital Son Llàtzer, Palma de Mallorca, Spain; 9 Walter Alberto Sifuentes Giraldo, MD: Hospital Ramón y Cajal, Madrid, Spain; 10Miguel A. Caracuel, MD: Hospital Reina Sofı́a, Córdoba, Spain; 11Mercedes Freire, MD: Hospital Universitario Juan Canalejo, La Coruña, Spain; 12Catalina Gómez-Arango, MD: Hospital Universitario Basurto, Bilbao, Spain; 13José Llobet, MD: Hospital Sant Pau, Barcelona, Spain; 14Sara Manrique-Arija, MD: Urgencias Hospital Regional Universitario Carlos Haya, Málaga, Spain; 15Carlos Marras, MD: Hospital Universitario Virgen de la Arrixaca, Murcia, Spain; 16Concepción Moll-Tuduri, MD: Hospital Mateu Orfila, Mahón, Spain; 17Chamaida Plasencia-Rodriguez, MD: Hospital Universitario La Paz, Madrid, Spain; 18Rosa Roselló, MD: Hospital San Jorge, Huesca, Spain; 19Ana Urruticoechea, MD: Hospital Can Misses, Ibiza, Spain; 20Maria Luisa Velloso Feijoo, MD: Hospital Valme, Seville, Spain; 21Jordi del Blanco, MD: Hospital Sant Jaume, Calella, Spain. Drs. Ortiz-Sanjuán, R. Blanco, and Calvo-Rio contributed equally to this work. Address correspondence to Miguel A. González-Gay, MD, PhD, or Ricardo Blanco, MD, PhD, Rheumatology Division, Hospital Universitario Marqués de Valdecilla, IDIVAL, Avenida Valdecilla s/n, 39008 Santander, Spain. E-mail: [email protected] or [email protected]. Submitted for publication November 8, 2013; accepted in revised form February 4, 2014. 1659 1660 resulted in rapid and maintained improvement in both clinical and laboratory parameters. After 1 year of TCZ therapy, the incidence of joint manifestations had decreased from 97.1% at baseline to 32.4%, the incidence of both cutaneous manifestations and fever had decreased from 58.8% to 5.9%, and the incidence of lymphadenopathy had decreased from 29.4% to 0%. A dramatic reduction in laboratory markers of inflammation, including the C-reactive protein level, the erythrocyte sedimentation rate, and the ferritin level, was achieved. The median dosage of prednisone was also reduced, from 13.8 mg/day (IQR 5–45) at the initiation of TCZ to 2.5 mg/day (IQR 0–30) at 12 months. After a median followup of 19 months (IQR 12–31 months), only 2 patients required permanent discontinuation of TCZ therapy because of severe infections. Conclusion. TCZ treatment was associated with rapid and maintained clinical and laboratory improvement in patients with AOSD refractory to standard treatment. However, joint manifestations seem to be more refractory to treatment compared with systemic manifestations. Adult-onset Still’s disease (AOSD) is a systemic inflammatory disease of unknown etiology characterized by high fever spikes, arthritis and/or arthralgia, and evanescent maculopapular salmon-pink rash that appears predominantly on the trunk and proximal limbs. Other features are sore throat or pharyngitis, myalgia, lymphadenopathy, hepatosplenomegaly, and serositis. Laboratory tests show increased concentrations of acute-phase reactants, leukocytosis with neutrophil predominance, elevated levels of liver enzymes, and high serum levels of ferritin (1,2). The pathogenesis of AOSD remains unknown. Several studies have suggested a genetic predisposition, while others have identified different infectious agents as potential triggers of the disease. A number of studies have demonstrated abnormal production of proinflammatory cytokines, such as interleukin-1 (IL-1), IL-6, IL-18, tumor necrosis factor ! (TNF!), or interferon-", by T lymphocytes and macrophages (3,4). These findings may explain the intermittent course of AOSD and the clinical and laboratory features that resemble those of genetic autoinflammatory syndromes. Increased levels of IL-6 and/or IL-18 have been associated with clinical and laboratory features such as fever, rash, elevated liver enzyme levels, hyperferritinemia, and increased C-reactive protein (CRP) levels (5). First-line treatment in AOSD includes the use of nonsteroidal antiinflammatory drugs, although only ORTIZ-SANJUÁN ET AL 15–20% of patients respond to this treatment; in most cases, treatment with corticosteroids is required. Other therapies, such as methotrexate, azathioprine, leflunomide, intravenous immunoglobulin, anakinra, antiTNF! drugs, rituximab, and abatacept, are often needed to achieve adequate control of the disease and reduce the dose of corticosteroids. However, the efficacy of these drugs in the control of disease activity is variable, and in some cases, they are associated with potential severe side effects. Tocilizumab (TCZ) is a humanized monoclonal antibody against the IL-6 receptor; it is approved for the treatment of rheumatoid arthritis (RA) (6) and systemic juvenile idiopathic arthritis (JIA) (7). Because IL-6 has been implicated in the pathogenesis of AOSD (3), several studies have assessed the potential effect of TCZ in patients with AOSD refractory to multiple therapies (8–10). However, in most cases, information related to this issue is based on small series or case reports. Therefore, the aim of the current study was to evaluate the efficacy of TCZ in a large series of patients with AOSD refractory to other treatments. PATIENTS AND METHODS Patients and study protocol. We conducted a retrospective, open-label, multicenter study that included 34 patients with AOSD. All patients had previously received standard synthetic immunosuppressive drugs and in some cases other biologic agents. TCZ treatment was prescribed due to lack of efficacy and/or adverse events associated with previous treatments. AOSD was diagnosed at the rheumatology units of 21 Spanish referral centers according to the criteria described by Yamaguchi et al (11). Other diseases were excluded. Before the initiation of TCZ treatment, the presence of infections, including hepatitis B or hepatitis C virus infections, was excluded using clinical examination and serologic tests. In all patients, latent tuberculosis was also ruled out by tuberculin (purified protein derivative) skin testing and/or QuantiFeron assay and chest radiography. Because AOSD is an off-label indication for TCZ, a written informed consent form approved for each hospital was requested and obtained from each patient prior to the onset of TCZ treatment. Data registered by each investigator were reviewed according to a protocol agreed upon beforehand that included the collection of relevant information on the patients. Clinical definitions. The medical records were reviewed according to a previously established protocol. According to that protocol, fever was defined as a body temperature of #38°C in the previous week of the assessment period. Joint symptoms included arthralgia and/or arthritis. Cutaneous rash was considered to be present if patients had a salmon-pink macular or maculopapular eruption predominantly on the trunk and extremities. Hepatomegaly and splenomegaly were confirmed by ultrasonography or computed tomography. Lymphadenopathy was defined as the presence of enlarged TOCILIZUMAB IN AOSD REFRACTORY TO STANDARD TREATMENT lymph nodes at #2 different sites. A diagnosis of pericarditis was made if the patient presented with chest pain and had pericardial rub or an effusion documented by echocardiography. Pleuritis was identified by the presence of pleuritic pain and pleural effusion. Clinical manifestations were considered to be improved if resolution of these manifestations occurred during the extended followup period. Laboratory data. According to the study protocol, information on routine laboratory markers of disease activity, including complete blood cell count, erythrocyte sedimentation rate (ESR), CRP level, serum levels of ferritin and creatinine, liver enzymes, proteinuria, and hematuria, was collected. Anemia