Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug design wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Prescription costs wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Neuropharmacology wikipedia , lookup
Plateau principle wikipedia , lookup
Pharmacognosy wikipedia , lookup
Theralizumab wikipedia , lookup
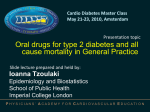
THE TITLE: Pharmacokinetic Drug Interaction with Gemfibrozil – Increased Risk of Concentration Dependent Adverse Effects of Rosiglitazone in Indian Volunteers AUTHORS: 1 Krishnan Karthickeyan*, 2Kanniappan Parthasarathy Arun, 3P Ramakrishnan Anand Vijaya Kumar and 4Mani Deepalakshmi Department of Pharmacy Practice, JSS College of Pharmacy, Rocklands, Udhagamandalam-643001 CORRESPONDING AUTHOR: Krishnan Karthickeyan, Telephone: 0423- 2443393 Fax: 0423- 2448427 Email: [email protected] ABSTRACT: AIM: To investigate the effect of Gemfibrozil on the pharmacokinetics of Rosiglitazone in Indian healthy adult male volunteers. METHODS: This prospective open label randomized two-way crossover study was conducted in 12 Indian healthy adult male volunteers after ethical committee approval. Rosiglitazone 4mg tablet was administered either with or without pre-treatment of Gemfibrozil 600mg tablets twice daily for 3 days. Plasma drug concentrations from time 0 to 12 hours were estimated by validated HPLC-UV method. The pharmacokinetic parameters were calculated and compared for statistical significance and 95% confidence interval (CI). RESULTS: Despite the absence of the interacting drug, the study subjects showed about 1.64 and 1.7 folds increase in Cmax and AUC 0- ∞ respectively than the literature values. Gemfibrozil caused an extremely significant increase (p<0.0001) in the mean values of Rosiglitazone AUC 0-∞ by 3141.5 µg-hr/ml (2738.5, 3544.5, 95% CI), Cmax by 242.34 µg/ml (208.41, 276.27, 95% CI) and half-life by 2.10 hours (1.474, 2.739, 95% CI). Gemfibrozil raised the mean AUC0 - ∞ and Cmax of Rosiglitazone by 2.2 folds and 1.6 folds respectively and these extents were comparable with values of western studies. CONCLUSIONS: Gemfibrozil increased the bioavailability of Rosiglitazone to the extent comparable with the reports found in literature. But the increased bioavailability of Rosiglitazone even without interacting drug enhanced the risk of concentration dependent adverse effects of Rosiglitazone in Indian subjects. This was further augmented by co-administration of Gemfibrozil. These findings supported the regulator’s recent decision to ban the drug in the country. INTRODUCTION Comorbidities and hence polypharmacy are more common in diabetic patients than other individuals. Anti-hyperlipidemics, anti-hypertensives and anti-depressants are the important class of drugs prescribed along with the prime hypoglycemic agents in diabetic patients [1]. One of the important risks in polypharmacy is drug-drug interaction (DDI) in which one drug influences the pharmacokinetic/pharmacodynamics of other(s) and results in reduced efficacy or increased toxicity. Though DDIs are common, only 10–12% of the prescriptions with potential interacting drugs have serious clinical consequences [2]. The conflicting reports found in literature that few studies clearly demonstrated drug interactions while others lacked to prove them retard our precise prediction and generalization of drug interactions and their consequences. This is due to the combination of interethnic variability in drug metabolism and other environmental factors. Rosiglitazone is an anti-diabetic drug that improves the insulin sensitivity and glycemic control in type 2 diabetes mellitus as an adjunct to diet and exercise. This thiazolidinedione class agent is extensively metabolized by CYP isoenzyme 2C8, with CYP2C9 contributing as a minor pathway [3] with no urinary excretion of unchanged drug. Gemfibrozil is a fibrate class of drug widely used for the treatment of dyslipidemias. It is a known inhibitor of CYP2C8 more potentially than CYP2C9 [4]. Gemfibrozil markedly increases the concentrations of CYP2C8 