Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
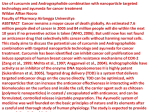
Exercise Training and Antioxidants: Effects on Rat Heart Tissue Exposed to Lead Acetate International Journal of Toxicology 30(2) 190-196 ª The Author(s) 2011 Reprints and permission: sagepub.com/journalsPermissions.nav DOI: 10.1177/1091581810392809 http://ijt.sagepub.com Valiollah Dabidi Roshan1, Mohammad Assali1, Akbar Hajizadeh Moghaddam3, Mahdi Hosseinzadeh1, and Jonathan Myers3 Abstract We have investigated the cardioprotective effects of exercise training and/or curcumin on lead acetate-induced myocardial damage. Forty rats were randomly divided into 5 groups: (1) lead acetate, (2) curcumin, (3) endurance training, (4) training þ curcumin, (5) sham groups. The rats in groups 3 and 4 experienced the treadmill running of 15 to 22 m/min for 25 to 64 minutes, 5 times a week for 8 weeks. Groups 1 to 4 received lead acetate (20 mg/kg), the sham group received curcumin solvent (ethyl oleat), and the curcumin and training þ curcumin groups received curcumin solution (30 mg/kg) intraperitoneally. Lead administration resulted in significant increases in high-sensitivity C-reactive protein (hs-CRP), creatine kinase-MB (CK-MB), malondialdehyde (MDA), and low-density lipoprotein (LDL), and significantly decreased glutathione peroxidase (GPx), Total Antioxidant Capacity (TAC), and high-density lipoprotein (HDL) levels. Treadmill running and\or curcumin supplementation resulted in a significant decrease in hs-CRP, CK-MB, MDA, and LDL levels and significantly increased GPx, TAC, and HDL levels. These results suggest a lifestyle-induced cardioprotective potential in ameliorating lead-induced cardiotoxicity. Keywords endurance training, antioxidants, lead, heart damage, rat Introduction Cardiovascular disease (CVD) is the major cause of mortality worldwide and recent studies have shown that there is an association between CVD, inflammation, and oxidative stress.1,2 Recently, the American Heart Association (AHA) published a scientific statement on the importance of air pollution in the development of cardiovascular disease.1 Lead is a ubiquitous environmental toxin that induces a broad range of physiological, biochemical, and behavioral dysfunctions. Its toxicity has been known from ancient times and affects organs with low antioxidant defense such as the heart.2-5 Recent studies have revealed the potential for lead to induce oxidative stress, and evidence has accumulated supporting the role of oxidative stress in the pathophysiology of lead poisoning.2,3 Toxic metals increase production of free radicals and decrease the availability of antioxidant reserves to respond to the resultant damage.3 The toxicity of lead is mainly connected with its influence on the enzymatic systems of cells, which leads to many biochemical disorders. It has been suggested that lead takes part in the formation of free oxygen radicals.6 Several studies have reported decreases in antioxidant enzyme activities such as glutathione peroxidase (GPx) and increases in inflammation and/or heart injury in lead-exposed animals and workers.2,3,6 Cardiovascular diseases are invariably followed by several biochemical alterations such as lipid peroxidation, free radical damage, hyperglycemia, and hyperlipidemia, which lead to qualitative and quantitative alterations of myocardium.7 Recent studies have revealed that generation of free radicals can lead to significant injuries2,3,7; hence, free radical scavengers (antioxidants) can be used as an important therapeutic method to prevent these injuries. An abundance of research suggests that lifestyle changes, including antioxidant therapy and regular physical training, are important in order to prevent chronic diseases. Despite considerable progress in the management of cardiac events by synthetic drugs, the search for indigenous cardioprotective agents continues. 