Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
From www.bloodjournal.org by guest on August 11, 2017. For personal use only.
Effect
of Hepatic
Dysfunction
Pharmacokinetics
in Marrow
By Gary C. Yee, Michael
The
effect
serum
of
kinetics
who
was
CSP
to
C
were
patients
mgldL).
dysfunction.
no
and
moderate
CSP
elimination.
(CSP)
(<
(2.0
distribution.
mild
5.0
mg/dL)
by
suppressive
agents,
CSP
is not myelosuppressive
at
therapeutic
concentrations,2
which
is important
in
marrow
transplant
patients.
In patients
with
acute
nonlymphocytic
leukemia,
a randomized
comparison
methotrexate
shows
that
significantly
faster
for prophylaxis
of graftCSP-treated
patients
have
engraftment
and
ization
than
methotrexate-treated
graft-v-host
disease
was also
group,
but
this
difference
less
not
recipients
dysfunction
during
course.5
Since
have
may
be at higher
signifi-
that
delayed
and
Hutchinson
consent
included
years
(range,
All
day
(daily
were
Research
Center.
analysis;
the
concentration
These
hepatic
dysfunc-
elimination
by the
Washington
Only
adults
age
and
toxicity.
Human
of
median
of
con-
function.
CSP-related
approved
University
dose
dose
suspension
1 1 to
Subjects
or
(age
the
Fred
16 years)
>
of patients
prophylaxis
day
doses
was
analyzed
were
between
28.5
steady-state
All
the
day
50.
in all patients
twice
CSP
was
during
continuing
after
7.5 mg/kg
administered
after
graft-v-host
and
tapered
5.5 and
or juice.
studied
transplant
gradually
milk
were
of acute
before
I 5 mg/kg/d),
in
of the courses
for
one
ranged
diluted
were
CSP
at least
although
CSP
courses
metabolite
the
received
180,
oral
CSP
developing
forms
in the
beginning
until
moderate
volume
serum
maximum
by hepatic
with
in
to
17 to 44).
patients
disease,
or
for
of
Cancer
were
The
CSP
risk
The
maximum
the
affected
patients
Committee
(P < .05).
absorption.
delayed
compared
daily
as
a
concentration-time
achieved
first
(> two
30 days
after
days).
marrow
grafting.
Hepatic
dysfunction
courses
none
were
(<
1.2 mg/dL),
5.0 mg/dL).
nase
was
divided
and
Similar
alkaline
not appear
defined
into
three
mild
(1.2
analyses
by serum
levels.
and
moderate
for
serum
performed
CSP
tests
was
(2.0
function
Renal
normal
(<
to
transami-
of hepatic
pharmacokinetics.
creatinine,
CSP
dysfunction:
to 2.0 mg/dL),
but these
with
bilirubin
of hepatic
were
phosphatase,
to correlate
by serum
categories
did
function,
1.5 mg/dL)
in all
41 courses.
CSP
frequently
their
elimination,6
after
oral
mine
effect
develop
posttransplant
is extensively
subject
to biliary
macokinetic
data
elimination.
dysfunction
tion
not
was
dysfunction
at which
was
as measured
hepatic
possible
statistically
study
in aplastic
anemia
results,
although
the incidence
disease
was not different
in
the CSP group.4
Marrow
transplant
the
Severe
in the CSP
common
indicate
clearance,
dysfunction
for
time
data
All
hospital3
was
cant.
A nonrandomized
patients
shows
similar
or severity
of graft-v-host
shorter
and
achieved
Review
and
hepatic
no hepatic
was
Thomas
constant
moderate
lag time
Protocols
undecapep-
tide with immunosuppressive
activity.’
The exact
mechanism
is unknown,
although
the drug selectively
inhibits
T lymphocyte
activity.
