Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
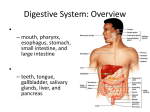
PATHOPHYSIOLOGY OF ORAL CAVITY Roman Benacka, MD, PhD Department of pathophysiology LF UPJŠ Content Oral manifestations of systemic disease Oral manifestations of drug reactions Contact stomatitis (irritation & allergy) Bacterial & viral oral infections as focuses for systemic spreading Nutritional defects - avitaminoses Topic 1 Oral manifestation of systemic diseases Gastrointestinal diseases Haematological disorders Connective tissue disorders Pulmonary disorders AIDS & Immunodeficiencies Cutaneous disorders Endocrine disorders Topic 1A Gastrointestinal diseases Crohn disease transmural inflammation, noncaseating granulomas, and fissures in bowels manifests systemically as arthritis, clubbing of the fingers, sacroiliitis, and erythaema nodosum intraoral signs occur in 8-9% of cases and may precede intestinal involvement: diffuse labial, gingival, or mucosal swelling; cobblestoning of the buccal mucosa; apthous ulcers, mucosal tags and angular cheilitis Ulcerative colitis oral lesions coincide with exacerbations of the colonic disease occur in 510% of patients aphthous ulcerations or superficial hemorrhagic ulcers, angular stomatitis Gastroesophageal reflux disease (GERD) regurgitation causes acidic environment (pH 1-2) in the oral cavity dissolving and errosion of enamel differing from caries; Caries is not increased commonly seen on the palatal surfaces exposing underlying dentin, Topic 1A Gastrointestinal diseases Hepatopathia and bilirubin metabolism and secretion disorders jaundice (yellow pigmentation) - deposition of bilirubin (25-30 mg/l) in the submucosa - mucosa on the soft palate and in the sublingual region Chronic liver disease excessive gingival bleeding with minor surgery - liver synthesizes clotting factors, vitamin K requires proper liver functioning to be adequately absorbed Hepatitis C leading infectious cause of chronic liver disease worldwide association between hepatitis C and erosive oral lichen planus transmission from patient to dentist Topic 1B Haematological disorders Anaemias oral mucosa exhibit pallor decreased resistance to infection - glossitis, recurrent aphthae, candidal infections, and angular stomatitis glossitis, tongue is reddened, the papillae are atrophic (first sign of folate or vitamin B-12 deficiency anaemia) angular stomatitis caused by a candidal infection (iron deficiency anaemia) Langerhans histiocytosis (histiocytosis X) abnormal histiocytic and eosinophilic proliferation - most common form is the eosinophilic granuloma in young adults. may present as a localized proliferation, or it may present with extensive systemic involvement. Oral sy.: a) ulcerations on the gingiva (destructive gingivitis), palate, and floor of the mouth. b) progressive alveolar bone loss with dental extrusion and characteristic floating teeth Topic 1C Connective tissue disorders Sjögren syndrome Def.: second most common autoimmune disease (90% are female; 3% of women over 50 years) manifested by thick and mucinous, or absent secretes (saliva, tears) -> sicca syndrome - keratoconjunctivitis sicca, xerostomia, etc.; lymphocytic Oral sy.: xerostomia (dry, red, and wrinkled mucosa) tongue has a cobblestone like appearance (atrophy of the papillae), difficulty in swallowing and eating, increased dental caries (sugar is not washed away by saliva), predisposition to infection (common is candidiasis) Kawasaki disease (mucocutaneous lymph node syndrome) Def.: vasculitis in medium and large arteries with a corresponding cutaneous lymph node syndrome; replaced rheumatic fever as the primary cause of childhood (< 5 years) heart disease Symptoms: acute cervical adenopathy, oedema & erythema, desquamation of the hands and feet, fever, polymorphous exanthema - rash; acute cervical adenopathy; aneurysm and myocardial infarction, myocarditis Oral sy.: papillae swelling on the surface of the tongue (strawberry tongue) intense erythema of the mucosal surfaces, labia are cracked, cherry red, swollen, and hemorrhagic Topic 1D Pulmonary disorders Wegener granulomatosis Def.: necrotizing vasculitis of small-to-medium arteries and veins + necrotizing granulomas of the upper and lower airways +/necrotizing glomerulonephritis. Oral and skin manifestations may be correlated with disease progression, thereby serving a prognostic purpose Oral