substrates like some cerivastatin and repaglinide [5, 6]. Gemfibrozil showed clinically significant pharmacokinetic interaction with rosiglitazone in a study conducted in Finnish volunteers[7]. Efficacy as well as toxicity of a drug is influenced by many factors including genetic and environmental. These factors vary from one geographic region to another and even among different ethnic groups within a particular geographic region. It is evident from the literature that Indians shown significant differences in pharmacokinetic behaviors of drugs like omeprazole, felodipine, isoniazid, zafirlukast, meloxicam [8-11]. Ethnic based variations in DDI are always possible due to various factors those include but not limited to genetics, social and environmental aspects. Hence we have investigated whether any such ethnic-specific difference in DDI between gemfibrozil and rosiglitazone in Indian subjects. MATERIALS AND METHODS: Ethical Considerations and Volunteer Recruitment The study was conducted in accordance with Ethical Guidelines for Biomedical Research on Human Participants, 2006 published by Indian Council of Medical Research. The study protocol was approved by the Institutional Review Board of JSS College of Pharmacy, Ooty. Written informed consent was obtained from twelve Indian adult male volunteers at the age group of 18 – 30 years with their freedom of choice. They were certified as healthy and to be fit to participate in the study by a physician after assessing the reports of physiological and vital biomedical parameters. Longterm therapy for any chronic diseases, alcoholism, and tobacco smoking/chewing were kept as exclusion criteria for the study. Study design This prospective open label randomized two-way crossover study was conducted at the BABE centre of the institution. As per the protocol, volunteers were randomized into two groups and one week wash out period was given between two phases of the study. At a particular phase, Rosiglitazone 4 mg tablet alone was administered to either a group as per randomization chart. The other group was given pre-treatment with Gemfibrozil 600 mg tablet twice daily for three days and on forth day rosiglitazone 4 mg was administered one hour post dose of gemfibrozil. The volunteers were requested for overnight fasting prior to study days and the study medications were administered to the volunteers in sitting position with 240 ml of water. The volunteers were under medical supervision throughout the sampling time. 5 ml of venous blood sample was collected from each volunteer at half an hour pre-dose and at 0.25, 0.5, 0.75, 1, 1.5, 2, 3, 4, 6, 8 and 12 hour post dose with adherence to universal precautions for blood collection. The plasma samples were separated and stored in deep freezer till analysis. Drug Concentration Assay Rosiglitazone and gemfibrozil concentrations in plasma were simultaneously estimated by a reverse phase high performance liquid chromatography (RP-HPLC) method developed and validated in our laboratory. The plasma samples were prepared by protein precipitation and calibration curves were constructed for both rosiglitazone and gemfibrozil by plotting the drug concentration versus ratio of chromatogram peak area of drug versus internal standard. An aliquot of 20 µL containing volunteer plasma sample with internal standard was eluted at the flow rate of 1 ml/minute through the C18 stationary column and UV detection was done at 276 nm. The method was validated by determination of linearity, lower limit of quantitation (LLOQ), accuracy, precision, extraction recovery, selectivity and stability. Calibration was performed by a least squares linear regression method and correlation coefficient was determined. The lowest concentration on the calibration curve with detector response five times greater than the blank human plasma was considered as the LLOQ. The analyte peak in LLOQ sample is to be identifiable, discrete and reproducible with 20% precision of and 80 – 120 % accuracy. The limit of detection (LOD) was determined as the concentrations with a signal-to-noise