1 Faculty of Physical Education and Sport Sciences, Department of Exercise Physiology, University of Mazandaran, Babolsar, Iran 2 Faculty of Biology, University of Mazandaran, Babolsar, Iran 3 Cardiology Division, VA Palo Alto Health Care System, Stanford University, Palo Alto, CA, USA Corresponding Author: Valiollah Dabidi Roshan, The University of Mazandaran (UMZ) Pasdaran Street, 47415, P.O. Box: 416, Babolsar, Iran Email: [email protected] or [email protected] Downloaded from ijt.sagepub.com at PENNSYLVANIA STATE UNIV on September 17, 2016 Dabidi Roshan et al 191 100 0.30 * 0.25 *# *# hs - CRP (mg / L) CK- MB (U / L) 80 # 60 40 20 0 0.15 0.10 # # 0.05 Sham Lead 0.00 Training Curcumin Training & Curcumin Lead Acetate (20 mg/kg) Sham Lead Training Curcumin Training & Curcumin Lead Acetate (20 mg/kg) 80 50 * 60 40 # HDL (mg / dL) LDL (mg / dL) * 0.20 # # 40 # # # 30 20 20 10 0 0 Sham Lead Training & Curcumin Lead Acetate (20 mg/kg) 10 Lead Training & Curcumin Lead Acetate (20 mg/kg) Training Curcumin 600 * # ¥$ 500 8 * # #¥ * # 6 TAC (mol / mL) GPx (m of GSH utilised / mg protein) Sham Training Curcumin * 4 2 0 * # * # 400 * 300 200 100 0 Sham Lead Training & Curcumin Lead Acetate (20 mg/kg) Training Curcumin Sham Lead Training Curcumin Training & Curcumin Lead Acetate (20 mg/kg) 60 ** MDA (nmol / mL) 50 # 40 # # 30 20 10 0 Sham Lead Training & Curcumin Lead Acetate (20 mg/kg) Training Curcumin Figure 1. Creatine kinase-MB (CK-MB), high-sensitivity C-reactive protein (hs-CRP), low-density lipoprotein (LDL), high-density lipoprotein (HDL), glutathione peroxidase (GPx), Total Antioxidant Capacity (TAC), and malondialdehyde (MDA) concentrations in experimental animals. Statistical significance P < .05: *Significantly different than sham group; # Significantly different than lead group; ¥ Significantly different than training þ lead group; $ significantly different than curcumin þ lead group. Downloaded from ijt.sagepub.com at PENNSYLVANIA STATE UNIV on September 17, 2016 192 International Journal of Toxicology 30(2) Recent emphasis on the use of natural and complementary medicines has drawn the attention of the scientific community to the potential of these treatment options. Curcumin {1,7bis (4-hydroxy-3-methoxyphenyl)-1,6-heptadiene-3,5-dione} (diferuloyl methane), the principle coloring agent present in the rhizomes of Curcuma longa (also known as turmeric) has a long history in traditional medicine. It has many therapeutic properties including antioxidant, anti-inflammatory, and anticancer activities. In addition, it is a powerful scavenger of free radicals.4,8 Moreover, it has been suggested to have a wide range of therapeutic effects in numerous conditions including chronic inflammatory diseases such as CVD. While research in this area has mainly focused on anticancer effects of curcumin and several clinical trials using curcumin have shown promising results in cancer therapy, studies of curcumin on other diseases, including CVD, are lacking. There has been a great deal of attention paid to the role of lipid peroxidation and antioxidant effects of physical training in the recent years. Many studies have reported that acute submaximal exercise increases exercise-induced lipid peroxidation. Regular physical training, on the other hand, causes an increase in the antioxidant system and a reduction in lipid peroxidation.9 It has been suggested that individuals who exercise regularly and therefore place a consistent oxidative stress on their muscles and other cells have an augmented antioxidant defense system to reduce exercise-induced oxidative risk.9 A meta-analysis from the Cochrane Database has shown that exercise training is highly effective in reducing mortality in patients with coronary artery disease (CAD).10 Despite the knowledge that lead can induce oxidative stress, studies have identified favorable effects of exercise training and/or antioxidants on certain cardiovascular biomarkers after acute exposure to air pollution.8 However, there are few data available with respect to concomitant effects of regular aerobic training and antioxidant supplementation, particularly the oxidant/antioxidant and inflammatory processes that underlie heart tissue injury during chronic exposure to lead acetate. The purpose of the current study was therefore to determine the effects of aerobic exercise, curcumin supplementation, or both of them on biomarkers of oxidative stress (GPx, Total Antioxidant Capacity (TAC), and malondialdehyde [MDA]), inflammatory (high-sensitivity C-reactive protein [hs-CRP]), and heart tissue injury (creatine kinase-MB [CK-MB]) in rats that have been chronically exposed to lead acetate. It is hypothesized that the results of this study provide novel insight about the cardiac ameliorative potential of curcumin and exercise training. Materials and Methods The experimental protocol was approved by Department of Physiology, University of Mazandaran, and was performed according to guiding procedures in the Care and Use of Animals, prepared by the Council of the American Physiological Society. Forty male Wistar rats, 8 weeks of age (initial body weight of 240 + 20 g), were obtained from the Laboratory of Animal Bearing and Multiplying at the Pasture Institute of Iran. Each rat was housed in single standard cages of polycarbonate (20 15 15), made at the Pasture Institute of Iran, in a large air-conditioned room with controlled temperature of 22 + 2 C, light-dark cycles of 12:12 hours and humidity of 50% + 5%. The pollutant standard index (PSI) was in the acceptable range as determined by the Iranian Meteorological Organization. Rats were fed with a standard rat chow provided by Pars Institute for animals and poultry with a daily regimen of 10 / 100 g body weight for each rat. Water was available ad libitum. Rats were familiarized with the laboratory environment and running on the treadmill, then were randomly assigned into 5 experimental groups of 8 rats each. The groups were defined as follows: group1—the animals were exposed to lead acetate at a concentration of 20 mg/kg in the form of a water solution (for intraperitoneal [ip] injection), 3 days weekly for 8 weeks; group 2—Curcumin (Cum) similarly received lead acetate, as well as curcumin 30 mg/kg 5 days weekly for 8 weeks (ip); group 3—endurance training (Pb þ training) —the rats in this group similarly received lead acetate, and in addition they performed progressive running exercise of 15 to 22 m/min for 25 to 64 minutes, 5 times a week; group 4—training and curcumin (Pb þ training þ Cum); the rats in this group performed a physical training protocol similar to that in group 3, and in addition received lead acetate and curcumin supplementation; group 5—the sham-operate or control group (sham); these rats received water and ethyl oleate, in the same manner and for the same duration of time as other groups. Lead acetate (Sigma) was solubilized in Milli-Q water, and curcumin was solubilized in 50% ethanol. In order to perform ip injections, curcumin was solubilized in ethyl oleate and was injected at a dose of 30 mg/kg. Curcumin was protected from light throughout the experiment.4 We are replicating a previously-reported leaddosing regimen that caused oxidative stress so that the doses of Curcumin and lead acetate were 30 and 20 mg/kg, respectively.4 All groups were anesthetized with ketamine and Xaylozine and decapitated after 12 to 14 hours overnight fasting. Blood samples were collected 24 hours after the last dose of treatment. These blood samples were initially centrifuged by a refrigerated centrifuge at 3000 rpm for 15 minutes within 30 minutes of collection and then stored at 80 C before assay; serum was separated for biochemical estimations of blood lipids and CK-MB. The body cavities were then opened and the heart was quickly excised from the aortic root. Heart tissues were weighed and placed into Petri dishes containing cold isolation medium (0.1 mol/L K2HPO4, 0.15 mol/L NaCl, pH ¼ 7.4) to remove the blood and were frozen immediately in liquid nitrogen and stored at 80 C for subsequent analysis of hs-CRP, MDA, and GPx. Tissues were homogenized in ice-cold 10 mmol/L Tris-HC1, pH 8.2, containing 0.25 mol/L sucrose, 2 mmol/L 2mercaptoethanol, 10 mmol/L sodium azide, and 0.1 mmol/L phenylmethylsulfonyl fluoride with a polytron (4 vol/wt), and centrifuged at 50 000 g (20 minutes, 4 C). The supernatants were lyophilized and stored at 20 C. The hs-CRP concentration was determined by Latex particle-enhanced Downloaded from ijt.sagepub.com at PENNSYLVANIA STATE UNIV on September 17, 2016 Dabidi Roshan et al 193 Table 1. Effect of Exercise Training and Curcumin on CK-MB, hs-CRP, LDL and MDA Levels, as Perilous