sy.: in 97% of patients ulcerations on the buccal mucosa or palate gingival hyperplasia - is a path gnomonic finding: swollen, reddened, and granular appearance to the gingivae (termed strawberry gums) start as bright red-to-purple friable diffuse papules originate on the labial interdental papillae tooth and alveolar bone loss are common Topic 1D Pulmonary disorders Sarcoidosis Def.: idiopathic systemic inflammatory disease involving nearly any organ system (liver, heart, spleen, eyes, kidneys), pulmonary manifestations are the most common, cutaneous (5-20% of patients). oral sy presents after systemic symptoms Oral sy.: multiple painless ulcerations of the gingiva, buccal mucosa, labia, and palate + salivary gland tumorlike swellings. Rarely, sarcoidosis involves the tongue swelling, enlargement, and ulcerations. Heerfordt syndrome - triade: parotid gland swelling, xerostomia, uveitis, and facial nerve palsy. Amyloidosis Def.: deposition of proteins in body tissues leading to tissue damage. Amyloidosis is classified as primary, stemming from multiple myeloma or an idiopathic disease, or as secondary, stemming from a chronic or inflammatory disease process Symptoms: affects the skin, heart, tongue, and GI tract, while the secondary form, although more common, has no cutaneous manifestations. Oral sy.: a) macroglossia (the most common; 20% of patients) with lateral ridging due to teeth indentation; b) loss of taste, xerostomia may result from amyloid deposition in the salivary glands Submandibular swelling occurs subsequent to tongue enlargement and may lead to respiratory obstruction. Topic 1E AIDS and other immunodeficiencies Candidiasis repeated oral candidiasis is the first sign in 90% of patients with HIV. Most common is pseudomembranous type - white plaques on the soft and hard palates, buccal mucosa (most commonly), and tongue that leave a reddened area when scraped. Herpes simplex virus (HSV) double-stranded DNA virus that has 2 serotypes: HSV-1 and HSV-2 Oral sy.: oro-labial vesicles (lips, tongue, gingiva, hard palate) that are rupturing, and leaving a small, irregular, and painful crusted weeping ulceration or fissures on dorsal part of tongue. May extend to esophagus. Stress, fever, and sunlight may precipitate reactivation. Until disproved, all perineal and ulcerations should be considered HSV in patients who are infected with HIV. Epstein-Barr virus (EBV) - Hairy leukoplakia (HL) adherent corrugated white plaques most commonly on the lateral portions of the tongue (5% of patients) Kaposi sarcoma (KS) - the most common skin or oral malignancy (lymph node enlargement), in patients who are HIV positive Oral sy.: brown, bluish, purple, or red patches or papules on the hard palate, mucosa, and gingiva that ulcerate, and bleed Cytomegalovirus (CMV) double-stranded DNA virus (60% of people being seropositive but asymptomatic) symptomatic disease - organ or bone narrow transplantation or HIV infection : retinitis (30% ; blindness). pneumonia (5%; lung failure) Oral sy.: very rare – aphthous-like ulcerations on the lips, tongue, pharynx, or any mucosal site Candidiasis Primary herpetic gingivostomatitis (HEV 1) affects mostly children or young adults. Inside the oral cavity, herpes simplex typically affects only keratinized tissues, such as the gingiva or the hard palate. Intraoral herpes zoster closely resembles recurrent human herpesvirus 1 (HHV-1) infection Topic 1F Cutaneous manifestations Psoriasis Def.: chronic papulosquamous inflammatory condition of the skin affecting 2% of population (20-30y) Oral sy.: oral psoriasis rarely manifests without cutaneous involvement: manifest on the lips, tongue, palate, buccal mucosa, and gingiva. Psoriatic tongue involvement appears indistinguishable from geographic tongue Acanthosis nigricans Def.: is a cutaneous disorder of hyperpigmentation and papillomatosis that may precede or coincide with a variety of benign, familial, or malignant disorders. Most cases of AN are rare benign congenital (AD) disorder. Malignancy associated AN (MAN) presents commonly with adenocarcinoma of the stomach. Oral sy.: in 25-50% of MAN patients - cutaneous and oral papillomatosis, gingival hyperplasia hypertrophy of the papillae along the dorsal surface and lateral edge of the tongue. Topic 1F Endocrine diseases Diabetes mellitus may increase the prevalence, incidence, or severity of gingivitis