was defined as a hemoglobin level of $11 gm/dl. Leukocytosis was defined as a white blood cell count of #11,000/mm3. The ESR was considered to be increased when it was !20 mm/hour in men or !25 mm/hour in women. An elevated CRP level was defined as !0.5 mg/dl, and a high serum level of ferritin was defined as #200 ng/ml. The effect of TCZ on variables other than clinical manifestations, such as the leukocyte count and hemoglobin level, the ESR, CRP and ferritin levels, and the daily prednisone dose, was also assessed. Values for these variables at baseline were compared with those at 1 month, 3 months, 6 months, and 12 months. In addition, clinical and laboratory data from the last visit were assessed. Data collection. Data were first reviewed and then analyzed in an attempt to assess the following: clinical and laboratory data, therapies used in the management of AOSD (including those given to patients before the onset of TCZ treatment), response to previous biologic therapy, and adverse events. This information was extracted from the patients’ clinical records, reviewed for confirmation of the diagnosis, and stored in a computerized file according to a protocol established beforehand and agreed upon by researchers. To minimize entry error, all of the data were double-checked. Statistical analysis. Statistical analysis was performed using StatSoft Statistica software. Results are expressed as the mean " SD for variables with a normal distribution or as the median (range) or interquartile range (IQR) for variables with a non-normal distribution. Continuous variables were compared using Wilcoxon’s signed rank test. RESULTS Thirty-four patients (26 women and 8 men) with AOSD who received TCZ therapy were studied. The mean age of the patients at the onset of TCZ treatment was 38.7 " 16.1 years (range 16–74 years), and the median duration of AOSD before the initiation of TCZ treatment was 4.2 years (IQR 1–9 years). Prior to receiving TCZ, in addition to receiving corticosteroids, all of the patients had been treated with traditional synthetic immunosuppressive drugs, and 17 (50%) of them had received other biologic therapies (Table 1). TCZ was prescribed as monotherapy (15 cases) or in combination with other traditional synthetic immunosuppressive drugs (19 cases), usually methotrex- 1661 Table 1. Main features of the 34 patients with conventional treatment–refractory adult-onset Still’s disease treated with tocilizumab (TCZ)* Age, mean " SD (range) years No. men/no. women Disease duration before TCZ, median (IQR) years Immunosuppressive treatment before TCZ Nonbiologic Methotrexate Leflunomide Cyclosporin A Sulfasalazine Cyclophosphamide Mycophenolate mophetil Biologic Anakinra Etanercept Adalimumab Rituximab Infliximab Abatacept Concomitant treatment with TCZ at baseline Corticosteroids Methotrexate Hydroxychloroquine TCZ dosage Baseline 8 mg/kg every 4 weeks 6 mg/kg every 4 weeks 4 mg/kg every 4 weeks 8 mg/kg every 2 weeks After 1 year 8 mg/kg every 4 weeks 6 mg/kg every 4 weeks 4 mg/kg every 4 weeks 8 mg/kg every 2 weeks 38.7 " 16.1 (16–74) 8/26 4.2 (1–9) 31 (91.2) 5 (14.7) 2 (5.9) 2 (5.9) 1 (2.9) 1 (2.9) 14 (41.2) 7 (20.6) 7 (20.6) 6 (17.6) 4 (11.8) 2 (5.9) 22 (64.7) 18 (52.9) 1 (2.9) 22 (64.7) 0 (0) 2 (5.9) 10 (29.4) 17 (50.0) 4 (11.8) 3 (8.8) 10 (29.4) * Except where indicated otherwise, values are the number (%). IQR # interquartile range. ate (Table 1). The initial intravenous TCZ dosage was 8 mg/kg every 4 weeks (22 cases), 8 mg/kg every 2 weeks (10 cases), and 4 mg/kg every 4 weeks (2 cases). The maintenance dosage of TCZ was 4–8 mg/kg every 2 weeks or every 4 weeks (Table 1). At the onset of TCZ treatment, the most frequent clinical features were joint manifestations (33 cases), fever (20 cases), cutaneous rash (18 cases), lymphadenopathy (10 cases), splenomegaly (2 cases), hepatomegaly (3 cases), pleuritis (1 case), and pericarditis (2 cases). Most patients had abnormal laboratory values at baseline, including anemia (15 cases), leukocytosis (19 cases), a high CRP level (28 cases), and an increased ESR (27 cases) (Table 2). Nevertheless, most patients experienced improvement in both clinical manifestations and laboratory abnormalities following TCZ therapy; such improvement was already clinically evident 1662 ORTIZ-SANJUÁN ET AL Table 2. Clinical manifestations and laboratory parameters at baseline and following tocilizumab therapy in the patients with adult-onset Still’s disease refractory to previous immunosuppressive drugs* Clinical manifestations Joint manifestations Fever Cutaneous manifestations Lymphadenopathy Splenomegaly and/or hepatomegaly Pleuritis and/or pericarditis Laboratory parameters Hemoglobin, mean " SD gm/dl Anemia Leukocyte count, mean " SD mm3 Leukocytosis CRP, median (IQR) mg/dl High CRP level ESR, median (IQR) mm/hour High ESR Ferritin, median (IQR) ng/ml High serum ferritin level Baseline (n # 34) Month 1 (n # 34) Month 3 (n # 34) Month 6 (n # 34) Month 12 (n # 32) 97.1 58.8 58.8 29.4 11.8 8.8 67.6 5.9 5.9 11.8 6.25 0 44.1 5.9 5.9 0 0 0 26.5 5.9 5.9 0 0 0 32.4 5.9 5.9 0 0 0 11.9 " 1.4 44.1 13,534.2 " 6,022.8 55.9 8.9 (3.9–23.2) 82.4 52 (45–69) 79.4 480 (200–808) 47.1 12.9 " 1.2 14.7 8,983.1 " 4,549.6 26.5 0.2 (0.1–1.6) 29.4 4 (2–12) 8.8 239 (39–358) 17.7 13.3 " 1.1 11.8 8,044.2 " 4,359.9 17.6 0.1 (0.01–0.7) 8.8 4 (2–9) 0 100 (73–132) 2.9 13.3 " 1.3 8.9 7,579.2 " 3,587.8 11.8 0.2 (0.01–0.9) 20.6 4 (2–8) 2.9 107 (53–187) 5.9 14 " 1.3 2.9 8,682.9 " 3,658.2 17.6 0.2 (0.03–1.1) 23.5 2 (2–12) 2.9 90 (63–115) 2.9 * Except where indicated otherwise, values are the percent of patients. CRP # C-reactive protein; IQR # interquartile range; ESR # erythrocyte sedimentation rate. at month 1. This good response to TCZ was maintained over time (Table 2 and Figure 1). After 1 year of TCZ therapy, the incidence of joint manifestations had decreased from 97.1% at base- Figure 1. Rapid improvement following the initiation of tocilizumab therapy and maintenance of improvement over 12 months. A, Leukocyte counts (black line) and hemoglobin levels (shaded line). B, C-reactive protein (CRP) levels (black line) and erythrocyte sedimentation rates (ESRs) (shaded line). C, Ferritin levels. D, Corticosteroid-sparing effects. Values in A are the mean " SD; values in B–D are the median (interquartile range). ! # P $ 0.05 versus basal. TOCILIZUMAB IN AOSD REFRACTORY TO STANDARD TREATMENT line to 32.4%, the incidence of both cutaneous manifestations and fever had decreased from 58.8% to 5.9%, and the incidence of lymphadenopathy had decreased from 29.4% to 0%. The frequency of abnormally elevated CRP levels and ESRs decreased from 82.4% to 23.5% and from 79.4% to 2.9%, respectively. The incidence of leukocytosis also decreased, from 55.9% at baseline to 17.6% at 1 year, the incidence of anemia decreased from 44.1% to 2.9%, and the incidence of high serum levels of ferritin decreased from 47.1% to 2.9% (Table 2). Interestingly, after 1 year of TCZ therapy, the median dosage of prednisone had decreased from 13.8 mg/day (IQR 5–45) at the onset of TCZ treatment to 2.5 mg/day (IQR 0–30). There was also a significant corticosteroid-sparing effect when the basal dose of prednisone was compared with the doses administered at 1 month (P # 0.01), 3 months (P $ 0.01), 6 months (P $ 0.01), and 12 months (P # 0.01), respectively (Figure 1). After a median followup of 19 months (IQR 12–31 months), infections were the most common complications related to TCZ therapy. Nevertheless, TCZ had to be permanently discontinued in only 2 patients, both of whom had severe infections. One of these patients had pyelonephritis and acute enterocolitis, and the other had bacterial spondylodiscitis