Biomarkers in Lead-Induced Myocardial Injury in Rats (Mean + SEM for 7 Rats) Markers Groups Sham Lead Trainingþ lead Curcumin þ lead Curcuminþ trainingþ lead CK-MB (U/L) 58.23 + 86.31 + 67.95 + 65.00 + 57.45 + 1.73 3.56a 2.32a,b 1.01a,b 1.30b HS-CRP (mg/L) 0.0538 + 0.1571 + 0.0788 + 0.0571 + 0.0513 + 0.03 0.09a 0.03 0.04b 0.04b LDL (mg/dL) 36.57 + 53.85 + 35.28 + 39.28 + 30.85 + 10.62 15.90a 6.40b 10.43b 3.84b MDA (nmol/g) 26.82 46.08 34.41 35.82 30.36 + 2.85 + 9.22a + 15.07b + 6.49b + 12.53b Abbreviations: CK-MB, creatine kinase-MB; HS-CRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein; MDA, malondialdehyde. a Statistical significance P < .05 significantly different than sham group. b Statistical significance P < .05 significantly different than lead group. Immunoturbidimetric assay on a Hitachi 912 automated analyzer using reagents from Diasorin (Stillwater, Minnesota). The latex particles coated with antihuman CRP antibody aggregates with the tissue homogenate CRP, forming immune complexes. The formed immune complexes caused an increase in turbidity measured at 572 nm, which is proportional to the concentration of CRP in heart tissue. The high-sensitivity C-reactive protein concentration was determined from CRP standards of known concentration.11 Biochemical measurements on activity of the GPx enzyme was conducted using GPx-340 kit (OXIS, Portland, Oregon). Frozen samples of heart tissue were thawed, rinsed successively with 0.9% NaCl þ EDTA and with cold 20 mmol/L Tris-HCl, followed by homogenization. The homogenates were diluted with cold 20 mmol/L Tris-HCl and centrifuged (10 minutes at 5 C, 3000g). In the supernatants, activity of GPx was estimated by spectrophotometry. All samples to be statistically compared were processed in the same assay to avoid interassay variations. The concentration of lead was detected by means of atomic absorption spectrophotometry (AAS) method. Lipid peroxidation levels in the tissue homogenate were measured with the thiobarbituric-acid reaction using the method of Ohkawa et al.12 The quantification of thiobarbituric acid reactive substances was determined at 532 nm by comparing the absorption to a standard curve of MDA equivalents generated by acid catalyzed hydrolysis of 1, 1, 3, 3 tetramethoxypropane. The values of MDA were expressed as nmol/g tissue. Furthermore, serum CK-MB levels were measured by immunological DGKE method. Fasting serum high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) concentrations were measured by an enzymatic colorimetric method, as previously described by Ademuyiwa et al.13 The assay sensitivity for the 2 tests was 1 mg/dL. Serum TAC was measured using a commercially available kit (Randox Laboratories, Crumlin, UK) as previously described by Erel et al.14 In this method, the most potent radical, hydroxyl radical, is produced. First, a ferrous ion solution is mixed with hydrogen peroxide. The sequentially produced radicals such as the brown colored dianisidinyl radical cations, produced by the hydroxyl radical, are potent radicals. The antioxidative effect of the sample against the potent free radical reactions is then measured. The assay has excellent precision values, which are lower than 3%. The results are expressed in mmol/mL. In accordance with the protocol of Sheril et al we analyzed the lead acetate concentration using a spectrophotometer method only in the lead acetate group.4 Statistical Analysis Statistical analysis was performed using a commercial software package (SPSS version 16.0 for Windows). Results are expressed as means + SE. Data for hs-CRP, CK-MB, and oxidant/antioxidant markers were normally distributed after log-transformation. A 1-way analysis of variance (ANOVA) was used to detect statistical differences between groups. A post-hoc test (Tukey test) was performed to determine differences in the various markers between groups. The differences were considered significant at P < .05. Results Changes in CK-MB, hs-CRP, LDL, and MDA levels, as biomarkers in lead-induced myocardial injury of animals in each group, are shown in Table 1. Exposure to lead (20 mg/kg) caused an increase in the concentration of CK-MB, hs-CRP, LDL, and MDA by 48%, 192%, 