Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
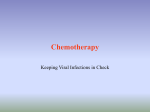
Clinical Science (1996) 91, 201-208 (Printed in Great Britain) 20 I Poincare plot of heart rate variability allows quantitative display of parasympathetic nervous activity in humans Peter Walter KAMEN, Henry KRUM* and Andrew Maxwell TONKIN Departments of Cardiology and *Clinical Pharmacology, Austin and Repatriation Medical Centre (Austin Campus), Melbourne, Australia (Received 24 October 1995/2 April 1996; accepted II April 1996) 1. Time domain summary statistics and frequency domain parameters can be used to measure heart rate variability. More recently, qualitative methods including the Poincarb plot have been used to evaluate heart rate variability. The aim of this study was to validate a novel method of quantitative analysis of the PoincarC plot using conventional statistical techniques. 2. Beat-to-beat heart rate variability was measured over a relatively short period of time (1&20 min) in 12 healthy subjects aged between 20 and 40 years (mean 30 f 7 years) during (i) supine rest, (ii) head-up tilt (sympathetic activation, parasympathetic nervous system activity withdrawal), (iii) intravenous infusion of atropine (parasympathetic nervous system activity withdrawal), and (iv) after overnight administration of low-dose transdermal scopolamine (parasympathetic nervous system augmentation). 3. The ‘width’ of the PoincarC plot, as quantified by SD delta R-R (the difference between successive R-R intervals), was determined at rest (median 48.9, quartile range 20ms) and found to be significantly reduced during tilt (median 19.1, quartile range 13.7 ms, P< 0.01) and atropine administration (median 7.1, quartile range 5.7ms, P<O.Ol) and increased by scopolamine (median 79.3, quartile range 33 ms, P< 0.01). Furthermore, log variance of delta R-R intervals correlated almost perfectly with log high-frequency (0.15-0.4Hz) power (r=0.99, P< 0.01). 4. These findings strongly suggest that the ‘width’ of the PoincarC plot is a measure of parasympathetic nervous system activity. The Poincarb plot is therefore a quantitative visual tool which can be applied to the analysis of R-R interval data gathered over relatively short time periods. INTRODUCTION Sympathetic-parasympathetic interactions have been well studied and their importance established in a number of cardiovascular diseases. Such situations include patients after myocardial infarction [l], patients at risk of sudden cardiac death [2, 31 and patients with heart failure [4,51, in all of which increased sympathetic and decreased parasympathetic nervous system activity is common. Various methods have been used to attempt to quantify these autonomic influences. Recently, there has been considerable interest in the measurement of heart rate variability (HRV) as one such approach and a number of time and frequency domain indices have been used to quantify this [6]. Another new method of HRV analysis is the PoincarC plot, which is a ‘scatterplot’ (return map) of current cardiac cycle length (the R-R interval on the ECG) against the preceding R-R interval [7]. The PoincarC plot allows a real time display of interbeat intervals at the time the patient is being monitored and can thus provide a visual measure of parasympathetic nervous system activity. In addition, this method permits immediate recognition of ectopic beats [S, 91 or artefact which may otherwise go unobserved [lo, 111. We have developed a method of quantifying the Poincart plot which is an extension of a method developed by Malik et al. [l2] who used the width of the main peak of the frequency distribution curve to quantify noisy HRV time series. Our technique of quantifying the pattern of the PoincarC plot uses statistical measures of variance of both R-R and delta R-R histograms. These may provide more robust measures of HRV in the presence of a low level of beat recognition error and recording artefact than more conventional techniques [12). In this study we sought to validate this new approach to quantitative assessment of the PoincarC plot by analysis in