ratio of 3. The analytical method was validated for interday and intraday variations with four selected concentrations covering lower, medium and upper ranges of calibration curve. The precision was calculated as coefficient of variation and the accuracy was estimated as the percentage of the measured concentration over the nominal concentration for both the analytes and internal standard as well. The specificity of the method was also evaluated considering the interference due to the existence of endogenous substances in the extracted human plasma by comparing the chromatograms obtained from blank human samples. Room temperature stability was analyzed chromatograms obtained from the sample spiked with standards of study drugs with the chromatograms obtained from blank human samples. Room temperature stability was analyzed at 0, 4, 8, 12, 18, and 24 hours. Freeze-thaw stability was analyzed at room temperature after three repeated freeze-thaw cycles (−70◦C to room temperature), and permanent stability was analyzed using the samples kept at −70 C for 7 days. Pharmacokinetic and Statistical Analysis The concentration-time data of the study drugs were analyzed by non-compartmental method using PK Solver, a freely available menu-driven add-in program for Microsoft Excel written in Visual Basic for Applications (VBA), for solving basic problems in pharmacokinetic (PK) and pharmacodynamic (PD) data analysis [12]. The terminal elimination rate constant (ke) was estimated by linear least squares regression analysis of the terminal portion of the log concentrationtime data. The half-life (t1/2) of the study drugs was calculated using the formula: t1/2 = 0.693 / ke. The total area under the concentration time curve (AUC0-∞) was determined using the linear trapezoidal rule with extrapolation to infinity. The maximum concentration (Cmax) and time at which Cmax was observed (tmax) were determined from the experimental data. The results are expressed as means ± standard deviations. The pharmacokinetic parameters of rosiglitazone were compared by paired t-test (two-tailed). 95% confidence intervals on mean differences were also calculated. A two-sided p < 0.05 was considered significant and all the data were analyzed using the statistical software PSPP (v.0.7.5). RESULTS: Demographics All the 12 healthy volunteers have completed the study. The demographic parameters and other physiological, biochemical parameters of the two groups were compared at base line (Table 1). All of these parameters were found within the normal values and none of these parameters showed statistically significant difference. This showed that no pharmacokinetic variations could be caused by these parameters. HPLC Analysis The retention time of internal standard, rosiglitazone and gemfibrozil is 6.2, 10.8, and 14.2 minutes respectively. The correlation coefficient of 0.981 and 0.998 for rosiglitazone and gemfibrozil respectively confirmed the linearity of assay method developed. The accuracy was calculated as coefficient of variation and found within ±5 percent. The interday and intraday precision was found as less than 15% and 10% for rosiglitazone and gemfibrozil. The LLOQ of was found as 5.0 ng/ml and 0.5 µg/ml for rosiglitazone and gemfibrozil respectively. No endogenous interference with the analytes and internal standard was observed in blank plasma. The concentrations of the analytes and internal standard did not change within a day, within a week at different time points and after freeze-thaw cycles. The coefficient of variation at all these conditions was less than 5%. Pharmacokinetics The important pharmacokinetic parameters of rosiglitazone in both treatment phases were shown in Table 2. The AUC0-12 and Cmax of gemfibrozil at steady state were 135.75 ± 23.85 µg. h. ml1 (range, 83.93 – 154.54) and 29.66 ± 1.57 µg/ ml (range, 27.49 – 31.95) respectively. The Cmax of single dose rosiglitazone 4 mg was found as 427.82 ± 35.13 ng/ml while the AUC0-∞ of this single dose was 2607.968 ± 354.89 ng h.ml-1. Gemfibrozil raised the mean AUC0 - ∞ and