47%, and 71%, respectively, in comparison to the sham group (all significantly increased P < .001, P < .05, P < .01, and P < .001, respectively). In contrast, curcumin, exercise training, and both interventions significantly reversed CK-MB, hs-CRP, LDL, and MDA levels (P < .001, P < .05, P < .01, P < .01, respectively). However, curcumin þ training þ lead treatment was more effective than curcumin þ lead and training þ lead alone treatment. Changes in the beneficial biomarkers in lead-induced myocardial injury, GPx and TAC, along with HDL in each group are shown in Table 2. The administration of lead at the concentration of 20 mg/kg for 8 weeks resulted in a decreases in GPx, TAC, and HDL levels by 43%, 27%, and 26%, respectively, in comparison to the sham group (P < .001, P < 0.01, and P < .01, respectively). Conversely, curcumin, exercise training, and their combination significantly increased GPx, TAC, and HDL levels (P < .001, P < .01, and P < .01, respectively). However, curcumin þ training þ lead treatment was more effective than curcumin þ lead and training þ lead alone treatment (Figure 1). Downloaded from ijt.sagepub.com at PENNSYLVANIA STATE UNIV on September 17, 2016 194 International Journal of Toxicology 30(2) Table 2. Effect of Exercise Training and Curcumin on GPx, TAC, and HDL Levels as Beneficial Biomarkers in Lead-Induced Myocardial Injury in Rats (Mean + SEM for 7 Rats) Markers Groups GPx (mm of GSH utilized/ mg protein) Sham Lead Trainingþ lead Curcuminþ lead Curcumin þ trainingþ lead 6.4700 3.6757 5.5412 6.2729 7.9500 TAC (mmol/mL) + 0.38 + 0.24a + 0.31a,b + 0.42b,c + 0.43a,b,c,d 385.75 + 279.85 + 411.75 + 411.71 + 450.37 + 8.89 14.33a 13.87a,b 14.37a,b 19.74a,b HDL (mg/dL) 28.85 + 21.14 + 30.28 + 32.57 + 36.14 + 10.18 5.66 8.95b 7.91b 6.17b Abbreviations: GPx, glutathione peroxidase; HDL, high-density lipoprotein. a Statistical significance P < .05 significantly different than sham group. b Statistical significance P < .05 significantly different than lead group. c Statistical significance P < .05 significantly different than training þ lead group. d Statistical significance P < .05 significantly different than curcumin þ lead group. Discussion The present study demonstrates the restorative potential of curcumin and exercise training by reversing lead-induced myocardial damage. Reductions in GPx, TAC, and HDL and increases in the concentration of hs-CRP, CK-MB, LDL, and MDA indicated deterioration of cardiac function and cellular damage due to the toxic effects of lead. Oxidative stress results in toxicity when the rate at which reactive oxygen species (ROS) are generated exceeds the scavenging capacity of the cell. Enhancement of MDA and reduction in GPx and TAC suggested oxidative damage in the heart muscle. Treatment by curcumin and exercise training restored lead-induced myocardial damage and tended to normalize biomarkers, suggesting a reversal of lead-induced cardiotoxicity, conforming the free radical scavenging property of curcumin (Tables 1 and 2). Lead, a commonly-used metal worldwide, has been used since ancient times. Studies have shown that lead has harmful effects on several tissues including the nervous system, blood, the cardiovascular system, and the reproductive and urinary systems.5 Recent studies suggest that one of the mechanisms by which lead can exert some of its toxic effects is through the disruption of the delicate prooxidant/antioxidant balance that exists within mammalian cells. In vivo studies have suggested that lead exposure is capable of generating ROS and thus alters antioxidant defense systems in animals.4 Thus, potential exists for biological mechanisms linking pollutants such as lead with cardiovascular disease through inflammation and oxidative stress.1 In the current study, hs-CRP and CK-MB were assayed as markers of inflammation and tissue damage in cardiac cells of rats treated with lead. Results of our investigation revealed a significant increase in the hs-CRP and CK-MB levels in the hearts of animals exposed to lead. This suggests that lead acetate had damaging effects on heart tissue during chronic exposure, which may heighten cardiovascular risk.5 The enzyme responsible for the