Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
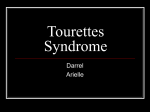
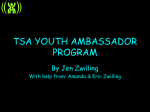
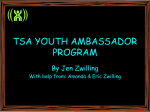
SEMINAR Seminar Tourette’s syndrome James F Leckman As our knowledge of Gilles de la Tourette’s syndrome increases, so does our appreciation for the pathogenic complexity of this disorder and the challenges associated with its treatment. Advances in the neurosciences have led to new models of pathogenesis, whereas clinical studies have reinvigorated early hypotheses. The interdependent roles of genes and environment in disease formation have yet to be fully elucidated. Results of epidemiological studies have prompted debate on how best to characterise and diagnose this disorder. Absence of ideal anti-tic drugs, combined with knowledge that uncomplicated cases of childhood Tourette’s syndrome frequently have a favourable outcome, has led to striking changes in care and treatment of patients. This seminar focuses on these changing views and offers a new perspective on our understanding of the pathogenesis of Tourette’s syndrome and on principles for treatment of patients with this disorder. Tic disorders have been the subject of speculation for at least the past 300 years. Despite the overt nature of tics and decades of scientific scrutiny, our ignorance remains great. Notions of cause have ranged from “hereditary degeneration” to the “irritation of the motor neural systems by toxic substances, of a self-poisoning bacteriological origin” to “a constitutional inferiority of the subcortical structures . . . [that] renders the individual defenseless against overwhelming emotional and dynamic forces”.1 Predictably, each of these aetiological explanations has prompted new treatments and new ways of relating to families. Symptoms and natural history The cardinal features of Tourette’s syndrome are motor and phonic tics that wax and wane in severity.2 Motor tics usually begin between the ages of 3 and 8 years, with transient periods of intense eye blinking or some other facial tic. Phonic tics, such as repetitive bouts of sniffing or throat clearing, can begin as early as 3 years of age, but typically they follow the onset of motor tics by several years.3 In uncomplicated cases, severity of motor and phonic tics peaks early in the second decade of life, with many patients showing a striking reduction in tic severity by age 19 or 20 years.4 However, the most severe cases of Tourette’s syndrome arise in adulthood. Extreme forms of this disorder involve forceful bouts of self-injurious motor tics, such as hitting or biting, and socially unacceptable coprolalic utterances—eg, shouting obscenities, racial slurs—and gestures. Motor and phonic tics arise in bouts over the course of a day, and change in severity over weeks and months.5 These episodes are characterised by stable intra-tic intervals—ie, time between successive tics—of short duration, typically 0·5–1·0 s. Less well known is the so-called self-similarity of these patterns across different times.6 Over minutes to hours, bouts of tics happen in groups. Over the course of weeks to months, many episodes of tics arise (figure 1). Lancet 2002; 360: 1577–86 Child Study Center and Departments of Paediatrics, Psychiatry, and Psychology, Yale University, New Haven, CT 06520-7900, USA (Prof J F Leckman MD) (e-mail: [email protected]) THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com This periodic higher-order combination of tic bouts could be the basis of the well-known waxing and waning course of Tourette’s syndrome. Knowledge of the temporal patterning of tics is important for the doctor, because it informs decisions about when to initiate anti-tic drugs, when to change drugs, and when to be patient and simply provide close monitoring and support to the family. Stated simply, if a clinician begins or changes a treatment at the end of a waxing period, the patient’s condition will improve irrespective of the efficacy of the intervention. Furthermore, a deeper understanding of the multiplicative processes that govern these timing patterns might clarify neural events arising every few milliseconds and the natural history of tic disorders over the first two decades of life. Many patients with tic disorders report associated sensory symptoms, including premonitory urges that incessantly prompt tics and feelings of momentary relief that follow performance of a tic.7 Many patients describe being besieged by these bodily sensations that are generally localised to discrete anatomical regions—eg, like an urge to stretch one’s shoulder or a need to clear one’s throat. These urges, and the internal struggle to control them, can be as debilitating as the tics themselves. Other antecedent sensory happenings include a generalised inner tension that can be relieved only by performance of a tic. A large range of auditory or visual cues can also prompt tics, but the nature of these cues is usually highly selective for individual patients—a cough, a particular word, an alignment of angles or specific shapes. Search strategy and selection criteria A computerised and manual search on PubMed of published work was done to identify studies about the pathogenesis of Tourette’s syndrome and its treatment, with particular focus on original reports published over the past 5 years. Selection criteria included a judgment about novelty and importance of studies and their relevance to the well-informed general medical doctor. In the case of treatment studies, only those interventions whose efficacy has been supported by at least one randomised, double-blind, clinical trial are cited. Keywords used included: “Tourette”, “tic”, “obsessivecompulsive”, “attention deficit hyperactivity disorder”, and “PANDAS”, among others. 1577 For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR in individuals with Tourette’s syndrome. Normal obsessive-compulsive-like symptoms are present in many young children, peaking at 2·5 years of age. This disorder when associated with tics generally has a prepubertal age of onset. When present, obsessive-compulsive symptoms are usually done in secret, and are most disabling in the home environment. They can lead to periods of depression.8–11 Individual tics Seconds Bouts of tics Hours Bouts-of-bouts of tics Epidemiology and genetics Days Bouts-of-bouts-of-bouts of tics Weeks Bouts-of-bouts-of-bouts-of-bouts of tics Months Time Figure 1: Fractal character of temporal occurrence of tics Progressively longer time scales (seconds to months) are depicted. In addition to tics, many patients with Tourette’s syndrome have symptoms of hyperkinetic disorder (known as attention-deficit hyperactivity disorder in the USA), obsessive-compulsive disorder, or both. These coexisting disorders can add greatly to morbidity associated with Tourette’s syndrome and detract from the patient’s