with an abscess in the psoas muscle caused by Staphylococcus aureus. Nevertheless, full recovery following antibiotic treatment was achieved in both patients. Other infections attributed to TCZ were pneumonia (1 case), upper respiratory tract infection (3 cases), dental infection (1 case), urinary infection (1 case), Epstein-Barr virus infection (1 case), and herpes zoster virus infection (1 case). Other minor side effects were mild leukopenia or neutropenia (4 cases), elevated hepatic enzyme levels during TCZ treatment (4 cases), hypercholesterolemia that required statin therapy in 1 patient who had normal cholesterol levels before the initiation of TCZ treatment, and headache associated with TCZ infusion in another patient. DISCUSSION In this multicenter observational study, we observed that TCZ treatment resulted in rapid clinical and laboratory improvement that was maintained over time, even in patients with AOSD refractory to treatment with other biologic agents. First-line therapy in AOSD is based on corticosteroids, which often requires high doses for a long period of time, with the subsequent risk of side effects. In an attempt to provide a corticosteroidsparing effect, different medications such as metho- 1663 trexate, azathioprine, intravenous immunoglobulin, anakinra, and anti-TNF! agents have been used in patients with AOSD. All of them have shown variable results without being exempt from side effects. The rationale for the use of the anti–IL-6 receptor antibody TCZ in AOSD is based on our understanding of the role of IL-6 in this disease and experience with TCZ in the treatment of RA (6,12). IL-6 is a pleiotropic cytokine involved in production of immunoglobulins, B cell differentiation, T cell growth and cytotoxic T cell differentiation, macrophage differentiation, modulation of hematopoiesis, and stimulation of hepatocytes to produce acute-phase proteins such as CRP. Overproduction of IL-6 can explain major symptoms of AOSD, inducing fever, leukocytosis, thrombocytosis, acutephase reactant production, and bone resorption. Furthermore, high levels of IL-6 have been observed in the blood of patients with AOSD and have been shown to correlate with disease activity (3). TCZ is a humanized monoclonal antibody that binds to the cell receptor for IL-6 and has demonstrated efficacy in patients with RA (13). Additionally, randomized placebo-controlled trials also demonstrated the efficacy of TCZ in systemic JIA, an entity that shows some similarities with AOSD (7). TCZ has been used in cases of treatmentrefractory AOSD, with promising results; however, the number of cases reported is still small (8–10). To the best of our knowledge, 2 small series of patients with conventional treatment–refractory AOSD who received therapy with TCZ have been reported. One of these studies assessed 14 patients (8), and the other assessed 11 patients (14). In both series, the patients were followed up for 6 months. In the current report, we present data on 34 patients with AOSD who were followed up for a median of 19 months. In keeping with previous series (8,14), a high number of our patients had received other synthetic immunosuppressive agents (Table 1). Moreover, in many of these patients, AOSD had also been refractory to treatment with biologic agents such as anakinra or anti-TNF! (Table 1). As in our series, the patients described by Puechal et al (8) and Elkayam et al (14) received variable dosages of TCZ (4–8 mg/kg every 2, 4, or 8 weeks). In this regard, although the dosage of TCZ in RA or systemic JIA is well established (6,7), there is no consensus on the dosage of TCZ that should be given to patients with AOSD. We believe that patients with AOSD in whom disease is very active, as manifested by a high inflammatory burden, may need a higher dosage of TCZ. In our series, two-thirds