decomposition of lipid peroxides is GPx. This enzyme protects cellular membranes from peroxidative damage.6 Glutathione peroxidase is a metalloprotein and accomplishes its antioxidant function by enzymatically detoxifying peroxides.2 Since this antioxidant enzyme depends on various essential trace elements for proper molecular structure and enzymatic activity, it is a potential target for lead toxicity.2,3,6 The presence of the free -SH group is necessary for the proper action of this antioxidant enzyme. Researchers have shown a decrease in the concentration of the free -SH groups in the blood as well as in the urine of the rats exposed to lead.2,6 The decrease in the activity of GPx in the heart and the increase in MDA concentration in the serum of the rats exposed to lead can be a result of this heavy metalinduced depletion in the free -SH groups noted in these animals.6 Several studies have shown that lead causes increased lipid peroxidation and decreased enzymatic and nonenzymatic antioxdants, which is in agreement with the observations in the current study.2,3,6 Our data indicate a protective effect of curcumin against cardiotoxicity. Antioxidant activity of curcumin was reported by Sharma as early as 1976.15 Curcumin is a known scavenger of free radicals and can significantly inhibit the generation of ROS such as superoxide anions, H2O2, and nitrite radical generation by activated macrophages, which play an important role in inflammation.16 When administered in the current study, curcumin effectively lowered the hs-CRP, CK-MB, MDA, and LDL levels after lead exposure, thus protecting cardiac tissues from inflammation, tissue damage, oxidative stress, and peroxidation lipids. Similarly, an enzymatic component of the defense system (GPx) was stimulated in the heart by curcumin, which is in accordance with earlier reports.7,17,18 Manikandan et al reported that curcumin treatment reduced levels of xanthine oxidase, superoxide anion, lipid peroxides, and myeloperoxidase while significantly increasing levels of superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), and glutathione-S-transferase (GST) in isoprenalineinduced myocardial ischemia in rats.17 Bharat et al reported that curcumin downregulated the expression of interleukin (IL)-6 protein, tumor necrosis factor (TNF), and various other chemokines, and inhibited the production of IL-8, MIP-1a, MCP-1, and IL-1a induced by inflammatory stimuli in human peripheral blood monocytes and alveolar macrophages. In Downloaded from ijt.sagepub.com at PENNSYLVANIA STATE UNIV on September 17, 2016 Dabidi Roshan et al 195 addition, curcumin downregulates the expression of the NF-kBregulated gene products such as COX-2, TNF, 5-LOX, IL-1, IL6, IL-8, MIP-1a, adhesion molecules, c-reactive protein (CRP), CXCR-4, and others.19 Thus, curcumin could suppress inflammation through multiple pathways. Sreejayan et al have suggested that the presence of phenolic groups in the structure of curcumin are fundamental to explaining its ability to eliminate oxygen-derived free radicals from the medium largely responsible for the peroxidation of cell lipids.20 The mechanism of protective curcumin is multifactorial, possibly including (1) its unique conjugated structure, which includes 2 methoxylated phenols and an enol form of b-diketone, a structure which shows typical radical-trapping ability as a chain-breaking antioxidant16,21; (2) prevention of lipid peroxidation and inhibition of ROS generation7; (3) the antioxidant property of curcumin decreases the utilization of vitamin C and vitamin E in the liver and thus maintains their level8; and (IV) interactions between curcumin, lead, and metal-curcumin complex (lead-curcumin); both the hydroxyl groups and the b-diketone moiety of curcumin are involved in metal-ligand complexation, either by directly bonding to the metal or by intermolecular hydrogen bonding.4 The current study suggests that supervised endurance training of 8 weeks can potentially produce a significant reduction in risk of cardiovascular events through decreases in leadinduced elevated levels of hs-CRP, CK-MB, MDA, and LDL, along with increases in GPx, TAC, and HDL levels. These results are consistent