overall quality of life8–11 (figure 2). Tics typically have the greatest effect on a patient’s self-esteem and peer and family relationships from age 7–12 years, especially during periods of waxing forceful motor tics and loud phonic tics that can go on for hours virtually nonstop. Hyperkinetic disorder takes a heavy toll from onset, with a negative effect on peer acceptance, school performance, and self-esteem. Increased irritability and rage attacks, and an increased vulnerability for drug abuse, depression, and antisocial behaviour are also not uncommon among patients with Tourette’s syndrome and hyperkinetic disorder.8–11 Lesser variants are typical Tics Hyperkinetic disorder Obsessivecompulsive disorder 0 5 10 15 Age (years) Figure 2: Age at which tics and coexisting disorders affect patients Width of bars shows schematically the amount the disorder affects a patient at a particular age. 1578 20 Once thought to be a rare disorder,12 the prevalence of Tourette’s syndrome is presently estimated to be between 31 and 157 cases per 1000 in children aged 13–14-years.13 Frequency of the disorder varies by age, sex, source of sample, and method of assessment. For example, studies on direct classroom observation and that use multiple informants consistently yield substantially higher prevalence estimates than do other assessment methods. Many patients identified with these techniques have mild characteristics and do not need long-term intervention apart from educational and other support. However, behavioural problems, in particular hyperkinetic disorder, are frequently associated with Tourette’s syndrome. Once diagnosed, these problems usually need prompt intervention to prevent or keep to a minimum adverse long-term results. In part, because of this association, children in special-education settings are more likely to be diagnosed with a tic disorder than children in community-based samples.14 Genes Genetic studies in twins and families provide compelling evidence that genetic factors are implicated in vertical transmission in families with a vulnerability to Tourette’s syndrome and related disorders. At present, the nature of vulnerability genes that predispose individuals to develop the disorder are unknown. Many genes probably have a role. Clarity about the nature and normal expression of even a few of the susceptibility genes in Tourette’s syndrome is likely to provide a major step forward in understanding the pathogenesis of this disorder. Future progress could also depend on identification of characteristic, biologically established, endophenotypes that are closely associated with specific vulnerability genes. Endophenotypes are measurable aspects of human psychiatric disorders that can either be used in linkage analyses as quantitative traits, be modelled in animals with the disease, or both. Promising endophenotypes include neurophysiological and neuroanatomical measures and patterns of treatment response (see section on neural substrates). The pattern of vertical transmission in family members suggests major gene effects, and results of segregation analyses accord with models of autosomal transmission.15,16 Historically, efforts to identify susceptibility genes within these high-density families with traditional linkage strategies have met with limited success. However, investigators studying a large FrenchCanadian family have reported evidence for linkage at 11q23.17 THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR Non-parametric approaches with families in which two or more siblings are affected with Tourette’s syndrome have also been undertaken.18 This sib-pair approach is suitable for diseases with an unclear mode of inheritance, and has been used successfully in studies of other complex disorders, such as type 1 diabetes mellitus and essential hypertension. In one sib-pair study of Tourette’s syndrome, two areas were suggestive of linkage, one on chromosome 4q and another on chromosome 8p.18 A genome scan of hoarding symptoms (a component of obsessive-compulsive disorder that can be seen in some patients with Tourette’s syndrome) as a quantitative phenotype was done with the same affected sib-pair data obtained by the Tourette’s Syndrome Association International Consortium for Genetics.19 Significant allele sharing was noted for hoarding phenotypes for markers at 4q34–35, 5q35, and 17q25. 4q is in close proximity to the region linked to Tourette’s syndrome.18 Identity-by-descent approaches have been used in populations in South Africa and Costa Rica. These techniques assume that a few so-called founder individuals contributed the vulnerability genes that are now distributed within a much larger population. The South African study implicated regions near the centromere of chromosome 2, and on 6p, 8q, 11q, 14q, 20q, and 21q.20,21 The marker in the French-Canadian family17 that was associated with the highest LOD score was the same marker for which significant linkage disequilibrium with Tourette’s syndrome was detected in the South African population. However, none of the chromosomal regions in which cytogenetic abnormalities have been found to co-segregate with phenotypes of Tourette’s syndrome has shown any convincing evidence for linkage in the high-density families, the sib-pair study, or the identity-by-descent studies. Several candidate genes have been assessed in people with Tourette’s syndrome, including various dopamine receptors (DRD1, DRD2, DRD4, and DRD5), the dopamine transporter, various noradrenergic genes (ADRA2a, ADRA2C, and DBH), and a few serotonergic genes (5HTT).22 Genetic variation at any one of these loci is unlikely to be a major source of vulnerability to the disorder, but in concert, these alleles could have an important cumulative effect. Environment Many epigenetic factors have been implicated in the pathogenesis of Tourette’s syndrome (panel 1). For example, children with a low birthweight with ischaemic parenchymal brain lesions are more likely to have tics and hyperkinetic symptoms by age 6 years than controls.23 Low Apgar scores recorded 5 min after birth have also been associated with an increased risk for tic symptoms.24 Males are more often affected with Tourette’s syndrome than females. Although this association could be attributable to genetic mechanisms, frequent male-tomale transmissions within families seem to rule out the presence of an X-linked vulnerability gene. This observation has led to the hypothesis that androgenic steroids during critical periods in fetal development could have a role in later development of the syndrome.25 It has also led investigators to test the efficacy of antiandrogenic drugs in treatment of refractory tics.26 Tic disorders have long been identified as stresssensitive problems. Typically, symptom exacerbations follow in the wake of stressful life-events. These events need not be adverse in