of the patients (n # 22) received an 1664 initial TCZ dosage of 8 mg/kg every 4 weeks, but 10 patients received an initial dosage of 8 mg/kg every 2 weeks. This higher dosage (8 mg/kg every 2 weeks) is used in systemic JIA. Thus, even in children with JIA who weigh $30 kg, the recommended dosage is 12 mg/kg every 2 weeks (7). During the followup period in our series, some patients required an increase in the dosage, while the dosage was reduced in others depending on efficacy and side effects (Table 1). Regardless of whether TCZ was combined with methotrexate, we observed a nonsignificant trend toward greater improvement in patients who received a higher or more frequent dose of TCZ compared with the remaining patients. However, the difference was not statistically significant (data not shown). In most cases, improvement in clinical and laboratory parameters was observed at the time of the first available analysis of data (1 month after the onset of TCZ therapy). Of note, improvement was also observed at 3, 6, and 12 months. The significant reductions in the CRP level and the ESR following the initiation of TCZ treatment were especially remarkable. This finding was consistent with previous reports that also described a reduction of these acute-phase reactants after 3 months or 6 months of TCZ treatment (8,14). Rapid improvement in systemic symptoms such as fever and cutaneous manifestations was also observed in our series. This was also described in a review article by de Boysson et al (15), which showed clinical and laboratory improvement in 27 of 28 patients (96%). However, it is well known that joint manifestations in patients with AOSD may be more refractory to treatment compared with systemic manifestations. This was also the case in our series, because 32.4% of patients had persistent joint involvement after 1 year of TCZ therapy. In accordance with our results, Puechal et al (8) reported improvement in joint manifestations (European League Against Rheumatism Response Criteria [Disease Activity Score in 28 joints of $2.6]) (16) in only 36% and 57% of patients after 3 months and 6 months of TCZ therapy, respectively. In our series, TCZ also had a significant corticosteroid-sparing effect. The prednisone dosage was reduced significantly during TCZ therapy (Figure 1). This is especially important in patients with chronic AOSD and those whose disease is refractory to conventional drugs, because these patients receive an inappropriately high cumulative dose of corticosteroids, leading to a high risk of side effects. TCZ was relatively safe in our series, with only 2 patients having to discontinue treatment due to severe infection. Other minor side effects ORTIZ-SANJUÁN ET AL such as mild leukopenia and neutropenia and increased levels of hepatic enzymes were transient, and discontinuation of TCZ was not required. To the best of our knowledge, this is the largest series of TCZ-treated patients with AOSD refractory to conventional immunosuppressive drugs and, in some cases, to other biologic therapies. TCZ treatment resulted in rapid and maintained clinical and laboratory improvement in these patients. Although TCZ showed global efficacy, joint manifestations were more refractory to treatment than were systemic manifestations. The efficacy and safety of TCZ in AOSD should be assessed in prospective controlled clinical trials. AUTHOR CONTRIBUTIONS All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. Drs. Blanco and González-Gay had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study conception and design. Ortiz-Sanjuán, Blanco, Calvo-Rio, Narvaez, Romero, Olivé, Castañeda, Flores, Hernández, Mata, Vilamajo, Giraldo, Caracuel, Freire, Arango, Llobet, Arija, Marras, Moll-Tuduri, Plasencia-Rodriguez, Roselló, Urruticoechea, VellosoFeijoo, del