healthy subjects of the effects of standard perturbations of autonomic function. Moreover, we tried to simplify the assessment of HRV by collecting R-R interval data over a relatively short time (10-2Omin). Most recent research has used HRV data acquired over a 24h period during prolonged ambulatory (‘Holter’) monitoring of the ECG. This approach has attendant logistic problems including non-stationarity of the HRV time series. Key Words: autonomic nervous system, heart rate variability, parasympathetic nervous system, Poincark plot. Abbreviations: HF, high frequency; HRV, heart rate variability; LF, low frequency; rMSSD, root mean-squared successive difference. Correspondence: Dr Peter W. Kamen, Department of Cardiology, ARMC (Austin Campus), Heidelberg, Victoria 3084, Australia. P. W. Kamen et al. 202 METHODS . . 14004 Subjects Twelve healthy subjects (seven males and five females) aged between 20 and 40 years (mean 30.2 i-7.2) years were studied. Subjects were included in the study if they were in sinus rhythm, did not smoke, had no known cardiovascular abnormalities and were not taking any medications. All had provided fully informed consent. Ethical approval was granted by the Austin Hospital Committee of Ethics in Human Research. f 6001 4001 200 artefact I , , ,”: ,;; artefact , , 200 400 600 800 1000 I200 R-R, interval (ms) 200 400 600 800 I , , 1400 1600 1400 1600 Study design Study subjects were instructed to have a light breakfast and not consume alcohol or caffeinated beverages for 12h before the study. All studies were performed at the same time of day with the subjects breathing spontaneously and remaining undisturbed in a quiet, temperature-controlled room. Although respiratory rate and amplitude are important modulators of HRV [13] we did not control respiration in our subjects because all phases of the study were conducted in the resting state where respiration frequency and amplitude should remain essentially unchanged and within the range of 16-18 breaths per min. An intravenous cannula was inserted into an antecubital vein and subjects then rested for 20 min before commencement of data collection. A total of 1024 data points (R-R intervals) were collected for each study segment and used to generate the PoincarC plot. Accordingly, data epochs varied from approximately 10 to 20min. The following sequential protocol of autonomic perturbations was performed. At least 20 min was allowed between each phase of the study to permit the return of heart rate to baseline. The study phases were not randomized. Baseline study. All baseline studies were conducted in subjects in the post-absorptive state after resting for 10min in the supine position in a quiet environment. Seventy degree head-up tilt. Subjects were tilted to 70” on a motorized table until 1024 data points were collected. This manoeuvre increases sympathetic and decreases parasympathetic nervous system activity [14, 151. Collection of HRV data commenced after 5min of tilt to permit the heart rate to stabilize in the new position. Atropine infusion. Atropine sulphate, 1.2mg, was added to 50ml of 5% intravenous dextrose and infused at a rate of 0.12 mg/min for 5 min and then at a rate of 0.024mg/min until completion of this phase of the study. This dose regimen markedly decreases parasympathetic nervous system activity [16]. Data collection began 10 min after commencement of the infusion. Transdermal scopolamine. A low-dose transdermal scopolamine patch (hyoscine 1.5 mg) was applied : : y 200 1000 1200 R-R, interval (ms) Fig 1. PoincarC plots. (a) Poincare plot before filtering of ‘noisy’ R-R interval data showing a ’central cluster’ with outlying data points due to artefact. (b) Poincare plot after ‘adequate’ filtering. The ‘central cluster’ has been preserved and the outlying data points have been removed. overnight to an undamaged hair-free area of skin behind the ear 1 week after the above studies. The patch remained in situ for the duration of this period of the study. Low-dose transdermal scopolamine increases parasympathetic nervous activity ~171. Data acquisition R-R intervals were