character, as long as there is a high level of emotional excitement—eg, the start of school, impending holidays or birthdays, vacation trips.27 Stress- THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com Panel 1: Possible risk factors Genetic vulnerability Gestational and perinatal risk factors ● Severe nausea and vomiting during the first trimester ● Severe psychosocial stress of the mother during pregnancy ● Maternal use during pregnancy of coffee (more than 2 cups a day), cigarettes (more than ten a day), or alcohol (fewer than two drinks a day) ● Identical twin with a lower birthweight ● Low-birthweight children with evidence of parenchymal lesions, ventricular enlargement, or both ● Transient hypoxia or ischaemia during birth (labour >24 h), use of forceps, nuchal cord, evidence of fetal distress ● Low Apgar scores Severe psychosocial trauma, recurrent daily stresses (eg, teasing by peers), or extreme emotional excitement Recurrent streptococcal infections with post-infectious autoimmune response Drug abuse ● Exposure to androgenic drugs ● Chronic intermittent use of cocaine and other psychostimulants Co-existing medical or psychiatric disorders ● Hyperkinetic disorders ● Learning disabilities ● Depression ● Manic depression related neurotransmitters and hormones have also been implicated in Tourette’s syndrome. For example, compared with healthy controls, patients with the disorder have been reported to excrete substantially more norepinephrine in the 20 h preceding a lumbar puncture, to have raised concentrations of adrenocorticotropin hormone after this procedure,28 and to have high concentrations of norepinephrine and corticotropinreleasing factor in their cerebrospinal fluid.29,30 Taken together, these findings suggest that a subset of patients with Tourette’s syndrome could be characterised by heightened reactivity of the hypothalamic-pituitaryadrenal axis and related noradrenergic sympathetic systems. The past decade has seen the re-emergence of the hypothesis that post-infectious autoimmune mechanisms contribute to the pathogenesis of some cases of Tourette’s syndrome. Speculation about a post-infectious (or at least a post-rheumatic fever) cause for symptoms of tic disorder dates from the late 1800s.1 Group A  haemolytic streptococci (GABHS) are known to be a possible trigger of immune-mediated disease in genetically predisposed individuals. Acute rheumatic fever is a delayed sequela of these bacteria, arising about 3 weeks after an inadequately treated infection of the upper respiratory tract. Rheumatic fever is characterised by inflammatory lesions of the joints, heart, or central nervous system (Sydenham’s chorea). This disorder and Tourette’s syndrome probably affect common anatomic areas—the basal ganglia of the brain and related cortical and thalamic sites. Some patients with Sydenham’s chorea have motor and phonic tics and symptoms of obsessive-compulsive and attention-deficit hyperactivity disorder, suggesting that, at least in some instances, these disorders share a common cause. As in Sydenham’s chorea, antineural antibodies have been reported to be raised in the sera of some patients with Tourette’s 1579 For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR Cerebral cortex Striatum Striosome Indirect pathway Direct pathway GPe SNr GPi Basal ganglia output system Thalamus Subthalamic nucleus GABA Glutamate Figure 3: Schematic diagram of the major connections of the basal ganglia GPe=globus pallidus, pars externa; GPi=globus pallidus, pars interna; SNr=substantia nigra, pars reticulata. syndrome.31–34 Paediatric autoimmune neuropsychiatric disorder associated with streptococcal infection (PANDAS) has been suggested to represent a distinct clinical entity and include cases of Tourette’s syndrome and obsessive-compulsive disorder, in which a GABHS infection is likely to have preceded symptom onset.35 Although the importance of antibodies against neurons in relation to cause, and the association with previous GABHS infections, remains a topic of great debate,36 treatments based on this mechanism show some promise.37 Furthermore, if specific immunological alterations are associated with onset or acute clinical exacerbations, then the nature of these alterations should provide insight into the genetic, neuroanatomical, and immunological mechanisms implicated. This knowledge could provide a basis for rational design of therapeutic or preventative interventions. Neural substrates of habit formation and tics Habits are assembled routines that link sensory cues with motor action. Ideas at present have suggested neural substrates of habit formation are crucial for a better understanding of Tourette’s syndrome38–42 (figures 3, 4, and 5). Neuroscientists who are interested in learning and habit formation have focused on the motor, sensorimotor, association, inhibitory, and limbic (motivational and threat detection) neural circuits that course through the basal ganglia.39–42 These circuits direct information from the cerebral cortex to the subcortex, and then back to specific regions of the cortex, thereby forming multiple cortical-subcortical loops (figure 3). Cortical neurons projecting to the striatum outnumber striatal neurons by about a factor of ten.43 These cortical projection neurons to the striatum segregate into two structurally similar, but neurochemically distinct, compartments: striosomes and matrix (figure 4). These two compartments 1580 differ by their cortical inputs, with the striosomal medium spiny projection neurons mainly receiving convergent limbic and prelimbic inputs, and neurons in the matrix mainly receiving convergent input from ipsilateral primary motor and sensory motor cortices and contralateral primary motor cortices. The response of particular medium spiny projection neurons in the striatum is partly dependent on perceptual cues that are judged salient, so rewarding and aversive stimuli can both serve as cues.44 Several other less abundant striatal cell types probably have a key role in this form of habit learning, including cholinergic tonically active neurons and fast spiking interneurons. Tonically active neurons are very sensitive to salient perceptual cues because they signal the networks within the cortico-basal ganglia learning circuits when these cues arise44 (figure 4). They are responsive to dopaminergic inputs from the substantia nigra, and these signals probably participate in calculation of the perceived salience (reward value) of perceptual cues along with excitatory inputs from midline thalamic nuclei.40,45 The fast spiking spiny interneurons of the striatum are electrically coupled via gap junctions that connect adjacent dendrites. Once activated, these fast spiking neurons can inhibit many striatal projection neurons synchronously.46 The characteristic electrophysiological properties of the striatal fast spiking