and periodontitis. Oral sy.: the severity and prevalence of periodontitis are increased in persons with diabetes and are worse in persons with poorly controlled diabetes Periodontitis may exacerbate diabetes by decreasing glycemic control. This effect indicates a degree of synergism and a link between the 2 diseases. Addison disease Oral sy.: black tinge of gingivae and teeth Topic 2 ORAL MANIFESTATION OF DRUGS Oral manifestations Finding Drugs Xerostomia antidepressants and antipsychotics, antihypertensives, antihistamines, anticholinergics, decongestants Candidiasis In correlation with dose and frequency of the steroids Gingival calcium channel blockers (nifedipine (38% of patients), enlargement nimodipine, nitrendipine, oxidipine, verapamil), dihydropyridines (hyperplasia) (bleomycin), cyclosporine ( up to 85% of patients), phenytoin (~ 50% of patients), valproate (antiepileptic) Swelling penicillins, aspirin, ACE inhibitors Ulceration Antineoplastics (methotrexate, 5-fluorouracil, doxorubicin, melphalan), barbiturates; phenazone derivatives; salicylates; sulfonamides; tetracycline; direct contact with compounds containing aspirin, hydrogen peroxide, or phenol Candidiasis after prolonged steroid therapy in reumatism Minocycline - associated bluish gray hue of the alveolar mucosa pigmentation in a patient who had used the drug for several months to treat severe acne. Gingival enlargement in a man with a several-year history of using calcium channel blockers Erythema multiforme: multiple erosions on the lips and tongue. Ulcers in buccal mucosa due to coxsackie virus infection Oral manifestations Finding Drugs Vesico ulcerative mucositis nonsteroidal anti-inflammatory drugs (indomethacin, gold salts, naproxen), meprobamate, methyldopa, phenylbutazone, propranolol, spironolactone, thiazides, and tolbutamide Pigmentation amiodarone, antimalarials (chloroquine, hydrochloroquine, hydroxychloroquine, quinacrine, quinidine), bisulfan, clofazimine, cyclophosphamide, estrogen, ketoconazole, minocycline, phenolphthalein, chlorpromazine Pemphigoidlike antibiotics (antimalarials, penicillins, sulfonamides), barbiturates, and salicylates Pemphiguslike antirheumatics (penicillamine, ibuprofen, phenacetin), cardiovascular drugs (furosemide, captopril, clonidine), antibiotics (penicillins, sulfonamides), antimicrobials, thiolcontaining drugs, and sulfonamide derivatives Topic 3 CONTACT WITH FOREIGN MATERAILS Contact Stomatitis Def.: inflammatory reaction of the oral mucosa by contact with irritants or allergens. Pathophysiol.: oral mucosa is resistant to irritants and allergens High vascularization that favors absorption and prevents prolonged contact with allergens Low density of Langerhans cells and T lymphocytes Dilution of irritants and allergens by saliva that also buffers alkaline compounds Occurence: may occur at any age. Irritant reactions appear to be more common than allergic reactions. Burning mouth syndrome that almost exclusively affects women. Contact Stomatitis - Causes Ingredients of candies and chewing gums cinnamon compounds, menthol, propolis (a strong sensitizer often used in the oral cavity because of its antiseptic properties) Local use of drugs antibiotics, anesthetics, antiseptics, and steroids, desinfectives e.g. chlorhexidine, quaternary ammonium compounds) Rubber and latex e.g. gloves, dams, orthodontic elastics, bite blocks Foods (rarely) Children with atopic dermatitis and a food allergy may develop lip swelling and stomatitis after contact with fruits Cosmetics Ingredients (ricinoleic acid, colophony derivatives, sunscreens lipsticks, lip balms) Contact Stomatitis - Causes Ingredients of dentifrices, mouthwashes, dental cleaners Flavoring agents (e.g. cinnamon compounds, eugenol, menthol) Ingredients of dental restorations Amalgam fillings contain mercury compounds (45-60%) and often gold, palladium, platinum. Metallic mercury - common sensitizer Dental cement used for sealing pulp canals (eugenol, balsam of Peru, colophony) Acrylic fillings (polymerized acrylate is relatively free of allergens) Ingredients of dental prosthesis Metal prostheses - may release nickel (present in dental braces, bridges, and crowns), especially poorly made/ corroded Acrylate sensitization is a common occupational problem in dentists and dental technicians. Allergic contact reaction due to nickel in a dental brace. Irritant contact