collected using an AMLAB data acquisition workstation (Associative Measurements, Sydney) with a program that triggers on the leading edge of the R-wave of the ECG. The analogue ECG signal was digitized at a sampling rate of 2kHz. The system was calibrated on a digital and analogue pulse generator to an accuracy of + l m s and found to measure R-R intervals to within k l m s . The Poincark plot and tachogram were constructed on line using raw data and examined for artefact and ectopic activity. Technical aspects of the Poincar6 plot The PoincarC plot is a ‘scatterplot’ (or ‘return map’) of the current R-R interval against the R-R interval immediately preceding it, as illustrated in Fig. 1. Poincare plot and autonomic perturbations The Poincark plot can provide a display of overall as well as beat-to-beat variability [181. This is because HRV is graphically displayed as a pattern of points which lends itself to visual analysis more readily than summary statistical measures such as the root mean-squared successive difference (r-MSSD). Histograms of R-R intervals and delta R-R intervals can be quantified by the analysis of variance of the respective data [4]. The SD of the R-R interval histogram relates to the variance of the data of the Poincark plot projected onto the x-axis. The delta R-R interval is the difference between successive RR intervals. Thus the SD delta R-R can be used to quantify the ‘width‘ of the Poincark plot as it relates to the variance of the distribution of data points around the line of identity. Mathematical details are given in the Appendix. Filtering technique Artefact and occasional ectopic beats occur in almost all HRV studies [12]. To reduce the effect of such ‘noise’, filters can be used to remove selected portions of the R-R interval data. We identified artefact or ectopic beats from the original ECG and related them to the pattern of distribution of points on the Poincark plot [8] as illustrated in Fig l(a). The outlying points were then replaced with interpolative R-R interval data using a cubic spline algorithm 119, 201 (Software for Science, Engineering and Industry for Microsoft Quickbasic 4.xIPCQB-006 Version 7; Quinn-Curtiss, Needham, MA, USA.). We then examined the filtered Poincark plot for evidence of distortion of the pattern induced by excessive filtering and for possible persistence of outlying points due to inadequate filtering. Figure 1 (b) illustrates the effect of filtering on the Poincark plot. Power spectral analysis The time series was created as a function of heartbeats and the resulting interval tachogram is thus a series of R-R intervals plotted as a function of the interval number, as detailed by De Boer et al. [21]. Since the interval tachogram is a function of the interval number rather than time, when used to compute the fast Fourier transformation the result in the abscissa is expressed in cycles per interval rather than Hz. When the total variability is small in comparison with the mean heart rate, only a small error arises and the calculated interval spectrum is considered as a true frequency spectrum. The spectral units must then be divided by the mean R-R interval in order to obtain a result expressed in Hz. After detrending and filtering the raw R-R interval data, an IBM PC 486 with a commercial software package (Software for Science, Engineering and Industry for Microsoft Quickbasic 4.xIPC-QB-006 Version 7; Quinn-Curtiss) was used 203 to compute the fast Fourier transformation. Power spectral measures of R-R variability were then computed by integrating over their frequency intervals. Two main components of the power spectra of HRV were identified: a high-frequency (HF) component (from 0.15 to 0.4Hz) and a low-frequency (LF) component (from 0.01 to 0.15Hz). The total power (from 0.01 to 0.4Hz) was also calculated. Statistics Variables with a normal distribution (age, heart rate) are presented as mean+SD and skewed data are expressed as median and quartile range (the value of the 75th percentile minus the value of the 25th percentile) where 50% of the data points fall within this range. We used the