neurons—eg, irregular bursting with stable intra burst frequencies—are reminiscent of temporal patterning of tics.5 These fast spiking interneurons are also very sensitive to cholinergic drugs, suggesting that they are functionally related to tonically active neurons.47 Under normal circumstances, peak metabolic activity happens in the matrix compartment (matrix>striosome), as shown in figure 5.42 However, when this balance is reversed (striosome>matrix), tics and stereotypies are likely to arise.48 Although alterations in the structure of the basal ganglia, including loss of right-left asymmetry in the volumes of the lenticular nuclei, in patients with Tourette’s syndrome have been reported,49 present data from in-vivo neuroimaging and neurophysiological studies suggest that broadly distributed cortical systems (or their thalamic inputs) might be even more important GABA Glutamate Acetylcholine Dopamine Inputs to striosomes S Striosomal medium spiny neuron FS M Medium spiny neuron in the matrix Tan Tonically active neuron Cortical inputs to the matrix Midline thalamic nuclei Hippocampus Prefrontal cortex Striosome Anterior cingulate cortex M FS S M Tan Orbital frontal cortex S Motor and premotor cortex FS M Amygdala Fast spiking aspiny neuron Sensorimotor cortex Matrix Substantia nigra, pars compacta Figure 4: Schematic diagram of the major inputs into the medium spiny GABAergic projection neurons of the striatum THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR Balance of activity Striosomes Matrix M alterations in dopamine pathways, such as an increase in dopamine transporter capacity, are possible, but not necessary, features of pathophysiology.57 Developmental models S Under normal conditions S M Stereotypies and tics? Figure 5: Effect of an imbalance between medium spiny neurons in the two striatal compartments determinants of tic and hyperkinetic behaviours.50,51 These cross-sectional data also emphasise the need to gain a better understanding of developmental processes, sexual dimorphisms, and compensatory responses through prospective longitudinal studies. Early results of functional in-vivo neuroimaging studies have shown that voluntary tic suppression involves activation of regions of the prefrontal cortex and caudate nucleus and bilateral deactivation of the putamen and globus pallidus.52 If confirmed, these findings accord with the well-known finding that chemical or electrical stimulation of inputs into the putamen can provoke motor and phonic responses that resemble tics. They also reinforce the view that prefrontal cortical regions have a crucial role in expression of tic symptoms. In addition to behavioural inhibition paradigms, neurophysiological studies—eg, transcranial magnetic stimulation and prepulse inhibition of startle responses—have shown that the cortical silent period is shortened and intracortical inhibition is defective in patients with Tourette’s syndrome.53,54 This finding provides a possible explanation for the reduced motor inhibition and intrusive sensory occurrence in Tourette’s syndrome and obsessivecompulsive disorder. These in-vivo neuroimaging and neurophysiological findings might also be useful endophenotypes that could be proven to have value in prediction of treatment response to specific drugs or in clarification of the role of specific vulnerability genes. Recent neurosurgical procedures reinforce the functional importance of thalamic regions that are part of these cortical-subcortical loops.55 Results of one case study showed that high frequency stimulation of the median and rostral intralaminar thalamic nuclei produced an important reduction of tics. This effect could be caused by the effect of these midline thalamic nuclei on the tonically active neurons (figure 4), or on broadly distributed cortical systems and their corticostriatal projections. As in other movement disorders, a deeper understanding of the circuitry involved in Tourette’s syndrome could lead to specific circuit-based therapies, with deep-brain stimulation to treat refractory cases. As with habits and stereotypies, ascending dopaminergic pathways probably have a key role in consolidation and performance of tics. First, dopamine D2 receptor-blocking drugs are the mainstay of traditional pharmacological approaches to treatment of tics. Second, studies of monozygotic twins suggest that developmental shifts in the balance of tonic-phasic dopaminergic tone arise as a result of epigenetic differences, and density of dopamine D2 receptors might affect severity of Tourette’s syndrome.56 Third, further evidence shows that a range of THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com Future progress in elucidation of the pathogenesis and treatment of Tourette’s syndrome could be greatly accelerated with development of animal models. Thus far, the use of psychomotor stimulants, direct dopamine receptor agonists, behavioural stress sensitisation conditioning paradigms, and immune-based challenges to induce different levels of stereotypy in rats and other species seem to offer the greatest promise in modelling key components of the disorder’s phenotype.48,58–60 If tics, like stereotypies, vary in accordance with the balance of activity of medium spiny projection neurons in the striosome and matrix compartments of the striatum, then it should be possible to investigate the clinical effect of genetics, developmental insults, or both, that affect the number and sensitivity of medium spiny projection neurons in the two striatal compartments. For example, perinatal ischaemic and hypoxic insults involving parenchymal lesions strikingly increase risk of tic disorders.24 Furthermore, this model could provide a meaningful integration of knowledge about tics drawn from several perspectives. These include the stress responsiveness of tics (limbic activation), the presence of premonitory sensory urges (as sensory motor and primary motor cortical inputs converge on the fewer medium spiny projection neurons in the matrix), the reduction of tics when an individual is engaged in acts that need selective attention, and guided motor action (heightened activity within the matrix compartment). Results of two studies have shown an increase in oral stereotypies in rats after infusion of sera from patients with Tourette’s syndrome with high concentrations of antibodies against neurons compared with controls.59,60 One plausible hypothesis is that these antibodies could alter synaptic transmission and alter the balance between the striosomal and matrix compartments of the striatum. From a developmental perspective, many GABAergic interneurons of the cerebral cortex clearly migrate tangentially from the same embryonic regions in the ganglionic eminence that also give rise to the GABAergic medium spiny projection neurons of the striatum.61 Could adverse events arising at a specific point in