Cmax of rosiglitazone by 2.2 folds (range, 1.8 – 2.5) and 1.6 folds (range, 1.44 – 1.75) respectively (Figure 1 & 2). The plasma concentration of rosiglitazone measured 12 hrs after dosing (C12) was 4.2 fold (range, 2.05 – 5.31) higher during the gemfibrozil pre-treatment. The half-life of rosiglitazone was significantly prolonged from 3.41 ± 0.27 h to 5.52 ± 0.77 h. by gemfibrozil (p= 0.1679). Good correlations existed between AUC0-∞ of gemfibrozil and change in AUC0-∞ and Cmax of rosiglitazone (r = 0.9314 and 0.8955 respectively) in this study volunteers. DISCUSSION: The significance of drug-drug interaction between gemfibrozil and rosiglitazone in Indian subjects was proven in this study. A single dose of rosiglitazone 4 mg had shown comparatively high peak plasma concentration and bioavailability than the values shown in the literature among the western population. A study done in Finland [13] reported the Cmax of 285±50ng/ml and AUC0-∞ of 1556 ± 368 ng.h.ml in healthy volunteers after 4 mg single dose of rosiglitazone and an another study carried out in Philadelphia [14] had reported 319 ± 97 ng/ml and 1552 ± 416 ng.h.ml-1 of Cmax and AUC0-∞ respectively. While our study group showed higher concentrations at tmax as 427.822 ± 35.13 ng/ml-1 and AUC0-∞ of 2607.968 ± 354.89 ng.h.ml-1 i.e., approximately about 1.64 folds higher concentration in the former parameter and 1.7 fold increase in the later. The single dose pharmacokinetic parameters of rosiglitazone 4 mg estimated in our study volunteers were comparable with the results obtained in Chinese healthy volunteers [15]. This study had reported the Cmax of 414.14 ± 73.30 ng/ml and 2436.90 ± 453.25 ng.h.ml-1 of AUC0-∞ for the reference standard rosiglitazone 4 mg tablet in a bioequivalence study. This showed the influence of ethnic differences on the pharmacokinetics of rosiglitazone. This sort of difference could be further confirmed with the pharmacokinetic parameters of rosiglitazone 2 mg tablet administered as single dose. The pharmacokinetic data shown in the prescribing information of rosiglitazone 2 mg oral tablet [16] was given as 156 ± 42 ng/ml of Cmax and AUC0-∞ of 733 ± 184 ng.h.m1-1. A study [17] conducted in Indian healthy volunteers with the same 2 mg rosiglitazone oral tablet showed the values of 215.9 ± 31.7 ng / ml of Cmax and 1441.89 ± 555.27 ng.h.ml-1 of AUC0-∞. The extent of increase in the values of these parameters was about 1.38 and 1.96 folds respectively those were comparable with our results shown for 4 mg of rosiglitazone as well. These differences in the pharmacokinetic parameters of rosiglitazone among different ethnic groups may be due to genetic variations existing in the drug metabolizing enzymes. The literature also indicated that the CYP2C8 allele frequencies of Caucasian European or Asian individuals cannot be considered as homogeneous groups [18]. Hence the risk for dose dependent adverse drug reactions of rosiglitazone could be more among Indian subjects. In this study volunteers, gemfibrozil 600 mg pretreatment had significantly increased the Cmax and AUC0-∞ of rosiglitazone to 670.15±75.32 ng/ml and 5749.47±670.95 ng.h.ml respectively. These results were attributed to CYP2C8 inhibition by gemfibrozil that could have impaired the hepatic metabolism of rosiglitazone. The extent of increase in the Cmax and AUC0-∞-1accounted for approximately 1.6 and 2.2 folds respectively and these extents of increase were comparable with the values reported in the western population during interaction between gemfibrozil and rosiglitazone. But the increase in the systemic bioavailability of rosiglitazone after interaction with gemfibrozil in Indian subjects should be the matter of concern, as it was shown very high (about 1.6 folds) than found in the western subjects under the same dosage criteria. As (dose dependent) Indian subjects might be at high risk for the adverse reactions even in the rosiglitazone could cause severe adverse drug reactions dependent on plasma concentrations absence of interacting drug. Further increase in the concentration