non-parametric Friedman repeated-measures analysis of variance on ranks as all HRV variables showed a skewed distribution. Consequently, Pearson’s correlation coefficient and the corresponding tests of significance were used to assess the relation between logtransformed frequency and time domain variables. R-R interval histograms were assessed for normality by the Kolmogorov-Smirnov method. A two-tailed P < 0.05 was considered significant. RESULTS Results are summarized in Table 1. HRV in the baseline study The Poincark plot of all subiects displayed a clustering of data-points as illustiated in Fig. 2(a), characterized by SDR-R of 55-142ms, median 69.3 (19.4)ms and SD delta R-R of 27-123ms, median 48.9 (20)ms. HRV during head-up tilt All subjects displayed a marked reduction in variance of delta R-R intervals compared with baseline, as illustrated in Fig. 2(b). Heart rate increased significantly during tilting from 60.9 & 9.7 to 80.9f 12.4 beats/min P<O.OOOl). The SDRR decreased by 22% to 54.4 (24.1)ms (P<O.Ol), but the coefficient of variation of R-R intervals remained unchanged compared with baseline values. The SD delta R-R and coefficient of variation of delta R-R intervals between baseline and tilt were reduced by 61% and 51% respectively (P<O.Ol for both). Considering analyses in the frequency domain, LF, H F and total power decreased by 31%, 82% and 39% respectively (all P <0.05). P. W. Kamen et al. 204 Table 1. Heart rate and HRV parameters from subjects exposed to various autonomic perturbations. All values are presented as median (quartile range). Abbreviations: Coeff, coefficient of variation; HF, high-frequency power; LF, low-frequency power; pNN50, proportion of R-R intervals more than 50ms different; NS. not significant. Statistical significance: *P < 0.05, **P < 0.01, Heart rate variability Time domain SDR-R (mr) Coeff R-R SDAR-R (ms) Coeff AR-R pNN50 SDR-R/SDAR-R Frequency domain LF (msl) HF (mrl) Total power (rnsl) Baseline 70” tilt Atropine Scopolamine 69.3 (19.4) 7.6 (1.3) 48.9 (10) 5.3(2.5) 19.1 (21.8) I .34 (0.3) 54.4 (24. I)** 7.3 (2.2) (NS) 19.1 (13.7)** 1.6 (I .5)** I .8 (6.5)** 1.61 (I .O)** 33.6 (8.6)** 4.3 (1.3)** 7.1 (5.7)** I .I (0.7)** 0.5 (0.3)** 5.4 (l.l)** 90.7 (35.3)** 8. I (I.8) (NS) 79.3 (33.0)** 7.6 (1.7)** 48.6 (20)** 1.1 (0.1) (NS) 858 (695) 303 (412) 1056 (961) 588 (703)* 54 (91)* 641 (8l8)* 142 (150)** 5.0 (7.3)* 147 (IS)** 1477 (134l)(NS) 685 (734)* 2287 (2160)* HRV during atropine infusion Heart rate increased significantly in all subjects, from 60.9 & 9.7 to 83.6 f9.4 beats/min (P < 0.01). Atropine administration resulted in a 57% reduction in SDRR to 33.6 (8.6)ms and an 87% reduction in SD delta R-R to 7.1 (5.7)ms ( P ~ 0 . 0 1for both) compared with baseline measurements. These changes were associated with a marked reduction in ‘width’ of the Poincark plot, as illustrated in Fig. 2(c). The reductions in coefficient of variation of RR and delta R-R intervals were also highly significant (P t0.01). Both LF and H F power decreased; LF power from 858 (695) to 142 (150)ms’ (P<O.Ol) and H F power from 303 (412) to 5.0 (7.3)ms2 (P<0.05). and increases with scopolamine, consistent with changes in parasympathetic activity. Correlations between time and frequency domain parameters Using all the HRV data, we found an almost perfect correlation between log H F power and log variance of delta R-R intervals (r=0.99, P<O.OOOl). This is illustrated in Fig. 3. Log total power was also strongly correlated with both log variance of R-R (r=0.98, P<O.OOOl) and delta R-R intervals ( r =0.95, P <0.0001). This has been reported previously [22, 231 and is supportive of experimental evidence for the mathematical relationship between time and frequency domain HRV parameters as described by Parseval’s theorem. Details appear in the Appendix. HRV during lowdose transdermal scopolamine The scopolamine patch was well tolerated by all patients, none of whom voluntarily reported adverse side effects such as dry mouth or drowsiness. The reduction in heart rate from the baseline value of 60.5k9.7 to 56.7k8.3 beats/min was not statistically