development— eg, the differential loss of medium spiny projection neurons in the matrix compartment—account for the striatal imbalance and intracortical deficits in inhibition seen in some patients with Tourette’s syndrome?53 Assessment and diagnosis Clinical examination of a child with tics should include an assessment of the child or adolescent as a whole not merely as someone with tics.62,63 During the examination, the full range of difficulties and competencies should be charted: the clinician, family, and child must collaborate to reconstruct the child’s history, tic symptoms (onset, progression, waxing and waning, and factors that have worsened or ameliorated tic status), and present functioning. An important question is the extent to which tics are interfering with the child’s emotional, social, familial, and school experiences. To establish this fact, it is useful to monitor symptoms over a few months to assess their severity and fluctuation, effect on the family, and adaptation of the child and family to them. This monitoring can be helped if the family keeps records or uses standard forms.3 1581 For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR A central task of assessment is to explicate, clarify, and address family issues. Diagnostic assessment is closely connected with the first steps of treatment. During the process of clinical inquiry, the doctor can approach sensitive issues through clarification, education, and an opening therapeutic discussion with the child and family. As with other children with school-performance problems, the child with Tourette’s syndrome needs careful assessment of cognitive functioning and school achievement. Children with this disorder tend to have difficulties in attentional deployment, perseverance, and ability to keep themselves and their work organised. Many have poor penmanship. Schoolwork can be impaired by compulsions, such as the need to scratch out words or return to the beginning of a sentence. Neurological examination of a child with Tourette’s syndrome can be of great value. Tics are sudden habitual movements or utterances that typically mimic some fragment of normal behaviour and that use discrete muscle groups. As such, they can be confused with normal coordinated movements or vocalisations. Tics can also be mistaken for akathisia, tardive dyskinesia, or other hyperkinetic movement disorders.64 Once established, any given tic tends to persist for a time. Tics are often exacerbated by stress and fatigue. By contrast with other movement disorders, tics can arise during sleep, but are usually much attenuated. Some severely affected patients have immaturities or atypicalities on the neuromaturational examination (so-called soft signs). These signs might suggest disturbances in the body schema and in integration of motor control, but their relevance is not really clear. Findings on electroencephalography and structural MRI are generally normal and are not yet of proven clinical use (apart from patients in whom other neurological suspicions are present). Similarly, laboratory studies can establish a child’s general health profile and assist in differential diagnosis of other movement disorders, but there are no laboratory tests for positive diagnosis of Tourette’s syndrome or other tic disorders. Diagnostic criteria presently in use include the international classification of disease and related health problems, 10th revision (ICD-10)65 and diagnostic and statistical manual, 4th edition text revision (DSM-IVTR).66 Although clear differences exist between these classification schemes, they are broadly congruent with each other. To keep error to a minimum in case ascertainment and to produce an instrument measuring the likelihood of having Tourette’s syndrome, an international team of experts has published a diagnostic confidence index.67 Scores on this index are highly correlated with present tic severity, as measured by a psychometrically sound, widely used, clinician-rating scale, the Yale global tic severity scale.68 Once diagnosis of tic disorder has been established, careful assessment will allow the clinician to learn about fluctuation of symptoms. As the child becomes more comfortable, he or she will show his or her symptoms with less suppression or inhibition. Patients or family members might recognise a symptom as a tic after they have been educated about possible symptoms. The history of patients with long-standing Tourette’s syndrome is often confused by use of drugs. Often, drugs have been stopped because they were thought to have been useless or to have caused side-effects. The history of treatments and what they have meant to the child and family can be pieced together during the assessment. Also, the clinician can learn why earlier treatment attempts were not useful. When a child or adolescent, and his or her parents, is given enough time, over the course of several sessions, to 1582 Panel 2: Possible protective factors Informed and supportive home and school or occupational environment ● Maintenance of good sleep hygiene ● Regular physical exercise regimen ● Presence and use of special talents (eg, exceptional social skills, athletic skills, musical abilities, academic gifts) ● narrate their experiences, sadness, and disappointments, they may feel that their full story has finally been heard, perhaps for the first time, after having seen many doctors. This process of rethinking the past and integrating disparate threads of experience can be therapeutic in its own right, and could help to ease the immediate crisis that led to the consultation. The experience of being understood through the diagnostic process is reassuring. Many patients and families often feel supported, understood, and reassured by hearing a more or less detailed account of our understanding of the pathogenesis and natural history of Tourette’s syndrome. Knowledge that their experience is similar to that of other families, and that many of the most puzzling features of the disorder are typical (such as waxing and waning, symptom variation, ability to suppress tic for brief periods, and premonitory urges), can be a great reassurance to families. Treatment Multimodal treatment for Tourette’s syndrome is usually indicated.69 As noted above, this approach includes educational and supportive interventions appropriate for any chronic disease. Panel 2 outlines possible protective factors for the disorder. The various manifestations of the disorder are best treated in the context of a long-term relationship with a clinician who can help the patient, family, and school deal with the changing manifestations of the disorder through the years. Because acute and chronic stress can exacerbate tics, psychotherapeutic attention to difficulties of self-esteem, social coping, family issues, and school adjustment could have non-specific ameliorative effects on tic