Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
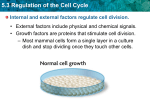
توفيق جاسم.د الجراحة العامة/المرحلة الرابعة جامعة بغداد/كلية طب الكندي 2014-2015 The abdominal wall Burst abdomen(abdominal dehiscence)and incisional hernia It occurs after 1-2% of laparotomies, mostly 6-8th day after operation, an abdominal wound bursts open and viscera are extruded. An incisional hernia usually starts as a symptomless partial distruption of the deeper layers during the immediate or early postoperative period A serosanguinous(pink) discharge from the wound is a forerunner in 50% of cases. It signifies that intraperitoneal contents are lying extraperitoneally. Patient feel something give way. If skin sutures have been removed, omentum or coils of intestine may be forced through the wound. Pain and shock are often absent 1 An emergency operation is required to replace the bowel, relieve any obstruction and resutures the wound. While awaiting operation, reassure the patient, cover the wound with a sterile towel. NGT and IV fluid commenced Factor relating to the incidence of burst abdomen and incisional hernia 1-Technique of wound closure a) Choice of suture material; catgut leads to a higher incidence of bursts than the use of non-absorbable monofilament and should never be used b) Method of closure; interrupted suturing has A low incidence than continuous. When continuous suturing is used, the length of suture should at least four times the length of the incision c) Drainage; drainage directly through a wound leads to a higher incidence of bursts than drainage through a separate(stab)incision 2-factors relating to incisions Midline and vertical incisions have a greater tendency to burst than those which are transverse 3-reasons for initial operation Deep wound infection, operations on pancreas with enzyme leakage, and on obstructed cases are other reasons of bursts 2 4-coughing, vomiting, distension Any violent coughing after removal of endotracheal tube and suction of laryngopharynx, postoperative cough, vomiting and distension can lead to wound disruption 5-general condition of the patient Obesity, jaundice, malignant disease, hypoprotienemia and anaemia, steroids and abdominal wounds in pregnancy Incisional(postoperative)hernia 3 This iatrogenic hernia occurs in 2-10% of all abdominal operations secondary to breakdown of the fascial closure of prior surgery. Even after repair, recurrence rates approach 2045%. incisional or Ventral Hernias may occur in the area of any prior surgical incision, and can vary in size from very small, to very large and complex. They develop as the result of disruption along or adjacent to the area of abdominal wall suturing. These hernias present as a bulge or protrusion at or near the area of the prior incision scar. Virtually any prior abdominal operation can subsequently develop an Incisional Hernia at the scar area, including those from large abdominal procedures (intestinal surgery, vascular surgery), to small incisions (Appendectomy, or Laparoscopy). These hernias can occur at any incision, but tend to occur more commonly along a straight line from the breastbone straight down to the pubis, and are more complex in these regions. Hernias in this area have a high rate of recurrence if repaired via a simple suture technique under tension and it is especially advised that these be repaired via a TENSION FREE repair method using mesh. These hernias may develop soon after the original surgery, or at any time thereafter. Incisional Hernias gradually increase in size once they develop and become progressively symptomatic. A bulge may not be evident at the hernia site initially, and pain may be the only early hernia symptom. These hernias develop in many cases as a result of too much tension placed when closing the abdominal incision, as stated above. Tension creates poor healing, swelling, wound separation and eventual Incisional Hernia formation. Management 4 They require urgent repair with reinforcing mesh used in large hernias. This is required particularly where the patient is obese.2 Recurrence occurs in up to 50% of large hernias. Aetiology Incisional hernia occurs often in obese individuals. Persistent postoperative cough and abdominal distension are its precursors. High incidence after operations for peritonitis. The placing of a drainage tube through a separate stab incision reduce the frequency Usually starts as a symptomless partial disruption of the deeper layers of laparotomy wound immediately or very early postoperative period Clinical features It may occur through a small portion of the scar, often the lower end. More often there is a diffuse bulging of the whole length of the incision. It usually increases steadily in size and more and more of its contents become irreducible. The overlying skin may be so thin and atrophied that peristalsis can be seen in the underlying intestine. Attacks of partial intestinal obstruction are common as strangulation is liable to occur at the neck or in a loculus Treatment Palliative An abdominal belt is satisfactory especially in cases of a hernia through an upper abdominal incision Operation If the patient is obese, weight reduction preced the operation. To attempt to return the contents of a very large hernia to the main abdominal cavity if they have not been there for several years, there is risk of failure of the hernioplasty, paralytic ileus from visceral compression and pulmonary complications. Divarication of the recti abdominis Is seen principally in elderly multiparus patients. When the patient strains, a gap can be seen between the recti through which the abdominal contents bulge. When the abdomen is relaxed, the finger can be introduced between the recti Treatment An