significant, possibly because of the small sample size. SDR-R increased by 31% (P<O.Ol) and SD delta R-R increased by 62% (P<O.Ol) with transdermal scopolamine. This was reflected by a marked increase in the ‘width’ of the Poincare plot, as illustrated in Fig. 2(4. The coefficient of variation of delta R-R intervals increased by 43% (P<O.Ol), indicating that the increase in HRV was not simply due to the reduction in heart rate. Analysis of the effect of transdermal scopolamine on measures in the frequency domain paralleled effects of the drug on time domain parameters. High-frequency power increased by 126% (P <0.05), consistent with an increase in parasympathetic nervous system activity. In summary, the results show that the ‘width‘ of the Poincart plot, as quantified by SD delta R-R, decreases from baseline with tilting and atropine DISCUSSlON Time series methodologies applied to the analysis of HRV have mainly been standard time [24] and frequency [25] domain techniques. The potential for use of serial correlation techniques [26, 271 has not been fully explored. The present study strongly suggests that short-term analysis of HRV using the Poincark plot and related histograms provides an accurate method with which to quantify autonomic activity. We have demonstrated that the ‘cluster’ Poincark pattern can be quantified with conventional statistical methods that correlate closely with time and frequency domain parameters used to quantify parasympathetic nervous system activity in healthy subjects [lS, 16, 281. More complex, nonlinear mathematical methods may be necessary to accurately quantify other pattern types seen in patients with cardiac disease [4, 291. Bigger et al. [22] have previously shown a strong correlation between H F power and the r-MSSD of normal R-R intervals. Although SD delta R-R is mathematically equivalent to r-MSSD (see Appendix), only the delta R-R interval can be used to Poincare plot and autonomic perturbations // 500 1W 205 1500 R-R, interval (ms) 0 Q / 9s % / ‘ D *4 ’*., 9@ % % Q A M interval R-R interval (ms) R-R interval histogram histogram AR-R interval histogram */ / R-R. interval (ms) O 600 800 loo0 I200 1400 R-R interval histogram 1500, I 500 MO 1000 R-R, interval (ins) 80 60 40 20 AR-R interval histogram 0 R-R interval histogram histogram R-R interval histogram Fig. 1. Characteristic Poincar6 plots generated by a 36year old female during various phases of the study. (a) Baseline study. The SDs of R-R (SDR-R) and AR-R (SDAR-R) intervals were 71 and 50ms respectively. (b) Head-up tilt. The SDR-R and SDAR-R were 50 and I I ms respectively. (c) Atropine infusion. The SDR-R and SDAR-R were 34 and lOms respectively. (d) Transdermal scopolamine. The SDR-R and SDAR-R were 81 and 71 ms respectively. construct a histogram which relates to the Poincart plot (all r-MSSD values are positive). Therefore, we have used S D delta R-R as a measure of the ‘spread‘ of the delta R-R interval histogram and have proposed this parameter as a method by which to quantify parasympathetic nervous system activity during these perturbations. We have also demonstrated a strong correlation between frequency and time domain measures used to quantify HRV. Total power was strongly correlated with SDR-R and SD delta R-R. The total power of spectral energy has been proposed to represent both sympathetic and parasympathetic activity, while H F power is accepted as a measure of pure parasympathetic activity [30]. Therefore, it is suggested that the ‘width’ of the Poincart plot as quantified by SD delta R-R represents a pure measure of parasympathetic activity. The use of this method also allows immediate recognition of ectopics or artefact which may go unobserved and corrupt HRV data if conventional analytical methods are used [111. We have used the Poincark plot to guide filtering algorithms to completely remove ectopic beats and artefact from the time series data without corrupting the normal sinus rhythm. Poincark plot analysis is an extension of a method developed by Malik et al. [12] who used the width of the main peak of the frequency distribution curve to quantify