with those of Frederico et al who reported that 12 weeks of treadmill training increased antioxidant enzymes and decreased oxidative damage and injury in the myocardium through reducing MDA and elevated levels of CK-MB induced by isoproterenol.22 Researchers have reported chronic physical activity reduces hs-CRP levels by multiple mechanisms, including decreases in cytokine production by adipose tissue, skeletal muscles, endothelial and blood mononuclear cells, and possibly an antioxidant effect.23 Physical training reduces peripheral inflammatory markers associated with endothelial dysfunction, such as soluble intracellular and vascular adhesion molecules, granulocyte-macrophage colonystimulating factor, and macrophage chemoattractant protein-1 in patients with heart failure.24 Regular physical activity also improves endothelial function preserving nitric oxide availability.25 Although exercise acutely increases oxidative metabolism and thereby induces oxidative stress, there is evidence that long-term physical activity increases antioxidant defenses through the upregulation of antioxidant enzymes.26 Furthermore, this antioxidant effect of exercise reduces the susceptibility of LDL to oxidation, which in turn helps further prevent endothelial injury and inflammation.23 Powers et al reported that training resulted in large and significant increases in myocardial nonprotein thiols.27 As glutathione is known to be the dominant nonprotein thiol in cells, endurance training resulted in elevated levels of myocardial glutathione in the heart. Glutathione plays a pivotal role in the maintenance of intracellular redox status, antioxidant vitamin levels (ie, vitamins E and C), and the function of the antioxidant enzyme GPX. Because GPX requires a supply of reduced glutathione to remove organic hydroperoxides and hydrogen peroxide, it follows that a training-induced increase in myocardial glutathione should result in an improved capacity to remove these potentially injurious metabolites.27 Therefore, it seems that the training-induced increases in both myocardial enzymatic and nonenzymatic antioxidant systems are potential mechanisms to explain the training-induced reduction in myocardial injury.22,27 In summary, we observed that curcumin þ training þ lead treatment was more effective than curcumin þ lead and training þ lead alone, suggesting a potentially important training and curcumin interaction. However, there is a lack specific information with respect to their interaction effects. A large body of data exist which show that free radicals and ROS increase cardiovascular risk. Our findings indicate treatment with curcumin, as a strong antioxidant supplement, can decrease lipid peroxidation and myocardial damage. Moreover, curcumin improves total antioxidant capacity in the animal body. In the long term, regular endurance training could improve the antioxidant defense systems and injury in the myocardium induced by lead. Treatment with the combination of curcumin and training could markedly inhibit myocardial damage caused by lead in rats. Declaration of Conflicting Interests The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article. Funding The author(s) received no financial support for the research and/or authorship of this article. References 1. Chuang KJ, Chan CC, Su TC, Lee CT, Tang CS. The effect of urban air pollution on inflammation, oxidative stress, coagulation, and autonomic dysfunction in young adults. Am J Respir Crit Care Med. 2007;176(4):370-376. 2. Gurer H, Ercal N. Can antioxidants be beneficial in the treatment of lead poisoning? Free Radic Biol Med. 2000;29(10):927-945. 3. Patrick L. Lead Toxicity part II: the role of free radical damage and the use of antioxidants in the pathology and treatment of lead toxicity. Altern Med Rev. 2006;11(2):114-127. 4. Daniel S, Limson JL, Dairam A, Watkins GM, Daya S. Through mental binding, curcumin protects against lead- and cadmiuminduced lipid peroxidation in rat brain homogenates and against lead-induced tissue damage in rat brain. J Inorg Biochem. 2004; 98(2):266-275. 5. Gholamhosseini B, Khaki A, Khaki AA, Kachabi H, Radsaeed F. Ultra structure study of lead acetate cytotoxic effects on heart tissue in rabbit. Ofogh-e-Danesh. GMUHS Journal. (in Persian). 