Unlike
most immuno-
of CSP
and
v-host
disease
with
centration.
stud-
determined
is a cyclic
rate
those
Patients
and E. Donnall
with
disease.
mg/dL).
to
as
Storb,
patients
were
1 .2
Rainer
patients
by radioimmu-
courses
Cyclosporine
Transplant
elimination
abnormal
pharmaco-
transplant
measured
with
YCLOSPORINE
as
of graft-v-host
concentration-time
among
S. Kennedy,
(CSP)
marrow
prophylaxis
concentrations
2.0
hepatic
defined
cyclosporine
in 28
for
Forty-one
divided
(1.2
on oral
examined
CSP
noassay.
dysfunction.
level.
received
Serum
ied.
hepatic
bilirubin
on Oral
metabolized
we analyzed
administration
of hepatic
Blood
and
our pharto deter-
dysfunction
on CSP
Our results
delays
CSP
show that moderate
or CSP
metabolite
MATERIALS
AND
hepatic
elimina-
Collection
Blood
atrial
samples
oral
CSP
catheters
after
for
at
Serum
-
at
two
Blood
hours,
samples
70 #{176}C
until
also
course.
least
from
patients
the study
centrifugation.
or frozen
obtained
indwelling
1 .5, 2, 3, 4, 6, 8, and
Some
preceding
temperature
room
were
at 0.5,
administration.
immediately
day
(5 to 7 mL)
(Hickman)
and
were
had
was
after
blood
allowed
serum
either
right
1 1 hours
was
analyzed
drawn
to clot
at
removed
the
next
analysis.
tion.
METHODS
From
Fred
Subjects
Pharmacy
Twenty-eight
(seven)were
Center
for
patients
with
admitted
to the
allogeneic
marrow
centration-time
courses
administration.
The
regimens
used
described
elsewhere.75
prepared
those
mide
the Clinical
Hutchinson
with
with
(60
Informed
were
mg/kg
consent
studied
Forty-one
in these
for
x 2) and
was
prepared
with
Blood. Vol 64, No 6 (December),
with
pp
all
donors
1277-1279
Schools
CSP
con-
18221,
after
oral
have
anemia
mg/kg
body
anemia
Research
irradiation
grafting
aplastic
high-dose
total
from
1 984:
and
(50
fractionated
obtained
patients
marrow
patients
cyclophosphamide
were
aplastic
Cancer
chemotherapy
patients
Briefly,
high-dose
or
transplantation.
pretransplant
to prepare
leukemia
leukemia
(21)
Fred
Hutchinson
DullS.
ED.
Submitted
Address
cyclophosphairradiation.
recipients.
Research
CA
awarded
1’. is the recipient
Oct
reprint
Section,
©
/8029,
the National
been
ogy
CA
Medicine,
No.
Center,
24, 1983;
accepted
1 984 by Grune
1 /24
CA
& Stratton,
15704,
Career
and
June
to Dr Gary
Oncology,
Columbia
of
by the National
ofResearch
of
of Oncology.
the Departments
of
Washington
Seattle.
ofAllergy
Division
and
University
33252,
Institute
requests
Division
Center,
Medicine,
and
by grants
and
Section,
Research
and
ofPharmacy
were
x 4), while
and
Practice
Supported
from
Pharmacology
Cancer
CA
30924,
CA
Cancer
Institute,
Award
Al
Infectious
02425
Diseases.
19, 1984.
C. Yee, Clinical
Fred
St, Seattle,
Hutchinson
WA
PharmacolCancer
98104.
Inc.
0006-4971/84/6406-0020$03.00/0
1277
From www.bloodjournal.org by guest on August 11, 2017. For personal use only.
1278
YEE
Assay
ET
AL
Procedure
Serum
The
samples
were
procedure
variation
was
at CSP
4,7%,
assayed
in duplicate
carried
out
as
concentrations
respectively.
The
of 100 and
minimum
20
by radioimmunoassay.
published.9
The
400
detectable
coefficient
ng/mL
of
is 8.8%
concentration
and
is about
Sc
20 ng/mL.
0
-Sc
Data
Analysis
-A
U
CSP
a
concentration-time
nonlinear
least-squares
PROPHET
when
available,
All CSP
serum
by the
maximum
mean
reported
fraction
K,.
absorbed
No
nonparametric
were
normally
statistical
uted,
the
was
also
different
patients
or
the
dose
and
of distriby
normal
the
patients.
were
Both
used.
two-sample
hepatic
were
t
test
When
the
data
were
Mann-Whitney
test
was
used.