severity and on attendant anxiety and depression. Local chapters of patients’ advocacy organisations, such as the Tourette’s Syndrome Association, can have a very supportive role, by putting families of newly diagnosed children in contact with more experienced families. Parents should be encouraged to build on their child’s strengths. Many cases of uncomplicated Tourette’s syndrome can be successfully managed with just these interventions, and do not need anti-tic drugs. When patients present with coexisting hyperkinetic disorder, obsessive-compulsive disorder, depression, or two or three of these disorders, it is usually better to treat these comorbid disorders first, since successful treatment of them will often diminish tic severity. Anti-tic treatments Ideal anti-tic treatments are not presently available. None of the drugs or techniques can be used effectively just when tics are at their worst. Most of the available pharmacological drugs need long-term treatment, and many have potentially serious side-effects. Indeed, for some drugs, it is much easier to begin their use than to stop them. The natural waxing and waning pattern of tics often confounds the results of drug trials. Even without intervention, periods of severe tics will be followed by one of spontaneous waning. Because tic-suppressant drugs generally need several weeks to have their full effect, it is often difficult to distinguish response to a drug from THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR spontaneous waning of symptoms. Thus, it is usually best to avoid beginning or increasing drugs as soon as an exacerbation begins. Two classes of drug are most widely used to control tics associated with Tourette’s syndrome: ␣2 adrenergic agonists and neuroleptics.70 Guanfacine and clonidine are two ␣2 adrenergic agents originally developed as antihypertensives for adults. In low doses, clonidine reduces central noradrenergic activity by stimulation of presynaptic ␣2 adrenergic autoreceptors; guanfacine is believed to act more selectively on postsynaptic ␣2 adrenergic receptors in the prefrontal cortex. Use of these drugs is supported by results of randomised, placebo-controlled, clinical trials.71–73 However, this support is not uniform.74,75 Although they are generally not as potent as neuroleptics in suppression of tics, guanfacine and clonidine are more benign than neuroleptics in terms of potential short-term and long-term side-effects and are frequently the first choice in previously untreated individuals, especially those with mild-tomoderate symptoms. Treatment with these drugs for children and adults is usually started at a low dose and gradually increased. Beginning with a morning dose of 0·025 mg or 0·05 mg of clonidine, additional doses are added every 3–4 h. The size of each dose can be gradually increased to a total dose of 0·2–0·3 mg daily. Although the effect of each individual dose of clonidine wears off after about 3–5 h, the full ticsuppressant effects of the regimen could need 10–12 weeks to be apparent. Guanfacine is longer acting than clonidine, but is given in a similar way, in a range of 0·25–1·0 mg two or three times a day. The main side-effect of these two drugs in the recommended dose range is sedation, sometimes accompanied by irritability. This unwanted effect may need dose reduction or a change of drug. Reversible cardiac arrhythmias have been rarely reported with clonidine; however, the need for electrocardiographic studies at baseline and as soon as a stable dosage is reached remains controversial. Hypotension has not been a typical drawback in children taking these drugs. If a decision is made to discontinue these drugs, gradual tapering over a week or two is advisable to avoid tic flare-ups or rebound hypertension. Several typical and atypical neuroleptics are frequently used for treatment of Tourette’s syndrome, especially in patients with severe tics or whose tic symptoms are unresponsive to ␣2 adrenergic agonists. Efficacy of these drugs is associated with their potency in blockage of postsynaptic dopamine-2 receptors. Pimozide, haloperidol, sulpiride, and tiapride are the most frequently used typical neuroleptics, whereas risperidone and ziprasidone are two atypical neuroleptics with proven ticsuppressant efficacy.76–85 Sulpiride is a substituted benzamide and a selective dopamine-2 antagonist, and has been widely used, especially in Europe.86 In the only double-blind trial with this drug, George and colleagues87 undertook a 14-week placebo-controlled crossover study of fluvoxamine versus sulpiride, followed by single-blind combined treatment in 11 patients with comorbid Tourette’s syndrome and obsessive-compulsive disorder. Sulpiride monotherapy greatly reduced tics and non-significantly improved obsessive-compulsive symptoms. With neuroleptics, it is best to start with a low daily dose and gradually increase the dose. With sulpiride, the initial dose is 200 mg per day, gradually increasing to 1 g per day. However, use of high doses of these drugs rarely shows additional improvement in tics, and very often produces bothersome side-effects. Withdrawal from neuroleptics THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com can produce tic exacerbations and dyskinesias that can be delayed in onset by several weeks. Although neuroleptics are widely prescribed for patients with Tourette’s syndrome, many patients do not adhere to treatment. The most typical, dose-related side-effects of neuroleptics are sedation or dysphoria. Weight gain is also a drawback with most of these drugs, especially risperidone. Some children taking neuroleptics develop de-novo separation anxiety and school refusal. Although atypical neuroleptics are believed to have a low risk of tardive dyskinesia, acute extrapyramidal reactions—eg, torticollis, oculogyric crisis, akathisia—do arise, and they might need anticholinergic drugs. Because of potential QT changes, baseline and follow-up electrocardiography is recommended for risperidone, ziprasidone, and pimozide. It is also essential for the prescribing clinician to be familiar with potential cytochrome P450-related drug reactions, because fatal interactions have arisen with pimozide and erythromycinrelated antibiotics. In accordance with the neuromodulatory role of tonically active neurons in the striatum (figure 4), nicotinic drugs, especially in combination with neuroleptics, have shown some promise in clinical trials.86,87 Other drugs with some promise include low doses of pergolide, a mixed D1-D2-D3 dopamine receptor agonist,88 and locally injected dilute botulinum toxin.89 Some patients report a striking reduction in premonitory sensory urges after local injections of botulinum toxin. Furthermore, investigators have used several specific behavioural techniques, eg, habit reversal, hypnotherapy, relaxation, and biofeedback techniques, and a growing