of rosiglitazone during pharmacokinetic drug interaction could worsen the risk in the Indian subjects. The findings of this study was supported by the recent (October, 2010) decision of the ministry of Health and Family Welfare of India to prohibit the manufacture and sale of rosiglitazone through gazette notifications under section 26A of Drugs & Cosmetics Act 1940 [19]. CONCLUSION: Diabetes is the most threatening disease today in India. Diabetes is associated with many other chronic disease conditions and so polypharmacy in diabetes patients is inevitable. In such circumstances there is a high risk for drug-drug interactions among the drugs prescribed and the consequence of such interaction will be very serious. But the microsomal enzyme variations that are very common among different ethnic groups of population may result variation in the extent and consequences of such interactions. In this study, the pharmacokinetic interaction between gemfibrozil and rosiglitazone was studied for the first time in Indian subjects and the results have proven the high risk for concentration dependent adverse reactions of rosiglitazone even without any interacting drug. In the presence of interacting drug, the risk is still higher in this study subjects. However, the decision of Indian Pharmaceutical Regulatory Agency to ban the use of rosiglitazone is justified and the exposure to adverse reactions of rosiglitazone is avoided in Indian subjects. ACKNOWLEDGEMENTS: The authors would like to acknowledge the pharmaceutical industries M/s Glenmark Pharmaceuticals, India and M/s Sun Pharma, India those generously provided Rosiglitazone and Gemfibrozil pure drug samples as gift for bio-analytical method development of the drugs and also the Management, Staffs and Non-teaching staffs of JSS College of Pharmacy, Udhagamandalam for successful completion of this study. REFERENCES: 1. Reunanen A, Kangas T, Martikainen J, Klaukka T. Nationwide survey of co morbidity, use and costs of all medications in Finnish diabetic individuals. Diabetes Care 2000; 23: 126571. 2. Matthijs L. Becker, Marjon Kallewaard, Peter W.J. Caspers, Tom Schalekamp, Bruno H.C. Stricker. Potential determinants of drug-drug interaction associated dispensing in community pharmacies. Drug Safety 2005; 28: 371-78. 3. Tack C.J.J, Smits P. Thiazolidinedione derivatives in type 2 diabetes mellitus. The Neth J Med 2006; 64: 166-74. 4. Jari J. Lilja, Janne T. Backman, Pertti J. Neuvonen. Effect of gemfibrozil on the pharmacokinetics and pharmacodynamics of racemic warfarin in healthy subjects. Br. J. Clin Pharmacol 2004; 59: 433-39. 5. Backman JT, Kyrklund C, Neuvonen M, Neuvonen PJ. Gemfibrozil greatly increases plasma concentrations of cerivastatin. Clin Pharmacol Ther 2002; 72: 685–91. 6. Niemi M, Backman JT, Neuvonen M, Neuvonen PJ. Effects of gemfibrozil, itraconazole, and their combination on the pharmacokinetics and pharmacodynamics of repaglinide: potentially hazardous interaction between gemfibrozil and repaglinide. Diabetologia 2003; 46: 347–51. 7. Niemi M, Backman J. T, Granfors M, Laitila J, Neuvonen M, Neuvonen P. J. Gemfibrozil considerably increases the plasma concentrations of rosiglitazone. Diabetologia 2003; 46: 1319-23. 8. Joseph T, Gowrishankar R. Higher AUCs on oral administration of omeprazole and felodipine in Indian volunteers--are they clinically important? Indian J Physiol Pharmacol 1996; 40: 253-56. 9. Singh Neera, Dubey Sudhisha, Chinnaraj Saravanan, Golani Anil, Maitra Anurupa. Study of NAT2 gene polymorphisms in an Indian population: Association with plasma isoniazid concentration in a cohort of tuberculosis patients. Molecular Diagnosis & Therapy 2009; 13: 49-58. 10. Shubha Rani, Swati Guttikar, Anjali Zope, Rajeshwari Rathod, Manish Nivsarkar, Harish Padh. Zafirlukast pharmacokinetics in healthy Indian male subjects: Interethnic variability. IJAAI 2005; 19: 69-73. 11. Shubha Rani, Swati Guttikar, Rajeshwari Rathod, Bapu Cherian, Manish Nivsarkar, Harish Padh. Determination of oral meloxicam pharmacokinetic parameters in Asian Indians: Comparison with a German population. Saudi Pharmaceutical Journal 2004; 12: 144-49. 