Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Compartmental models in epidemiology wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Breech birth wikipedia , lookup
Public health genomics wikipedia , lookup
HIV and pregnancy wikipedia , lookup
Epidemiology wikipedia , lookup
Birth control wikipedia , lookup
Prenatal development wikipedia , lookup
Prenatal testing wikipedia , lookup
Prenatal nutrition wikipedia , lookup
Maternal health wikipedia , lookup
Women's medicine in antiquity wikipedia , lookup
Multiple birth wikipedia , lookup
Maternal physiological changes in pregnancy wikipedia , lookup
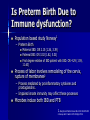
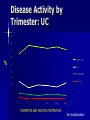
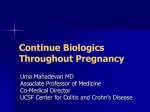
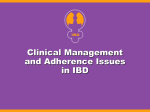
Management of Pregnant Women with IBD Uma Mahadevan MD Associate Professor of Medicine Co-Medical Director UCSF Center for Colitis and Crohn’s Disease Objectives Is fertility altered among patients with IBD? What adverse pregnancy outcomes are associated with IBD? What medications are compatible with use during pregnancy and lactation? What recommendations should be shared with the multidisciplinary team? Fertility and Pre-pregnancy Women with IBD have similar rates of conception to non-IBD women unless they have surgery Once pregnant, even with inactive disease, there is an increased risk of complications – Moderate to severe disease may make this worse Being in remission on low risk medication is the best option for a healthy pregnancy Healthcare maintenance up to date – Pap smears – Colonoscopy – Vaccinations THE PREGNANT PATIENT Pregnancy Outcomes: Population Based Studies IBD UC CD Preterm Birth X X XX LBW X SGA XX X 1. 2. 3. 4. Kornfeld et al. Am J Obstet Gynecol. 1997 (n=756 IBD) Fonager et al. Am J Gastroenterol. 1998 (n=510 CD) Norgard et al. Am J Gastroenterol. 2000 (n=1531 UC) Dominitz et al. Am J Gastroenterol. 2002 (n=107 UC, 155 CD) – Knight, no c Increase in Preterm birth with moderate to high disease activity LBW LBW at term Preterm birth Congenital Anomalies Crude Relative Risk 95% CI 1.1 0.3-4.0 0.9 0.1-8.5 3.4 1.1-10.6 0.4 0.0-3.9 Danish population based study: Pregnancies with disease activity at any time (n=71) were compared to pregnancies without any disease activity (n=86) Norgard B, et al. Am J Gastroenterol. 2007;102:1947–1954. IBD and Pregnancy: Overlapping Pathways Preterm birth (>37 wks gestation) – Leading cause of mortality in newborns – Higher rates CP, sensory deficits, learning disabilities, respiratory illness Animal models: During pregnancy, shift Th1:Th2 balance by placenta which produces Th2 cytokines (IL4) and progesterone. Nasef. Translational Research 2012;160:65-83 Cytokine spectrum in Pregnancy Early: dominant proinflammatory profile – Embryo invades and damages maternal uterus to implant Middle: – Decrease in proinflammatory cytokines. Mother, fetus, placenta in synchrony Late: – Increase in proinflammatory cytokines to activate parturition Is Preterm Birth Due to Immune dysfunction? Population based study Norway1 – Preterm Birth Maternal IBD: OR 2.15 (1.36, 3.39) Paternal IBD: OR 3.02 (1.82, 5.01) First degree relative of IBD patient with IBD: OR 4.29 (1.59, 11.63) Process of labor involves remodeling of the cervix, rupture of membranes2 – Process mediated by proinflammatory cytokines and prostaglandins. – Impaired innate immunity may affect these processes Microbes induce both IBD and