noise HRV time series. Although the analysis of histograms using the Malik P. W. Kamen et al. 206 2 4 6 8 Log variance AR-R interval (ms’) 10 Fig. 3. Relation between time and frequency domain variables. Log HF power (O.IM.4Hz) correlated strongly with log variance of AR-R intervals. algorithm provides the same statistical result as the Poincart plot technique we have found that the visual information provided by the latter method augments the simple statistical analysis of histograms. Furthermore, other methods for analysis of Poincart plot patterns may demonstrate non-linear relationships [31] between sympathetic and parasympathetic nervous activity [32-341 which would otherwise go unrecognized. Therefore the PoincarC plot provides additional information to complement current methods of HRV analysis and is a useful adjunct, especially in the clinical setting where ‘real time’ analysis of HRV is of critical importance. In contrast to most, but not all [35] studies of HRV which have relied on data collected during prolonged ambulatory monitoring of the ECG, our patients rested quietly with data collected over a relatively short time span of 10-20mins. This may account for the finding that our healthy subjects did not display Poincart plot patterns with the characteristic ‘comet’ and ‘stem’ shape seen in data from healthy subjects in the study of Woo et al. [7] who employed 24 h ambulatory monitoring. The small ‘head’ of their ‘comet’ pattern was probably the result of increased sympathetic and decreased parasympathetic activity leading to an increase in absolute heart rate and associated reduction in HRV. Significance and potential applications Analysis of HRV based on short-term analysis of the PoincarC plot provides a sensitive, non-invasive measurement of autonomic input to the heart. Heart rate variability can be measured in both the time and frequency domain, and in the present study, time and frequency domain variables have been shown to correlate very highly. Time domain indices used to quantify the PoincarC plot have been shown to be nearly equivalent to their respective frequency domain variables. The technique described could therefore greatly simplify HRV analysis. Bigger et al. [35] have demonstrated that power spectral measures of R-R variability calculated from short (2-1 5 min) electrocardiographic recordings are remarkably similar to those calculated over 24 h. If so, short-term HRV analyses based on the Poincark plot should be as predictive of prognosis as 24h measures of HRV. In summary, the present study has demonstrated that the PoincarC plot is a simple, yet powerful adjunct to conventional HRV analytical techniques. It provides complementary information to other standard procedures such as statistical (time domain) measures, the tachogram, histogram and frequency (power spectrum) analysis. ACKNOWLEDGMENT We thank AMRAD Operations Pty Ltd and National Mutual Life Association for their support of this work. REFERENCES I. Stramba-Badiale M, Vanoli E, De Ferrari GM, Cerati D, Foreman RD, Schwartz PJ. Sympathetic-parasympathetic interaction and accentuated antagonism in conscious dogs. Am J Physiol 1991; 260: H335-40. 2. Corr PB, Pitt B, Natelson BH, Reis DJ, Shine KI, Skinner JE. Sudden cardiac death. Neurakhemical interactions. Circulation 1987; 76 (Suppl. I): 1-208-14. 3. Schwartz PJ, La Rovere MT, Vanoli E. Autonomic nervous system and sudden cardiac death. Experimental basis and clinical observations for post-myocardial infarction risk stratification. Circulation 1992; 8 5 177-91. 4. Kamen PW, Tonkin AM. Application of the Poincare plot t o heart rate variability: a new measure of functional status in heart failure. Aust N Z Med 1995; 2 5 1&26. 5. Adamopoulos 5, Piepoli M, McCance A, et al. Comparison of different methods for assessing sympathovagal balance in chronic congestive heart failure secondary t o coronary artery disease. Am J Cardiol 1992; 70 157682. 6. Kienzle MG, Ferguson DW, Birkett CL, Myers GA, Berg WJ, Mariano DJ. Clinical, hemodynamic and sympathetic neural correlates of heart rate variability in congestive heart failure. Am J Cardiol 1992; 69: 761-7. 