use of alternative treatments—eg, acupuncture and dietary supplements—has been seen. The most promising of these approaches is habit-reversal training. Azrin and Nunn90 developed this procedure for treatment of tics and other habits. As originally described, the intervention consists of several inter-related components. Four components focus on increasing patient’s awareness of their tic behaviour. The first component is response description, in which the patient is trained to describe tic occurrences in detail and to re-enact tic movements while looking in a mirror. The second one is response detection, in which the therapist points out each tic as soon as it takes place. The third includes practices aimed at helping the patient to identify the earliest signs of tic occurrence. The fourth is functional analysis, to identify situations in which tics are most likely to happen. A fifth component comprises competing response practice, which teaches individuals to produce incompatible physical responses dependent upon the urge to perform a tic. Individuals are instructed to isometrically contract tic-opposing muscles for 1–3 min, or until the urge to tic has passed. Other components include ones used to increase and sustain motivation and adherence, as well as one aimed at generalisation training. This intervention may be useful for some individuals, but systematic clinical trials have not been done.91 Treatment of hyperkinetic disorder in children with tics Treatment of hyperkinetic disorder in patients with a personal history of tics is common, complex, and controversial. In addition to classroom interventions—eg, small classes, close monitoring, assigned seat at the front of the classroom, assignment of a teacher’s aide, and other accommodations—and behavioural interventions at home (eg, parents’ management training and behavioural management are often very important, especially when the 1583 For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR child manifests disruptive behaviour), clinicians typically find drugs to be helpful in treatment of this disorder. Psychostimulants, such as methylphenidate, dexamfetamine, and related drugs are the most effective agents for uncomplicated hyperkinetic disorder. Although these drugs could be used with impunity in some individuals with tics, in a few cases, they can precipitate de-novo tics or exacerbate pre-existing tics in some individuals with Tourette’s syndrome. As a result, many clinicians will begin with clonidine or guanfacine, which, although not as potent as the stimulants, seem to be less prone to exacerbation of tics.71–73 Researchers in one large-scale, double-blind, clinical trial reported that the combination of clonidine and methylphenidate was most efficacious in treatment of children with both attention-deficit hyperactivity disorder and chronic tics.73 This study showed that these two drugs had differential effects, with clonidine being most helpful for impulsivity and hyperactivity, and methylphenidate being most helpful for symptoms of inattention. Treatment of tic-related obsessive-compulsive disorder Specific cognitive behavioural techniques (eg, exposure and response prevention training) might be useful for selected patients with Tourette’s syndrome who present with obsessive-compulsive disorder. Serotonin reuptake inhibitors are usually useful in treatment of symptoms of this disorder, but might not produce a complete therapeutic response.92 Augmentation with a low dose of a neuroleptic might increase the anti-obsessional efficacy of these drugs.93,94 At higher dosages, the serotonin reuptake inhibitors might occasionally precipitate or exacerbate tics. PANDAS interventions Although some cases of Tourette’s syndrome have been proposed to be a sequela of GABHS infections, this connection remains controversial, and is likely to be a contributing mechanism in only a few people with the syndrome.95 Antibiotic prophylaxis and arduous investigational interventions, such as plasma exchange or intravenous immunoglobulins, have been successfully used in a few patients with exacerbations after streptococcal infection.37,96 Such measures should be considered only with expert child psychiatric and paediatric consultation. At present, the main mandate for the clinician is to be vigilant in assessment of children with pharyngitis or those exposed to Streptococcus spp, and vigorous treatment and follow-up of those with positive throat culture results. development. Research paradigms used in these studies, and many of the empirical findings resulting from them, will probably be relevant to other chronic disorders of childhood onset and will also advance our understanding of normal development. References 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Future prospects Present ideas about Tourette’s syndrome have been shaped by advances in the neurosciences and our emerging understanding of the role of the basal ganglia in learning and habit formation. Although evidence that the same mechanisms have a role in habit formation and tics is circumstantial, progress has set the stage for a major advance in our understanding of this disorder. Continued success in these areas will lead to molecular insights into functioning of neural networks, complexities of information transfer, and targeting of specific circuits for more intensive study. Diagnostic, treatment, and prognostic advances can also be anticipated. The identification of susceptibility genes in Tourette’s syndrome will doubtless point us in new therapeutic directions, as will characterisation of possible autoimmune mechanisms active in the PANDAS subgroup of patients. In view of this potential, Tourette’s syndrome can be deemed a model disorder in which to study the dynamic interplay of genetic vulnerabilities, environmental events, and neurobiological systems active during early brain 1584 17 18 19 20 21 22 23 Kushner HI. A cursing brain? The histories of Tourette syndrome. Cambridge, MA. Harvard University Press, 1999. Robertson MM. Tourette syndrome, associated conditions and the complexities of treatment. Brain 2000; 123: 425–62. Leckman JF, King RA, Cohen DJ. Tics and tic disorders. In: Leckman JF, Cohen DJ, eds. Tourette’s syndrome tics, obsessions, compulsions: developmental psychopathology and clinical care. New York: John Wiley and Sons, 1998: 23–42. Leckman JF, Zhang H, Vitale A, et al. Course of tic severity in Tourette’s syndrome: the first two decades. Pediatrics 1998; 102: 14–19. Peterson BS, Leckman JF. Temporal characterization of tics in Gilles de la Tourette’s syndrome. Biol Psychiatry 1998; 44: 1337–48. Lin HQ, Yeh C-B, Peterson BS, et al. Assessment of symptom exacerbations in a longitudinal study of children with Tourette syndrome or obsessive-compulsive disorder. J Am Acad Child Adolesc Psychiatry 2002; 41: 1070–77. Bliss J. Sensory experiences of