A P value
noted
parametric
When
the
was
data
used
nonnormally
for
distrib-
of less
than
effect
cant
(P
<
function
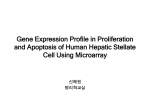
Table
1 . Effect
Patients
had
of hepatic
after
oral
with
delayed
of Hepatic
dysfunction
administration.
on
moderate
Cl/F
hepatic
values
Dysfunction
dys-
compared
on Oral
to
Cyclosporine
Pharmacokinetics
Severity
of Hepatic
Dysfunction
None
Parameter
(n
0.20
In
±
0.06
0.12
±
52.40
±
6.60
50.20
±
V,/F(L/kg)
2280
±
3.10
29.60
±
0.10
±
69.00
±
10.40
t,,(h)
c,_
1.30
(ng/mL)
c,,._/D
1.60
376.00
(hI
tP
P
-
(n
61.30
3.80
<
<
05 when compared
.05 when compared
Since
function,
these
patients
with
with moderate
±
0.20
to patients
to patients
there
was
no significant
ratios
between
and those with
groups
were
moderate
hepatic
difference
patients
with
no
mild hepatic
dys-
combined
hepatic
dysfunction
and Cmat/D
ratios
hepatic
dysfunction
Cmax
0.03
0.08
±
O.02t
29.60
±
7.lOt
±
7.80
21.20
±
6.10
±
0.30
±
0.50
±
85.00
77600
±
223.O0
14.30
129.40
±
36.50
±
0.40
1.70
62.20
4.40
±
±
0.40
3.90
none (< 1 .2 mg/dL),
with no hepatuc dysfunction.
with
either
no or mild hepatic
Our
correlate
and
compared
dysfunction.
also had
compared
to patients
(P < .05).
data
show
that
with
changes
to
Patients
increased
with
no or
mild (1.2
dysfunc-
changes
in CSP
in serum
elimination.
bilirubin
Serum
half-life
increased
as serum
bilirubin
increased,
with
mean values
of 3.5, 5.8, and 8.7 hours
in patients
with
no, mild,
and moderate
hepatic
dysfunction,
respectively.
Since
changes
in half-life
can be caused
by
changes
in volume
of distribution,
clearance,
or both,
we also calculated
these pharmacokinetic
parameters,
divided
by
the
estimated
fraction
decrease
in Cl/F
without
a change
with moderate
hepatic
dysfunction
with
no hepatic
decreased
CSP
increased
half-life
hepatic
dysfunction
than in patients
mean
half-life
7)
11.10
‘As determined
by elevated serum bilirubin levels:
to 2.0 mg/dL),
moderate (2.0 to 5.0 mg/dl).
tion.
SEM)
(ng/mL)
(mg/kg)
t,,,
383.00
±
Moderate
9)
-
Cl/F(mL/min/kg)
K,(h)
(Mean
Mild
25)
=
mild. or moder± SEM
(serum
DISCUSSION
hepatic
dysfunction
and those
with
dysfunction
was statistically
signifi-
.01).
also
with no.
the mean
.05
Mean
serum
half-life
increased
in patients
with
hepatic
dysfunction;
mean values
were 3.5, 5.8, and 8.7
hours
in patients
with no, mild,
or moderate
hepatic
dysfunction,
respectively.
The difference
in K between
with no
hepatic
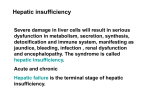
Cl/F in patients
Bars indicate
or Cmax/D
dysfunction
significant.
Table
I shows
the
CSP
pharmacokinetics
Moderate
(>2 0)
(I2-20)
with no hepatic
dysfunction
(Fig 1) (P < .05).
not appear
to be altered
by changes
in hepatic
dysfunction.
mild
RESULTS
patients
moderate
patients
Vd/Fdid
in Cmax
hepatic
hepatic
moderate
differences
anemia
the
statistically
doses,
CSP
divided
with
mild
comparisons.
considered
was
Fig 1 .
Cyclosporine
ate hepatic
dysfunction.
bilirubin.
mg/dL).
2)
dividing
Volume
with
methods
distributed,
C,,,,
by
and
significant
aplastic
(t,,5),
Cl/F).
those
statistical
estimates
at which
by the
calculated
for
to
and
calculated
received
statistically
leukemia
and
time
was
Mild
1<)
of
absorption
and
divided
also
for
2C
v time
reciprocal
provided
time
patients
(Vd/Fand
compared
as the
analysis
the
dose,
ofconcentration
was
parameters
were
dysfunction.
lag
on
preceding
([ng/mL]/[mg/kg]).
were
Pharmacokinetic
between
ratio
clearance
ofdose
function
Since
CI,,,,/D
as the
and
this
(K,),
half-life
concentration
the
weighted
CSP,
MODEL,’#{176}
available
from
(Cm,,),
serum
DRUG
program
were
concentration
CSP
bution
constant
Mean
(t,,,,).