2009;14(4):5-12. 6. Kulikowska-Karpinska E, Moniuszko-Jakoniuk J. Lead and Zinc Influence on Antioxidant Enzyme Activity and Malondialdehyde Concentrations. Polish J Environ Stud. 2001;10(3):161-165. Downloaded from ijt.sagepub.com at PENNSYLVANIA STATE UNIV on September 17, 2016 196 International Journal of Toxicology 30(2) 7. Nazam Ansari M, Bhandari U, Pillai KK. Protective role of curcumin in myocardial oxidative damage induced by isoproterenol in rats. Hum Exp Toxicol. 2007;26(12):933-938. 8. Kalpana C, Shdheer AR, Rajasekharan KN, Menon VP. Comparative effects of curcumin and its synthetic analogue on tissue lipid peroxidation and antioxidant status during nicotine-induced toxicity. Singapore Med J. 2007;48(2):124-130. 9. Recep Aslan M, Ramazan Sekeroglu, Mehmet Tarakcioglu, Fahri Bayiroglu, Ismail Meral. Effect of acute and regular exercise on antioxidative enzymes, tissue damage markers and membran lipid peroxidation of erythrocytes in sedentary students. Tr J Med Sci. 1998;28(4):411-414. 10. Niessner A, Richter B, Penka M, et al. Endurance training reduces circulating inflammatory markers in persons at risk of coronary events: impact on plaque stabilization? Atherosclerosis. 2006; 186(1):160-165. 11. Jayachandran M, Okano H, Chatrath R, Owen WG, McConnell JP, Miller VM. Sex-Specific changes in platelet aggregation and secretion with sexual maturity in pigs. J Appl Physiol. 2004;97(4):1445-1452. 12. Ohkawa H, Ohishi N, Yagi K. Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal Biochem. 1979;95: 351-358. 13. Ademuyiwa O, Agarwal R, Chandra R, Behari JR. Lead-induced phospholipidosis and cholesterogenesis in rat tissues. Chem Biol Interact. 2009;179(2-3):314-320. 14. Erel O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin Biochem. 2004;37(4):277-285. 15. Sharma VP. Malaria and poverty in India. Curr Sci. 1976;84(4): 513-514. 16. Chattopadhyay I, Biswas K, Bandyopadhyay U, Banerjee RK. Turmeric and curcumin: Biological actions and medicinal applications. Curr Sci. 2004;87(1):44-53. 17. Manikandan P, Sumitra M, Aishwarya S, Manohar BM, Lokanadam B, Puvanakrishnan R. Curcumin modulates free 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. radical quenching in myocardial ischaemia in rats. Int J Biochem Cell Biol. 2004;36(10):1967-1980. Shmasara J, Ramezani M, Mohammadpour AH. Curcumin as a novel plaque stabilizing agent in prevention of acute coronary syndrome. Irn J Med Hypotheses Ideas. 2009;3(9):1-6. Aggarwal BB, Harikumar KB. Potential therapeutic effects of curcumin, the anti-inflammatory agent, against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases. Int J Biochem Cell Biol. 2009;41(1): 40-59. Sreejayan, Rao MN. Curcuminoids as potent inhibitors of lipid peroxidation. J Pharm Pharmacol. 1994;46(12):10131016. Dattani JJ, Rajput DK, Moid N, Highland HN, George LB, Desai KR. Ameliorative effect of curcumin on hepatotoxicity induced by chloroquine phosphate. Environ Toxicol Pharmacol. 2010;30(2):103-109. Frederico MJ, Justo SL, Da Luz G, et al. Exercise training provides cardioprotection via a reduction in reactive oxygen species in rats submitted to myocardial infarction induced by isoproterenol. Free Radic Res. 2009;43(10):957-964. Kasapis C, Thompson PD. The Effects of Physical Activity on Serum C-Reactive Protein and Inflammatory Markers. J Am Coll Cardiol. 2005;45(10):1563-1569. Adamopoulos S, Parissis J, Kroupis C, et al. Physical training reduces peripheral markers of inflammation in patients with chronic heart failure. Eur Heart J. 2001;22(9):791-797. Taddei S, Galetta F, Virdis A, et al. Physical activity prevents agerelated impairment in nitric oxide availability in elderly athletes. Circulation. 2000;101(25):2896-2901. Powers SK, Ji LL, Leeuwenburgh C. Exercise training-induced alterations in skeletal muscle antioxidant capacity: a brief review. Med Sci Sports Exerc. 1999;31(7):987-997. Powers SK, Demirel HA, Vincent HK, et al. Exercise training improves myocardial tolerance to in vivo ischemia-reperfusion in the rat. Am J Physiol. 1998;275(5pt2):1468-1477. Downloaded from ijt.sagepub.com at PENNSYLVANIA STATE UNIV on September 17, 2016