12. Y. Zhang, et al. PKSolver: An add-in program for pharmacokinetic and pharmacodynamic data analysis in Microsoft Excel. Comput. Methods Programs Biomed. (2010), doi:10.1016/j.cmpb.2010.01.007. 13. M. Niemi, J.T. Backman, M. Granfors, J. Laitila, M. Neuvonen, P.J. Neuvonen, Gemfibrozil considerably increases the plasma concentrations of Rosiglitazone, Diabetologia 2003; 46: 1319-23. 14. Ann K. Miller, Robert A. DiCicco and Martin I. Freed. The Effect of Ranitidine on the Pharmacokinetics of Rosiglitazone in Healthy Adult Male Volunteers. Clin Ther. 2002; 24: 1062-71. 15. Jia Yu, Ke Ma, Jinwen Qi, Ge Jin, Yan Wang. Shungan Fang and Gonghua Li. Bioequivalence and Comparison of Pharmacokinetic Properties of 4-mg Tablet Formulations of Rosiglitazone Hydrochloride and Rosiglitazone Maleate: A Single-Dose, Randomized, Open-Label, Two-Period Crossover Study in Healthy Adult Male Chinese Volunteers. Clin Ther 2008; 30: 2272-79. 16. Downloaded from the web address: http://www.accessdata.fda.gov/drugsatfda_docs/label /2007/021071s023lbl.pdf. 17. Mary Francis, Moghe A.A, Pawar S.R. and Khedkar S.S. Bioequivalence of Rosiglitazone Maleate 2 mg Tablets on Twelve Indian Human Male Volunteers, IJPS 2002; 64: 405-408. 18. García-Martín E, Martínez C, Ladero JM, Agúndez JA. Interethnic and intraethnic variability of CYP2C8 and CYP2C9 polymorphisms in healthy individuals. Mol Diagn Ther. 2006; 10: 29-40. 19. Downloaded from the web address: http://cdsco.nic.in/html/Drugsbanned.html. TABLES: TABLE-1: Demographic Characteristics Parameters Mean (SD) Group A pValue Group B Age (Years) 24.4 (2.30) 23.6 (2.88) 0.6424 NS Weight (Kg) 62.6 (3.62) 68.7 (6.57) 0.1506 NS Height (Cm) 169.6 (6.19) 170.2 (4.82) 0.8690 NS Heart Rate (Beats/min) 67.8 (7.82) 72.2 (4.50) 0.3174 NS Systolic Pressure (mmHg) 114 (5.48) 116 (8.94) 0.6847 NS Diastolic pressure (mmHg) 79.6 (0.89) 80 (1.41) 0.6122 NS SGPT U/L 10.4 (2.2) 11 (4.13) 0.8622 NS SGOT U/L 14 (4.12) 15.2 (4.87) 0.6867 NS Total 0.774 (0.07) 0.79 (0.06) 0.7234 NS Direct 0.22 (0.007) 0.212 (0.02) 0.5415 NS Indirect 0.594 (0.05) 0.574 (0.06) 0.6021 NS Serum Creatinine (mg/dL) 0.826 (0.05) 0.78 (0.06) 0.2933 NS Blood Urea Nitrogen (mg/dL) 21.2 (1.64) 23.8 (4.66) 0.3045 NS Fasting Blood Sugar (mg/dL) 77 (9.24) 80.6 (5.90) 0.4907 NS Serum Bilirubin (mg/dL) (NS= Non Significant) TABLE-2: Pharmacokinetic Parameters of Rosiglitazone (RZN) in 12 healthy male Indian Subjects after a single oral administration of 4mg Rosiglitazone and pretreatment with 600mg Gemfibrozil (GZL) twice daily for 3 days. Variables Treatment RZN Phase Cmax (ng/ml-1) tmax (h) t ½ (h) Ke (h-1) AUC0-t (µghml-1) AUC0-∞ (µghml-1) 427.82±35.13 RZN+GZL Phase 670.15±75.32 Percentage of Control (Range) 156.44±8.52 (144.01- 174.76) 1.3±0.34 1.1±0.21 90±28.54 (50-150) 3.41±0.27 5.52±0.77 162.83±27.87 (113.18- 189.07) 0.204±0.01 0.138±0.01 68.05±10.97 (54.01-88.87) 2099.25±257.14 3919.68±425.35 187.52±15.38 (167.89-209.34) 2607.96±354.89 5749.47±670.95 222.13±25.68 (179.70-254.70) Mean difference between treatments (95% CI) 242.34 (208.41, 276.27) -0.2000 (-0.5016, 0.1016) 2.107 (1.474, 2.739) -0.0662 (-0.08441,-0.04813) 1820.4 (1616.3, 2024.6) 3141.5 (2738.5, 3544.5) p Value p<0.0001 E.S. p=0.1679 N.S. p<0.0001 E.S. p <0.0001 E.S. p <0.0001 E.S. p <0.0001 E.S. Data are mean values ± SD; Cmax- Peak plasma concentration; tmax- Time to peak concentration; Ke- Elimination rate constant; AUC0-t- Area under the plasma concentrationTime curve (0 hr to 12 hrs); AUC0-∞ - Area under the plasma concentration- Time curve (0 hr – Infinity hours); E.S.- Extremely significant; N.S.- Non significant. FIGURES: Figure: Mean plasma concentrations of Rosiglitazone in 12 healthy subjects after a single oral dose of 4 mg Rosiglitazone following 3 days pretreatment with Gemfibrozil 600 mg twice daily. Rosiglitazone phase (■); Rosiglitazone plus Gemfibrozil phase (▲) PRE GE M P OS T GE M R os ig litaz one ratio (ng /m l) 700 600 500 400 300 200 100 0 0 1 2 3 4 5 6 7 T im e (h) 8 9 10 11 12