7. Woo MA, Stevenson WG, Moser DK. Trelease RB. Harper RM. Patterns of beat-to-beat heart rate variability in advanced heart failure. Am Heart J 1992; lU: 704-10. 8. Anan T, Sunagawa K, Araki H, Nakamura M. Arrhythmia analysis by successive RR plotting. J Electrocardiol 1990; U: 243-8. 9. Woo MA, Stevenson WG, Moser DK, Middlekauff HR. Complex heart rate variability and serum norepinephrine levels in patients with advanced heart failure. J Am Coil Cardiol 1994; U.565-9. 10. Kamen PW, Tonkin AM. Heart rate Poincare plots in heart failure: reply. Aust N 2 J Med 1995; 25 (4): 372-3. I I. Myers G, Workman M, Birkett C, Ferguson D, Kienzle M. Problems in measuring heart rate variability of patients with congestive heart failure. J Electrocardiol 1992; 25. 214-19. 12. Malik M, Farrell T, Cripps T, Camm A]. Heart rate variability in relation t o prognosis after myocardial infarction: selection of optimal processing techniques. Eur Heart J 1989 10 1060-74. 13. Novak V, Novak P, de Champlain J. Le Blanc AR. Martin R, Nadeau R. Influence of respiration on heart rate and blood pressure fluctuations. J Appl Physiol 1993; 74: 617-26. 14. Butler GC, Yamamoto Y, Xing HC, Northey DR, Hughson RL. Heart rate variability and fractal dimension during orthostatic challenges. J Appl Physiol 1993; 75 ZMI2-12. 15. Vybiral T, Bryg RJ, Maddens ME, Boden WE. Effect of passive tilt on sympath etic and parasympathetic components of heart rate variability in normal sub jects. Am J Cardiol 1989; 63: I117-20. 16. Hayano J,Sakakibara Y, Yamada A, e t al. Accuracy of assessment of cardiac vagal tone by heart rate variability in normal subjects. Am J Cardiol 1991; 67: 199-204. 17. La Rovere MT, Mortara A, Pantaleo P, Maestri R, Cobelli F, Tavazzi L. Scopolamine improves autonomic balance in advanced congestive heart failure. Circulation 1994; 90 (2): 83B-43. 207 Poincare plot and autonomic perturbations 18. Raetz SL, Richard CA, Garfinkel A, Harper RM. Dynamic characteristics of cardiac R-R intervals during sleep and waking states. Sleep 1991; 14 526-33. 19. Rompelman 0, Coenen AJ, Kitney RI. Measurement of heart-rate variability: Part I-Comparative study of heart-rate variability analysis methods. Med Biol Eng Comput 1977; IS:233-9. 20. Albrecht P, Cohen RJ. Estimation of heart rate power spectrum bands from real world data: dealing with ectopic beats and noisy data. Comp Cardiol. L a Alamitos, CA, U.S.A.: IEEE Computer Society Press, 1988 31 1-14. 21. De Boer RW, Karemaker J. Strackee J. Comparing spectra of a series of point events particularly for heart rate variability data. IEEE Trans Biomed Eng 1984; where R-R, corresponds to the x-coordinate and R-R, + to the y-coordinate. Delta R-R interval The delta R-R interval (AR-R) is defined as 31: 3B4-7. 22. Bigger Jr JT, Albrecht P, Steinman RC, Rolnitzky LM. Fleiss JL, Cohen RJ. Comparison of time- and frequency domain-based measures of cardiac parasympathetic activity in Holter recordings after myocardial infarction. Am J Cardiol 1989; 64. 536-8. 23. Bigger Jr IT, Fleiss JL, Steinman RC, Rolnitzky LM, Kleiger RE, Rottman JN. Correlations among time and frequency domain measures of heart period variability two weeks after acute myocardial infarction. Am J Cardiol 1992; 6 9 891-8. 24. Box GEP, Jenkins GM. Time series analysis: forecasting and control. San Francisco, U.S.A.: Holden-Day, 1970. 25. Bloomfield P. Fourier analysis of time series: an introduction. New York John Wiley, 1976. 26. Pincus SM. Greater signal regularity may indicate increased system isolation. Math Biosci 1994; 122 (2): 161-81. 27. Cox DR. Lewis PAW. The statistical analysis of series of events. London: Chapman and Hall, 1966. 28. Jaffe RS, Fung DL, Behrman KH. Optimal frequency ranges for extracting information on autonomic activity from the heart rate spectrogram. J Auton Nerv Syst 1994; 46: 37-46. 29. Kamen PW, Tonkin AM. Chaos mathematics enables quantitative assessment of heart rate variability in patients with cardiac failure. [Abstract] Aust N Z Med 1993; 2 3 595. 