with
in the analysis
data
For oral
rate
maximum
0.693
included
value.
elimination
fitted
concentrations
concentration
the measured
achieved
CSP
were
were
regression
system.”
data.
of
data
This
22.8
absorbed.
in Vd/F
compared
The
in patients
to those
dysfunction
clearly
shows
that
clearance
is responsible
for
the
(Fig 1 ). Cl/F
in patients
with mild
was
not significantly
different
with no hepatic
was increased
dysfunction,
from
3.5 to
although
5.8 hours.
was probably
due to an increase
in Vd/F (29.6
L/kg)
in patients
with mild hepatic
dysfunction.
Although
no single
test of hepatic
specific
marker
for drug
metabolism,
v
function
is a
serum
bilirubin
correlated
most
accurately
with
CSP
elimination.
Other
common
tests of hepatic
function,
such as serum
transaminase
or alkaline
phosphatase,
did not appear
to be helpful.
Cl/F
was not significantly
different
for
patients
with
abnormal
alkaline
phosphatase
values
(n
=
I 3)
compared
to
those
with
normal
alkaline
From www.bloodjournal.org by guest on August 11, 2017. For personal use only.
CYCLOSPORINE
PHARMACOKINETICS
phosphatase
kg). Similarly,
values
(n
patients
nase
those
v41.l
1279
28) (47.2
with elevated
v 49.7
serum
=
(n
I 1) did not eliminate
CSP
with normal
serum
transaminase
mL/min/kg).
=
Hepatic
dysfunction
ients
during
often
first
unclear,
30 days
v-host
men.5
disease
Hepatic
tion
the
or toxicity
dysfunction
of some
drugs
that
and
are
urine.
No
for
dose
and
aplastic
is
regielimina-
metabolized.’2
unchanged
studies
of CSP
but
a variety
of nonmalig-
as Fanconi’s
anemia,’4
and Wiskott-Aldrich
6
The
of CSP
by the US Food
and Drug
will probably
lead to increased
use for
indications,
tation.
Although
pharmacokinetics
mendations,
we
in patients
such
as marrow
transplan-
wide interpatient
variability
in CSP
precludes
any definite
dosing
recomsuggest
that clinicians
monitor
CSP
with
hepatic
dysfunction.
ACKNOWLEDGMENT
in
have been reported.
being performed
not
anemia,
such
concentrations
in all marrow
graft
recipients
and be
aware of the potential
for accumulation
of CSP or CSP
metabolites,
with its resulting
risk of nephrotoxicity,’7
CSP is extensively
elimination.6
Less
is excreted
and
diseases,
“nonapproved”
etiology
preparative
to delay
pharmacokinetic
leukemia
recip-
extensively
patients
with hepatic
dysfunction
Marrow
transplantation
is now
only
marrow
lymphoma’3
hematologic
thalassemia,’5
recent
approval
Administration
causes
during
the
early
acute
graft-
show that
to biliary
1 % of an administered
in the
(50.6
The
from
the
is known
studies
subject
than
=
in many
likely
are
nant
differently
(n
30)
period.
but the most
posttransplant
Pharmacokinetic
metabolized
than
occurs
postgrafting
non-Hodgkin’s
mL/min/
transami-
also
for
We
thank
Julie
Carlin
and
technical
assistance;
Lisa
Drs
Milo
Gibaldi
and
Dr David
Winter
of Sandoz,
Shoshanna
Eldred
Maslin
for preparation
H. Joachim
Deeg
Inc.
for
of the
for helpful
for financial
excellent
manuscript;
suggestions;
and
support.
REFERENCES
1 . Calne
tions
2.
RY:
lmmunosuppression
on cyclosporin
A. Immunol
Hellmann
A, Goldman
granulopoiesis
in vitro.
Deeg
3.
HJ,
CD,
Marrow
transplantation
first
and
host disease.
Transplant
Hows
Palmer
bone
5. Shulman
Kopecky
KJ,
venoocclusive
bone
ing
6.
A,
JM,
tional
(ed):
Conference
7. Thomas
ED,
plantation.
8.
hepatic
and
R, Clift
RA,
J Med
292:832,
895,
ED,
Clift
RA,
Fefer
A,
McGuffin
for acute
using
fractionated
Biol
Phys
8:817,
1982
Hersman
nonlymphoblastic
or single-dose
KC,
Elsevier,
Oncol
FL,
JE,
Storb
leukemia
irradiation.