stomatitis of the tongue. Leukoplakialike lesion in a patient who is allergic to mercury. Contact urticaria of the lip due to food allergy Acute allergic stomatitis involving the oral mucosa and the lip due to benzocaine. Allergic contact stomatitis on the gingiva in a patient with a positive patch test result to nickel, palladium, and mercury. Contact urticaria of the tongue in a patient with latex allergy. Lichen planus–like lesion adjacent to a dental restoration. Allergic contact dermatitis involving the lips and the perioral area due to propolis Manifestations of contact stomatitis Erythema and swelling - may be localized or diffuse, ingredients of mouthwashes and toothpastes, dental materials, and chewing gum flavorings Erosions/ulcerations - evolution of vesicles and blisters rarely seen in the mouth. outlined, whitish, rough, macerated areas. Ulcerations are usually covered by a yellow-white exudate and may present with an erythematous halo. Chemical burns are not frequent because the oral mucosa is resistant to heat and acid or alkaline compounds. Prolonged contact with aspirin or vitamin C tablets, or contact with irritants used for dental care. Allergic contact stomatitis from metal salts or acrylates rarely causes mouth ulcerations. Contact urticaria Swelling of the lips, the tongue, the buccal mucosa, and the gingiva develops suddenly with intense itching due to allergy to foods. Severe cases may be associated with upper airway obstruction. Chemical burns result in tissue necrosis produced by a chemical agent used by the practitioner or the patient to relieve pain. The lesion takes the aspect of a whitish plaque which can be removed, leaving an erosive, painful surface The bitten mucosa - alteration of normal tissue - whitish multiple erosions, abrasions and slight sloughing of the most superficial layers of the mucosa. It affects the buccal mucosa, lips and tongue wherever they can be reached by the patient´s bite. Manifestations of contact stomatitis Lichen planus–like lesions May occur at the site of mucosal contact with amalgam restorations - lesions are typically localized. Sensitization to gold, palladium chloride, and copper sulfate Leukoplakia-like lesions Contact sensitization from nickel and other metals commonly localized in the medial part of the cheek. Burning mouth syndrome Burning pain and dryness of mucosa improving during meals. Although contact allergy (especially to mercury) has often been implicated, the disorder most likely has a psychogenic basis. Other Compliants Paresthesia, numbness, bad taste, salivation, itching White-colored findings Lichen planus - chronic dermatosis which may affect both skin and mucosa. Oral intercrossing white lines that give the appearance of a weave or net (arboriform).In some patients the lesions may disappear spontaneously Leukoplakia - whitish lesion which does not slough off when scraped, histologically presents as a spot, keratosis of wartlike. They are produced by continued chronic irritation in people with some sort of predisposition (smoking habits, the rough and or sharp surfaces of teeth, and or broken or ill-adapted partial and full dentures) Topic 4 BACTERIAL MOUTH INFECTIONS Bacterial mouth infections Oral cavity contains some of the most varied and vast flora in the body which - adhere to the teeth, the gingival sulcus, the tongue, and the buccal mucosa. Number and proportion of flora changes with the age and systemic changes (pregnancy, drug intake) Alterations in the flow and composition of salivary fluid and in the levels and activity of defense components (e.g., immunoglobulins, cytokines) in the saliva. Oral microbiota participate in various systemic diseases. Foci of infection in the oral cavity arising from chronic periodontitis (inflammation of the periodontal attachment of the teeth and the alveolar bone) or chronic periapical abscesses (i.e., inflammation and abscess of the tissue attached to the apex of the root). Bacterial infections of the mouth. A 72-year-old man with severe periodontal disease Bacterial infections caused severe alveolar bone loss and periodontitis in X-ray scan Odontogenic abscess Inflammatory swelling Origin of infection focus Odontogenic abscess Pathways of spreading Periodontal disease The relative risk of cardiovascular disease is doubled in persons with periodontal disease Periodontal and cardiovascular disease share