PTB 1. Bengtson Inflamm Bowel Dis 2010:16:847-855 2. Savoye Am J Gastro:105:2010pp 473-4 Management of Flares Medication choices are similar – Avoid new aza/6mp in pregnancy – Avoid mnzl, CS in T1 Laboratory/Stool Tests – LFT’s (Alk Phos), ESR may be elevated – Albumin may be low; mild anemia normal – C. difficile Imaging – MRI preferred to CT, though no gadolinium in T1 – Ultrasound! Endoscopy: Unsedated flexible sigmoidoscopy Surgery: Indications similar to non-pregnant patient ; T2 best time Method of Delivery Delivery should be at the discretion of the obstetrician – Most women with IBD can have an uncomplicated vaginal delivery Exceptions: – Women with active perianal disease should have a cesarean section. Women with inactive perianal disease may deliver vaginally without increased complications (1) – Women with an ileoanal J pouch should consider cesarean section, though vaginal delivery is possible (2) Preserve sphincter function and continence later in life 1. Ilnyckyji A, Am J Gastroenterol 1999;94:3274-8 2. Juhasz ES, Dis Colon Rectum 1995;38:159-65. C-section and risk of IBD? CS delivery disturbs the normal bacterial colonization of the newborn's intestine Swedish Case-Control study 1536 cases – CS risk of pediatric CD among boys (OR = 1.25, 1.011.54) but not girls, (OR = 0.99, 95% CI 0.76-1.29) Danish Population Based study – 32.6 million person-yrs of follow-up CS increased risk of IBD at age 0-14 years (IRR 1.29, 95% CI 1.11-1.49) – Assuming causality, an estimated 3.2% of IBD cases before age 15 years were attributable to cesarean section. – Andersen: increase in IBD risk restricted nearly all to boys IRR=1.26 (1.15,1.37) vs. 1.06 (1.15 among girls) Higher for UC than CD 1. Decker Pediatrics 2010:125:e1433-40 2.Malmborg Inflamm Bowel Dis 2011 3.Bager Inflamm Bowel Dis. 2011 Jul 7. 4.Andersen Inflamm Bowel Dis 2012 Pelvic Floor Disorders Spontaneous vaginal birth vs. C section (n=1011) – Stress incontinence (OR 2.9, 1.5-5.5) – Prolapse to or beyond the hymen (OR 5.6, 95% CI 2.214.7) Operative vaginal birth significantly increased the odds for all pelvic floor disorders, especially prolapse – (OR 7.5, 95% CI 2.7-20.9). Forceps deliveries and perineal lacerations, but not episiotomies, were associated with pelvic floor disorders 5-10 years after a first delivery. Handa Obstet Gynecol. 2011 Oct;118(4):777-84 Handa Obstet Gynecol. 2012 Jan 5. Medication Use in Pregnancy Medication Safety Medication FDA Category Comment Lactation 5ASA Asacol, olsalazine B C Asacol: DBP Compatible (rare diarrhea) Corticosteroids Budesonide C C Low risk T1: Cleft palate Compatible Azathioprine/6MP D Low risk Compatible: Ideally wait 4 hours after dose Methotrexate Contraindicated Contraindicated X Azathioprine/6MP Swedish Medical Birth Register – 476 women used AZA in early pregnancy – Most common indication was IBD (>300) – Rate of CA 6.2% AZA vs. 4.7% other OR 1.41, 95% CI: 0.98-2.04 – Increased rate of VSD/ASD OR 3.18, 95% CI: 1.45-6.04 N=9 (4 SLE, 4 IBD, 1 nephrotic syndrome) – Increased rate of preterm, LBW, SGA Likely disease effect Coelho: Gut. 2011 Feb;60(2):198-203. Cleary. Birth Defects Research 85:647-654, 2009 Breastfeeding Breastfeeding (non-IBD moms) associated with a protective effect in the development of early onset IBD (1) Breastfeeding not associated with an increased risk of disease flare; possible protective effect against disease flare in the post-partum – Manitoba, population