Blanco, González-Vela, Rueda-Gotor, Pina, Loricera, González-Gay. Acquisition of data. Ortiz-Sanjuán, Blanco, Calvo-Rio, Narvaez, Romero, Olivé, Castañeda, Flores, Hernández, Mata, Vilamajo, Giraldo, Caracuel, Freire, Arango, Llobet, Arija, Marras, Moll-Tuduri, Plasencia-Rodriguez, Roselló, Urruticoechea, Velloso-Feijoo, del Blanco, González-Vela, Rueda-Gotor, Pina, Loricera, González-Gay. Analysis and interpretation of data. Ortiz-Sanjuán, Blanco, Calvo-Rio, Castañeda, González-Gay. REFERENCES 1. Riera E, Olive A, Narvaez J, Holgado S, Santo P, Mateo L, et al. Adult onset Still’s disease: review of 41 cases. Clin Exp Rheumatol 2011;29:331–6. 2. Crispin JC, Martinez-Banos D, Alcocer-Varela J. Adult-onset Still disease as the cause of fever of unknown origin. Medicine (Baltimore) 2005;84:331–7. 3. Hoshino T, Ohta A, Yang D, Kawamoto M, Kikuchi M, Inoue Y, et al. Elevated serum interleukin 6, interferon-", and tumor necrosis factor-! levels in patients with adult Still’s disease. J Rheumatol 1998;25:396–8. 4. Fujii T, Nojima T, Yasuoka H, Satoh S, Nakamura K, Kuwana M, et al. Cytokine and immunogenetic profiles in Japanese patients with adult Still’s disease: association with chronic articular disease. Rheumatology (Oxford) 2001;40:1398–404. 5. Chen DY, Lan JL, Lin FJ, Hsieh TY. Association of intercellular adhesion molecule-1 with clinical manifestations and interleukin18 in patients with active, untreated adult-onset Still’s disease. Arthritis Rheum 2005;53:320–7. 6. Kremer JM, Blanco R, Brzosko M, Burgos-Vargas R, Halland AM, Vernon E, et al. Tocilizumab inhibits structural joint damage in rheumatoid arthritis patients with inadequate responses to methotrexate: results from the double-blind treatment phase of a randomized placebo-controlled trial of tocilizumab safety and prevention of structural joint damage at one year. Arthritis Rheum 2011;63:609–21. TOCILIZUMAB IN AOSD REFRACTORY TO STANDARD TREATMENT 7. De Benedetti F, Brunner HI, Ruperto N, Kenwright A, Wright S, Calvo I, et al. Randomized trial of tocilizumab in systemic juvenile idiopathic arthritis. N Engl J Med 2012;367:2385–95. 8. Puechal X, deBandt M, Berthelot JM, Breban M, Dubost JJ, Fain O, et al. Tocilizumab in refractory adult Still’s disease. Arthritis Care Res (Hoboken) 2011;63:155–9. 9. De Bandt M, Saint-Marcoux B. Tocilizumab for multirefractory adult-onset Still’s disease. Ann Rheum Dis 2009;68:153–4. 10. Perdan-Pirkmajer K, Praprotnik S, Tomsic M. A case of refractory adult-onset Still’s disease successfully controlled with tocilizumab and a review of the literature. Clin Rheumatol 2010;29:1465–7. 11. Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult Still’s disease. J Rheumatol 1992;19:424–30. 12. Schoels MM, van der Heijde D, Breedveld FC, Burmester GR, Dougados M, Emery P, et al. Blocking the effects of interleukin-6 in rheumatoid arthritis and other inflammatory rheumatic dis- 13. 14. 15. 16. 1665 eases: systematic literature review and meta-analysis informing a consensus statement. Ann Rheum Dis 2013;72:583–9. Rueda Gotor J, Blanco Alonso R. Tocilizumab in rheumatoid arthritis. Reumatol Clin 2011;6(Suppl 3):29–32. Elkayam O, Jiries N, Dranitzki Z, Kivity S, Lidar M, Levy O, et al. Tocilizumab in adult Still’s disease: the Israeli experience [abstract]. Arthritis Rheum 2012;64 Suppl:S83. De Boysson H, Fevrier J, Nicolle A, Auzary C, Geffray L. Tocilizumab in the treatment of the adult-onset Still’s disease: current clinical evidence. Clin Rheumatol 2013;32:141–7. Van Gestel AM, Prevoo ML, van ’t Hof MA, van Rijswijk MH, van de Putte LB, van Riel PL. Development and validation of the European League Against Rheumatism response criteria for rheumatoid arthritis: comparison with the preliminary American College of Rheumatology and the World Health Organization/ International League Against Rheumatism criteria. Arthritis Rheum 1996;39:34–40.