many common risk and socioeconomic factors, particularly smoking, which is a powerful risk factor for both diseases. The chronic inflammatory state and microbial burden in persons with periodontal disease may predispose to cardiovascular disease in ways proposed for other infections, such as with Chlamydia pneumoniae. Bacterial endocarditis due to oral foci of infection Etiology: Streptococcus viridans; Staphylococci (> 80% of cases) Dental manipulation 90% (brushing teeth, chewing gum, eating -> transient bacteremia; 8-10% oral infections - Transient oral bacteremia after tooth extractions lasting less than 15-30 minutes Occurence: In developed countries 1-5 cases per 100,000 population per year; mortality rate up to 80% Patients with congenital or acquired cardiovascular defects are at risk for BE. Mortality rate of 10-80%. Symptoms: Septic emboli, congestive heart failure with infection-induced valvular damage, splenomegaly, splenic abscesses. Neurologic manifestations (delirium, headache, and meningeal irritation) may be caused by mycotic aneurysms. Cardiovascular diseases due to oral foci of infection Manifestations: atherogenesis, thromboembolia coronary heart disease cardiomyopathy Etiology: Chronic periodontal infections Streptococcus sanguis oral Gpositive bacteria & G -negative Porphyromonas gingivalis found in dental plaque Mechanisms: bacterias enter the bloodstream, invade and proliferate within heart and coronary artery endothelial cells (found in carotid and coronary atheromas) direct effect on atheroma formation & induce platelet aggregation, thrombus formation Glomerulonephritis due to oral foci of infections Occurence: Patients (2-12 years) with poor oral hygiene, twice as common in males as in females most common primary renal disease in developing countries Etiology: Streptococcus mitis or Streptococcus mutans bacteremia Pathology: In the early phases - diffuse glomerular and endocapillary proliferation + polymorphonuclear infiltration In later phases - mesangial deposits Manifestations: acute nephritic syndrome - abrupt onset of gross haematuria and proteinuria oliguria, oedema, hypertension (80% of cases ) 10-21 days after the onset of bacteraemia. Non-specific symptoms, such as malaise, weakness, and nausea, are frequent. Dull lumbar pain is present in 5-10% of patients Topic 5 Deficiency or excess of vitamins Deficiency or excess of minerals Deficiency or excess of main nutrients Oral manifestation of nutrient defects Vitamin-related disorders VITAMIN DEFICIENCY OR EXCESS Vitamin C Deficiency: Scurvy - red swollen gingiva; gingival friability; periodontal destruction; increased tooth mobility & exfoliation; sore burning mouth; soft tissue ulceration; increased risk of candidiasis; malformed teeth (inadequate dentine). Excess: return to normal levels of the vitamin cause deficiency (rebound scurvy). Vitamin D Deficiency: Abnormal bone regeneration osteoporosis; osteomalacia; incomplete mineralisation of teeth & alveolar bone; rickets. Excess: Pulp calcification; enamel hypoplasia. Vitamin K Deficiency: Increased risk of bleeding & candidiasis Scurvy Scurvy-red swollen gingiva Vitamin C deficiency Vitamin B2,B3,B6 deficiency Folic acid, B12 deficiency Iron deficiency periodontal destruction; increased tooth mobility & exfoliation; sore burning mouth; soft tissue ulceration; candidiasis; malformed teeth (inadequate dentine). Angular cheilosis Vitamin-related disorders Vitamin A Deficiency: Inadequate cell differentiation-impaired healing & tissue regeneration; desquamation of oral mucosa; keratosis; increased risk of candidiasis; gingival hypertrophy & inflammation; leukoplakia; decreased taste sensitivity; xerostomia; disturbed or arrested enamel development; irregular tubular dentine formation and increased caries risk. Excess: Impairs cell differentiation & epithelialisation-impaired healing (mimics deficiency). Vitamin B2 (Riboflavin) Deficiency: Angular cheilosis; atrophy of filliform papillae; enlarged fungiform papillae; shiny red lips; magenta tongue; sore tongue. Vitamin B3 (Niacin) Deficiency: Angular cheilosis; mucositis; stomatitis; oral pain; ulceration; ulcerative gingivitis; denuded tongue; glossitis; glossodynia; tip of tongue is red & swollen; dorsum is dry & smooth. Vitamin-related disorders Folic acid Deficiency: Angular cheilosis; mucositis; stomatitis; sore or burning mouth; increased