Stewart
R:
Witherspoon
in first
Int J Radiat
Mamelok
Storb
(ed):
Bolt
Beranek
and
sharing.
Fed
RP:
ED,
Public
I 7.
in marrow
disease
and
drug
phar-
use
of marrow
1980
Review
HD,
Fanconi’s
of the
lymphoma.
Kennedy
JE,
anemia
J Clin
CD,
marrow
Sanders
Deeg
in vivo.
CD,
P. Sullivan
by
allogeneic
J, Papayannopoulou
KM.
Lancet
Johnson
FL,
Clift
T,
Storb
R:
1982
G,
in the
and
RA,
2:227,
Schiffman
transplantation
hematological
MS,
treated
P. Sullivan
34:284,
F, Buckner
Stewart
1983
for thalassemia.
LG,
transplantation:
immunosuppression
Appelbaum
61:954,
Buckner
Lum
R: Bone
ED,
L, Sanders
C, De Stefano
Complete
Oncol
Hepatic
ED:
Blood
Transplantation
remis-
resource
of non-Hodgkin’s
R, Thomas
transplantation
syndrome.
tion.
HM
Mass,
and
5:528,
K, Johnson
Doney
Ochs
Storb
RD:
Thomas
transplantation.
Marrow
P,
Marrow
1981
system
Pharmacokinet
FR,
Hi,
KM.
RJ,
JW,
Deeg
16.
M,
A in plasma
1983
15. Thomas
1975
J, Sanders
7:440,
RA,
trans-
R, Trapp
in Perry
I . Cambridge,
in the treatment
Borgna-Pignatti
Neiman
2:19,
PROPHET
RL,
Clin
Clift
Interna1982
Bone-marrow
The
I 3. Appelbaum
marrow
of cyclosporin
of an
A, Johnson
CD:
1980
suppl
Traber
cyclosporin
1974
Williams
14.
follow-
79: 1 1 78,
York,
R, Smith
WF:
transplantation
of hepatic
degeneration
metabolism
Fefer
Buckner
CD,
transplantation
ane-
M,
to measure
1982
Raub
.
I 2.
Doney
analysis
Proceedings
A. New
H,
sion
D,
An
Gastroenterology
A,
II
A
aplastic
Homberger
DRUGMODEL,
Notebook,
Proc 33:2390,
ofcyclosporin
Matthews
Glucksberg
N EngI
Use
for severe
ED:
Cyclosporin
Storb
comparing
E,
J Immunoassay
NHG:
macokinetics.
EC:
centrilobular
Thomas
Buckner
prophylaxis
GB,
on Cyclosporin
KG,
in
of graft-versus-
T: Pharmacokinetics
DiG
Lerner
and
Newman,
1983
Thomas
transplantation.
Beveridge
in White
PE,
McDonald
disease
R:
leukemia
samples.
Holford
Procedures
1982
HM,
serum
N,
J, Witherspoon
the
transplantation
Gauvreau
marrow
Flournoy
trial
15:1385,
33:382,
MS,
nonlymphoblastic
5, Gordon-Smith
marrow
Transplantation
mia.
Kennedy
P, Abisch
R: A radioimmunoassay
10.
of a randomized
for
Proc
and
A on human
1980
G, Sanders
acute
results
methotrexate
JM,
in allogeneic
ED,
Donatsch
Voges
ofcyclosporin
30:386,
K, Sale
for
9.
grafting-Observa-
46: 1 1 3, 1979
Effects
R, Thomas
Preliminary
cyclosporine
4.
JM:
R, Doney
Clift
remission:
Rev
Transplantation
Storb
Buckner
for organ
Wedgwood
Wiskott-Aldrich
immunological
reconstitu-
1982
Hi,
Storb
R, Thomas
Concentration-dependent
Transplant
Proc
ED:
Cyclosporine
toxicity
15:471,
1983
and
From www.bloodjournal.org by guest on August 11, 2017. For personal use only.
1984 64: 1277-1279
Effect of hepatic dysfunction on oral cyclosporin pharmacokinetics in
marrow transplant patients
GC Yee, MS Kennedy, R Storb and ED Thomas
Updated information and services can be found at:
http://www.bloodjournal.org/content/64/6/1277.full.html
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.