30. Pomeranz 8, Macaulay RIB, Caudill MA, et al. Assessment of autonomic function in humans by heart rate spectral analysis. Am J Physiol 1985; 248: H151-3. 31. Glass L, Kaplan DT. Time series analysis of complex dynamics in physiology and medicine. Med Prog Techno1 1993; I9 115-28. 32. Woo MS, Woo MA, Gozal D, Jansen MT, Keens TG, Harper RM. Heart rate variability in congenital central hypoventilation syndrome. Pediatr Res 1992; 31: 291-6. 33. Garfinkel A. Raetz SL, Harper RM. Heart rate dynamics after acute cocaine administration. J Cardiovasc Pharmacol 1992; I9 453-9. 34. Schechtman VL, Raetz SL, Harper RK, et al. Dynamic analysis of cardiac R-R intervals in normal infants and in infants who subsequently succumbed to the sudden infant death syndrome. Pediatr Res 1992; 31: 606-12. 35. Bigger JrIT, Fleiss JL, Rolnitzky LM, Steinman RC. The ability of several short-term measures of RR variability t o predict mortality after myocardial infarction. Circulation 1993; 88: 927-34. APPENDIX Geometrical interpretation of R-R interval histogram The relationship between the histogram of R-R intervals and the corresponding PoincarC plot can best be illustrated using geometric concepts and techniques. We make the assumption that the xand y-axes are scaled identically. We consider first the time series XN X, = AR-R, R-R, - R-R, +1 If it is assumed that the PoincarC plot has a symmetric distribution about its mean, then the AR-R interval distribution has zero mean A R-R interval histogram The AR-R interval histogram is a frequency distribution graph which includes both negative and 920 980 940 960 980 1 I000 IOW /’ I i 9001” I 900 920 ’ I ’ I 940 960 R-R, interval (ms) ’ I 980 ’ + 1, R-R, + 2, Fig. 4. Geometric relationship between the AR-R interval and data points on the PoincarC plot. Point A is the point with coordinates (R-R,, R-R,+J, while points B and C lie on the line of identity. The AR-R interval is quantified by the distance AC. The ‘width’ of the Poincare plot is derived from the length of AB. a=454 positive values and is centred around zero (mean = 0) with variance measured by SDAR-R. SD of AR-R intervals is given by ...,R-RN) which is equivalent to the r-MSSD given by Each datapoint on the PoincarC plot corresponds to the ordered pair. r-MSSD = Datapoint, =(R-R,, R-R,+ ,) I 900 1000 SDAR-R = (R-R,, R-RZ, ...,R-R,, R-R, 920 (R-R, - R-R, + 1)2 P. W. Kamen et al. 208 SDAR-R and r-MSSD are mathematically equivalent if AR-R=0, but only the former is a measure of SD of the AR-R histogram which relates to the ‘width’ of the Poincare plot. Geometrical interpretation of the AR-R interval histogram (where a = 45”). A ‘width’ histogram can be constructed from the transformed data which can then be tested for normality by the Kolmogorov-Smirnov method. If the ‘width’ histogram is Gaussian, then the ‘width’ measure is directly related to the width of the Poincart plot, namely SD width = Take two consecutive R-R intervals in the time series; namely (R-R, and R-R, + 1) Let A denote the point (R-R,R-R,,,) which they determine on the Poincare plot, as illustrated in Fig. 4. Let C(R-R,, R-R,) denote the projection, in the direction of the y-axis, of the point A(R-R,, R-R, + 1) onto the line of identity. Any point above the line of identity is defined as having a negative AR-R interval and any point below as having a positive AR-R value. Therefore SDAR-R Jz Relationships between time and frequency domain HRV variables Parseval’s theorem. where Y k is the discrete Fourier transform of X , and P,(k) is the power spectral density of X w Thus the signal variance and total spectral power are equal to each other. length A C = AR-R, HF power Geometrical interpretation of the ‘width’ measure The term ‘width’ is defined in terms of AR-R(AC) with respect to AB in Fig. 4. In particular, A B = A C .sincl= A C * sin-.n=-A C 4Jz For a continuous R-R time series, X N , with fast Fourier transform ( Y f ) and power spectral density function Px(f), the power spectrum of dX(t)/dt is 4 n z f 2 P , ( f ) . Thus, time domain parameters related to the first derivative or successive differences in the R-R interval time series are correlated with HF spectral power.