based study (2) 1. Barclay J Pediatr 2009 2. Moffatt Am J Gastro June 2009 Breast Feeding While Taking AZA/6MP 8 lactating women received Aza 75-200 QD – Milk and plasma at 30, 60 min and every hour x 5 Variation in bioavailability reflected in wide range in milk an plasma first 3 hours Major excretion in breast milk within 4 hours of drug intake Worst case scenario: max concentration 0.0075 mg/kg – In most cases, will be <10% of maximum concentration Christensen S et al. Aliment Pharmacol Ther. 2008:28, 1209-1213. Anti-TNF-alpha Therapies Infliximab Adalimumab Fab′ Certolizumab pegol Fab PEG IgG1 Fc Chimeric Human Monoclonal antibody PEGylated humanized Fab′ fragment 2 × 20 kDa PEG Adapted from: Hanauer SB. Rev Gastroenterol Disord. 2004;4(Suppl. 3):S18-S24. Anti-TNF’s: Safety Infliximab (B) – Katz: 100 infants exp, similar rate of live births, SAB’s – TREAT: 117 exp vs. unexposed with similar rate of miscarriage (10 vs. 6.7%) and neonatal complications (6.9% vs. 10%) Adalimumab (B) – 137 women enrolled in a prospective study in pregnancy and an additional 89 adalimumab exposed pregnant women in a registry. No increase in birth defects Certolizumab (B) data on file – 139 maternal exp pregnancies Natalizumab (C): IgG4 – 143 pregnant patients exposed to natalizumab – No birth defects reported Katz JA, et al. Am J Gastroenterol. 2004;99:2385; Lichtenstein. Gastroenterol 2010;138, S-475; Jurgens Inflamm Bowel Dis. 2009 Dec 21 ; Nazareth M, Mahadevan U. Am J Gastroenterol 2008;103:S449-50 Breastfeeding Infliximab Adalimumab Breastmilk 1/200th mother’s level (n=1)1 Peak concentrations in BM 100 ng/ml Induction therapy: (n=1) infant levels 1700 ng/ml (maternal level 78,300 ng/ml)3 Breastmilk 1/200th mother’s level(n=1)2 ADA undetectable in infant serum (n=1)3 Certolizumab Not detected in breastmilk (n=1) 1. Benhorin J Crohn’s Colitis 2011; Ben-Horin CGH 2010 3. Friitzsche J Clin Gastro 2012 Placental Transfer of IgG Ab INF and ADA are IgG1 antibodies Fc portion of IgG actively transported across placenta by specific neonatal FcR Highly efficient transfer in 3rd T leads to elevated levels of drug in newborn 20 B: Fetal r2=0.87, p<0.04 IgG (g/L) 15 10 5 0 0 10 20 30 40 50 Gestational age (weeks) Wiley-Blackwell Publishing Ltd. Malek A, Evolution of maternofetal transport of immunoglobulins During human pregnancy. Am J Reprod Immunol 1996; 36(5):248-55. Image Courtesy of Sundana Kane MD Maternal IgG and IgA are potentially available to the embryo as early as the 6th week of gestation (coelomic fluid) Maternal Ig present for the first 6 months of life to aid in fighting infection Placental Transfer Infliximab: – Study of 10 mothers on IFX – In all cases, infant and cord IFX level were greater than mother. 6 months to clear Adalimumab – Study of 10 mothers on ADA – In all cases, infant and cord ADA level was greater than mother. Up to 4 months to clear – ¾ pts who stopped ADA 35 days prior to delivery had a flare Certolizumab – Study of 10 mothers – In all cases, infant and cord levels were less than 2 mcg/ml even if mom dosed the week of delivery Mahadevan U Clin Gastro Hep 2012 epub ahead of print Placental Transfer: Another view 28 live births (17 IFX, 11 ADA) – Mean GA 39 [32-42] – Pts with active disease continued tx (5) – 10 pts on thiopurines, continued through pregnancy IFX: 12/17 d/c week 18-27 – 14 restarted (week 8-27) – 1 allergic rxn, 2 changed to ADA: 3/12 (25%) ADA: All 11 pts stopped week 