abdominal belt is all that is required. There is no risk of strangulation. A similar condition is met with in babies, no treatment is necessary, spontaneous cure will result Tearing of the inferior epigastric artery 5 Occurs in three types of patients; elderly thin feeble women, middle aged athletic muscular men and pregnant women. The site of the haematoma is usually at the level of the arcuate line Clinical features Usually following bout of coughing, or a sudden blow to the abdominal wall, tender lump appear. Occasionally a haematoma appear lateral to the rectus sheath Differential diagnosis Twisted ovarian cyst Appendix abscess Strangulatet spigelian hernia Treatment With rest, a small haematoma may resolve, but sometimes renewed haemorrhage causes the haematoma to rupture into the peritoneal cavity. Thus, its saver to operate early, evacuate the clot and ligate the artery Superficial cellulitis Oedematous skin at the site of stitches. On palpation, induration and tenderness of the area involved. A stitch should be removed, and if pus or seropus escapes it should be sent for bacteriological examination. Treatment with broad-spectrum antibiotic Deep cellulitis Browny oedema towards one or both flanks, may be of the scrotum or vulva. Antibiotic is the mainstay of treatment. If tenderness persists, draiage is advisable Progressive postoperative bacterial synergistic gangrene A rare complication after laparotomy, usually for a perforated viscus(appendicitis), after gall bladder operations, colectomy for ulcerative colitis, and even after drainage of an empyema thoracic. Its due to synergistic action of microaerophilic non-haemolytic streptococci and, staphylococcus. The skin near the wound exhibits signs of cellulitis, central purplish zone with an outer brilliant red zone, extremely tender. The gangrenous skin sloughes. Finally septicemia with associated multiorgan failure supervene Treatment Identification of the organisms and their sensitivity to antibiotic is essential.broad spectrum antibiotic with metronidazole should be given. Surgical debridement of all the necrotic and infected tissue should be performed. Hyperbaric oxygen can be life-saving. Cellulitis due to bacteroids may give no bacterial growth on culture and may be missed Amoebic cutis Lethal complication of amoebic colitis, liver abscess or empyema Neoplasms of the abdominal wall 6 Desmoids tumour A benign soft tissue(connective tissue) tumor that occurs most often in young adults and involves the limbs or trunk but can also arise in the abdomen or thorax.in the abdominal wall , it occure in the musculoaponeurotic structures They never metastasize (spread to other parts of the body). However, they are very difficult to remove because they intertwine extensively with the surrounding tissues. These tumors look like dense scar tissue. Just like scar tissue, they adhere tenaciously to surrounding structures and organs. Desmoids tumor, also called aggressive fibromatoses , are locally aggressive. This means that they can grow into and even destroy adjacent normal tissues, even bones. most doctors consider desmoid tumors to be benign and not malignant. But regardless of the name, tumor-related destruction of vital structures and/or organs can be fatal. Desmoid tumors are uncommon. The estimated incidence in the general population is 2-4 per million people per year Desmoid tumors may occur sporadically, or in association with familial adenomatous polyposis (FAP) . The combination of familial polyposis and desmoid tumors, along with other non-intestinal manifestations, has been referred to as Gardner’s syndrome Aetiology 80% occur in women. The neoplasm occurs occasionally in scars of abdominal operation wounds. Trauma e.x. stretching of muscle during pregnancy may play a role, muscle haematoma also may be the cause. It may occur in a cases of familial adenomatous polyposis. Unlike fibroma elsewhere, no sarcomatous change occurs Clinical Presentation Painless or slightly painful swelling or lump.Pain or soreness caused by compressed nerves or muscles.Limping when the tumors occur in the legs . when tumors form in the abdomen, it may cause bowel obstruction, change in bowel habits, pain or rectal bleeding Diagnosis A biopsy specimen is necessary to diagnose a desmoid tumor. Ultrasound is often the first method of examination of a soft tissue tumor. If the mass is solid, a CT and/or MRI scan is used to determine whether it adheres to nearby structures and whether it can be safely removed. 7 Behavior of Desmoid Tumors Although they do not metastasize, desmoid tumors are locally aggressive, infiltrating and sometimes causing destruction of adjacent vital structures and organs. Treatment Treatment of desmoid tumors is indicated when they cause symptoms, when there is risk to adjacent structures, or when they create cosmetic concerns . Under some Medical Therapy Clear evidence suggests the hormonal dependency of some desmoid tumors. Hormonal agents (an anti-estrogen) such as tamoxifen (brand name Nolvadex), toremifene, raloxifene and progesterones have all been used, often in combination with NSAIDs. Of these, tamoxifen has been used most widely.. Treatment with hormones and NSAIDs, both alone and in combination, result in detectable improvement in pain and other symptoms in about half of patients, but lead to major shrinkage in only a small minority of patients and complete disappearance of the tumor in very few cases. Radiation Therapy Radiation therapy is an effective option for many patients who cannot have surgery, or as an adjunct to surgery or chemotherapy. Chemotherapy Chemotherapy may be effective in patients with unresectable tumors, and is often used if tumors do not respond to tamoxifen and/or NSAID 8