risk of candidiasis; inflamed gingiva; glossitis oral pain; ulceration; ulcerative gingivitis; denuded tongue; glossitis; glossodynia; tip or borders of tongue red & swollen; slick bald pale; apthous ulcers. Vitamin B6 Deficiency: Angular cheilosis; sore or burning mouth; glossitis; (Pyridoxine) glossodynia. Deficiency: Angular cheilosis; mucositis; stomatitis; sore or burning mouth; haemorrhage gingiva; halitosis; epithelial dysplasia of oral mucosa; oral paresthesia; detachment of Vitamin B12 periodontal fibres; loss or distortion of taste; glossitis oral (Cyanocoba pain; ulceration; ulcerative gingivitis; denuded tongue; lamin) glossitis; glossodynia; tongue is "beefy", red, smooth & glossy; delayed wound healing; xerostomia; bone loss; apthous ulcers. Mineral disorders MINERAL DEFICIENCY OR EXCESS Fluoride Deficiency: Decreased resistance to caries. Excess: Disturbed amelogenesis; mottled/stained enamel; enamel hypoplasia (fluorosis) Iron Deficiency: Angular cheilosis; pallor of lips and oral mucosa; sore, burning tongue; atrophy/denudation of filliform papillae; increased risk of candidiasis; glossitis. Calcium Deficiency: Incomplete mineralisation of teeth; rickets; osteomalacia; osteoporosis; excessive bone resorption & bone fragility; increased tendency to haemorrhage; increased tooth mobility & premature loss. Copper Deficiency: Decreased trabeculae of alveolar bone; decreased tissue vascularity; increased tissue fragility. Mineral disorders Zinc Deficiency: Loss or distortion of taste & smell acuity; loss of tongue sensation; delayed wound healing; impaired keratinisation of epithelial cells; epithelial thickening; atrophic oral mucosa, increased susceptibility to periodontal disease, candidiasis, xerostomia & caries if deficient during tooth formation. Magnesium Deficiency: Alveolar bone fragility; gingival hypertrophy Phosphorus Deficiency: Incomplete mineralisation of teeth; increased susceptibility to caries if deficient during tooth formation; increased susceptibility to periodontal disease due to effects on alveolar bone Main nutrients NUTRIENT DEFICIENCY OR EXCESS Carbohydrate Deficiency: Caries rate generally decreases when carbohydrate intakes decreases. Excess: Increased frequency of intake of all carbohydrates (except fibre) is a causative risk factor for caries Fats Protein Water Deficiency: Angular cheilosis; pallor of lips and oral mucosa; sore, burning tongue; atrophy/denudation of filliform papillae; increased risk of candidiasis; glossitis Excess: No direct effect but fats may coat teeth and protect them againts cariogenic challange. Deficiency: Defects in tooth composition, eruption pattern & resistance to decay; increased susceptibitlity to soft tissue infrection poor healing/tissue regeneration. Deficiency: Dehydration and fragility of of epithelial tissue; decreased muscle strength for chewing; xerostomia; burning tongue. Changes in the tongue Thrombocytopenic Purpura Definition Thrombocytopenic purpura is a hematological disorder characterized by a decrease in platelets in the peripheral blood. Etiology nonspecific viral infection, myelotoxic agents. Clinical features red lesions in the form of petechiae, ecchymoses, hematomas, usually located on the palate and buccal mucosa (Spontaneous gingival bleeding is a constant early finding. Purpuric skin rash, epistaxis, and bleeding from the gastrointestinal and urinary tract Laboratory tests Peripheral platelet count, bone-marrow aspiration, bleeding and clotting times. Differential diagnosis Aplastic anemia, leukemias, polycythemia vera, agranulocytosis, macroglobulinemia, drug reactions. Infectious Mononucleosis Definition Infectious mononucleosis is an acute, self-limited infectious disease that primarily affects children. Etiology Epstein–Barr virus transmitted through saliva transfer. Clinical features The oral manifestations are early and common - palatal petechiae, uvular edema, tonsillar exudate, gingivitis,rarely ulcers Generalized lymphadenopathy, hepatosplenomegaly, maculopapular skin rash, and sore throat are common. Prodromal symptoms such as anorexia, malaise, headache, fatigue, and later fever occur before the clinical manifestations. Laboratory tests Heterophile antibody tests, and other specific antibody tests (Paul–Bunnell test, monospot test). Idiopathic thrombocytopenic purpura: Infectious mononucleosis: petechiae on the palate.