22 – 2/11 relapsed – [18%] (CS wk 30; C section week 37) – all resumed therapy f/u 9 mos 22 % (5/23) had a flare or need to change therapy postpartum. – Account for preterm birth, continuing thiopurines, presence of detectable levels even when discontinued <30 weeks. Zelinkova Clin Gastro Hep Oct 2012 Infections Fatal case of disseminated BCG infection in an infant born to a mother on INF for Crohn’s disease – – – – – 10 mg/kg q 8 weeks monotherapy Healthy boy delivered 36 wks. No Breastfeeding Did well until 3 months when received BCG Failure to thrive, died at 4.5 months Post-mortem: disseminated BCG Cheet K J of Crohn’s Colitis 2010 PIANO: Pregnancy in Inflammatory Bowel Disease And Neonatal Outcomes Patients classified by exposure to four groups of drugs taken b/w conception and delivery: – Unexposed: no immunomodulators/biologics (mesalamine, steroids, antibiotics allowed) – Group A: AZA/6MP +/- Unexposed medications – Group B: INF, ADA, CZP +/- Unexposed medications – Group AB: Combination therapy +/- Unexposed medications Mahadevan Gastroenterology 2012 RESULTS Women Enrolled (4/25/2012) 1115 Pregnancies Ended •Still pregnant •Missing outcomes •Excluded/Withdrew 896 94 55 17/53 Unexposed •No medications 326 32 Group A (AZA/6MP) 204 Group B (Biologics) 291 Group AB (Combination) 75 Infliximab (+multiple exp) Adalimumab Certolizumab Natalizumab 193 104 37 5 (214) (126) (47) (6) Multiple Exposure: 27 •IFX/ADA (16) IFX/CZP (5) ADA/CZP (5) ADA/CZP/NAT (1) Disease Activity by Trimester: CD % TRIMESTER AND MONTHS POSTPARTUM Two hospitalizations Disease Activity by Trimester: UC % TRIMESTER AND MONTHS POSTPARTUM No hospitalization Adverse Pregnancy Outcomes Group A (aza) RR (CI) Group B (bio) Group AB (combo) Any Complication 0.98(0.69-1.40) 1.09 (0.80-1.48) 1.28 (0.82-1.98) Spontaneous Abortion 2.03 (0.74-5.55) 2.56 (1.07-6.12)* 1.29 (0.79-2.11) Preterm Birth 1.06 (0.62-1.81) 0.89 (0.54-1.47) 1.83 (1.01-3.31)* Low Birth Weight 0.69 (0.32-1.48) 1.17 (0.66-2.09) 1.05 (0.41-2.68) IUGR 0.96 (0.28-3.27) 1.01 (0.35-2.98) 1.25 (0.26-5.88) Cesarean section 1.07 (0.86-1.33) 1.23 (1.02-1.48)* 1.14 (0.86-1.53) NICU 1.09 (0.66-1.81) 1.20 (0.77-1.88) 1.71 (0.96-3.07) Congenital Anom 1.05 (0.50-2.21) 1.07 (0.55-2.08) 1.36 (0.52-3.56) Adjusted for none/mild vs. mod/severe disease activity * P <0.05 Timing of biologics Debate: stop drug early or continue scheduled? – Last dose infliximab at week 32 weeks gestation No real delay if patient gets next dose immediately after delivery (assume delivery around week 40 gestation) – Last dose adalimumab at week 36-38 Stopping earlier may lead to flares If needed, can continue throughout on schedule – Continue certolizumab throughout pregnancy – If mom flares, treat her! – No live virus vaccine for first 6 months for infants exposed to IFX or ADA during pregnancy – Never switch drugs during pregnancy purely for placental transfer issues Mahadevan U. Am J Gastroenterol. 2011 Feb;106(2):214-23 Communicate with Interdisciplinary team Obstetrician: – Most IBD medications are low risk in pregnancy (exception methotrexate) and can be continued during pregnancy and lactation – Mode of delivery is per OB discretion except with active perianal disease at the time of delivery and perhaps J Pouch Pediatrician – No live virus vaccines in the first 6 months if infant exposed to infliximab or adalimumab in utero – All other vaccines can be given on schedule – Monitor for infections