Gilles de la Tourette syndrome. Arch Gen Psychiatry 1980; 37: 1343–47. Spencer T, Biederman J, Harding M, et al. Disentangling the overlap between Tourette’s disorder and ADHD. J Child Psychol Psychiatry 1998; 39: 1037–44. Carter AS, O’Donnell DA, Schultz RT, Scahill L, Leckman JF, Pauls DL. Social and emotional adjustment in children affected with Gilles de la Tourette’s syndrome: associations with ADHD and family functioning. J Child Psychol Psychiatry 2000; 41: 215–23. Peterson BS, Pine DS, Cohen P, Brook JS. Prospective, longitudinal study of tic, obsessive-compulsive, and attention-deficit/hyperactivity disorders in an epidemiological sample. J Am Acad Child Adolesc Psychiatry 2001; 40: 685–95. Elstner K, Selai CE, Trimble MR, Robertson MM. Quality of life (QOL) of patients with Gilles de la Tourette’s syndrome. Acta Psychiatr Scand 2001; 103: 52–59. Costello EJ, Angold A, Burns BJ, et al. The Great Smoky Mountains Study of Youth: goals, design, methods, and the prevalence of DSMIII-R disorders. Arch Gen Psychiatry 1996; 53: 1129–36. Hornsey H, Banerjee S, Zeitlin H, Robertson M. The prevalence of Tourette syndrome in 13-14-year-olds in mainstream schools. J Child Psychol Psychiatry 2001; 42: 1035–39. Kurlan R, McDermott MP, Deeley C, et al. Prevalence of tics in schoolchildren and association with placement in special education. Neurology 2001; 57: 1383–88. Walkup JT, LaBuda MC, Singer HS, Brown J, Riddle MA, Hurko O. Family study and segregation analysis of Tourette syndrome: evidence for a mixed model of inheritance. Am J Hum Genet 1996; 59: 684–93. Leckman JF, Pauls DL, Zhang H, et al. Obsessive-compulsive symptom dimensions in affected sibling pairs diagnosed with Gilles de la Tourette syndrome. Am J Med Genet (in press). Merette C, Brassard A, Potvin A, et al. Significant linkage for Tourette syndrome in a large French Canadian family. Am J Hum Genet 2000; 67: 1008–13. The Tourette Syndrome Association International Consortium for Genetics. A complete genome screen in sib-pairs affected with Gilles de la Tourette syndrome. Am J Hum Genet 1999; 65: 1428–36. Zhang H, Leckman JF, Tsai C-P, Kidd KK, Rosario Campos MC, The Tourette Syndrome Association International Consortium for Genetics. Genome wide scan of hoarding in sibling pairs both diagnosed with Gilles de la Tourette syndrome. Am J Hum Genet 2002; 70: 896–904. Simonic I, Gericke GS, Ott J, Weber JL. Identification of genetic markers associated with Gilles de la Tourette syndrome in an Afrikaner population. Am J Hum Genet 1998; 63: 839–46. Simonic I, Nyholt DR, Gericke GS, et al. Further evidence for linkage of Gilles de la Tourette syndrome (GTS) susceptibility loci on chromosomes 2p11, 8q22 and 11q23-24 in South African Afrikaners. Am J Med Genet 2001; 105: 163–67. Comings DE. Clinical and molecular genetics of ADHD and Tourette syndrome: two related polygenic disorders. Ann N Y Acad Sci 2001; 931: 50–83. Whitaker AH, Van Rossem R, Feldman JF, et al. Psychiatric outcomes in low-birth-weight children at age 6 years: relation to neonatal cranial ultrasound abnormalities. Arch Gen Psychiatry 1997; 54: 847–56. THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR 24 Burd L, Severud R, Klug MG, Kerbeshian J. Prenatal and perinatal risk factors for Tourette disorder. J Perinat Med 1999; 27: 295–302. 25 Peterson BS, Leckman JF, Scahill L, et al. Hypothesis: steroid hormones and sexual dimorphisms modulate symptom expression in Tourette’s syndrome. Psychoneuroendocrinology 1992; 17: 553–63. 26 Peterson BS, Zhang H, Bondi C, Anderson GM, Leckman JF. A double-blind, placebo-controlled, crossover trial of an antiandrogen in the treatment of Tourette’s syndrome. J Clin Psychopharmacol 1998; 18: 324–31. 27 Silva RR, Munoz DM, Barickman J, Friedhoff AJ. Environmental factors and related fluctuation of symptoms in children and adolescents with Tourette’s disorder. J Child Psychol Psychiatry 1995; 36: 305–12. 28 Chappell P, Riddle M, Anderson G, et al. Enhanced stress responsivity of Tourette syndrome patients undergoing lumbar puncture. Biol Psychiatry 1994; 36: 35–43. 29 Leckman JF, Goodman WK, Anderson GM, et al. CSF biogenic amines in obsessive-compulsive disorder and Tourette’s syndrome. Neuropsychopharmacol 1995; 12: 73–86. 30 Chappell PB, Leckman JF, Goodman WK, et al. CSF corticotropin releasing factor is elevated in Tourette’s syndrome. Biol Psychiatry 1996; 39: 776–83. 31 Kiessling LS, Marcotte AC, Culpepper L. Antineural antibodies in movement disorders. Pediatrics 1993; 92: 39–43. 32 Singer HS, Giuliano JD, Hansen BH, et al. Antibodies against human putamen in children with Tourette syndrome. Neurology 1998; 50: 1618–24. 33 Morshed SA, Parveen S, Leckman JF, et al. Antibodies against striatal, nuclear, cytoskeletal and streptococcal epitopes in children and adults with Tourette’s syndrome, Sydenham’s chorea, and autoimmune disorders. Biol Psychiatry 2001; 50: 566–78. 34 Wendlandt JT, Grus FH, Hansen BH, Singer HS. Striatal antibodies in children with Tourette’s syndrome: multivariate discriminant analysis of IgG repertoires. J Neuroimmunol 2001; 119: 106–13. 35 Swedo SE, Leonard HL, Garvey M, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. Am J Psychiatry 1998; 155: 264–71. 36 Kurlan R. Tourette’s syndrome and ‘PANDAS’: will the relation bear out? Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infection. Neurology 1998; 50: 1530–34. 37 Perlmutter J, Leitman SF, Garvey MA, et al. Therapeutic plasma exchange and intravenous immunoglobulin for obsessive-compulsive disorder and tic disorders in childhood. Lancet 1999; 354: 1153–58. 38 Leckman JF, Riddle MA. Tourette’s syndrome: when habit forming units form habits of their own? Neuron 2000; 28: 349–54. 39 Graybiel AM, Canales JJ. The neurobiology of repetitive behaviors: clues to the neurobiology of Tourette syndrome. Adv Neurol 2001; 85: 123–31. 40 Suzuki T, Miura M, Nishimura K, Aosaki T. Dopamine-dependent synaptic plasticity in the striatal cholinergic interneurons. J Neurosci 2001; 21: 6492–501. 41 Jog MS, Kubota Y, Connolly CI, Hillegaart V, Graybiel AM. Building neural representations of habits. Science 1999; 286: 1745–49. 42 Brown LL, Feldman SM, Smith DM, Cavanaugh JR, Ackermann RF, Graybiel AM. Differential metabolic activity in the striosome and matrix compartments of the rat striatum during natural behaviors. J Neurosci 2002; 22: 305–14. 43 Zheng T, Wilson CJ. Corticostriatal combinatorics: the implications of corticostriatal axonal arborizations. J Neurophysiol 2002; 87: 1007–17. 44 Blazquez PM, Fujii N, Kojima J, Graybiel AM. A network representation of response probability in the striatum. Neuron 2002; 33: 973–82. 45 Raz A, Feingold A, Zelanskaya V, Vaadia E, Bergman H. Neuronal synchronization of tonically active neurons in the striatum of normal and parkinsonian primates. J Neurophysiol 1996; 76: 2083–88. 46 Koos T, Tepper JM. Inhibitory control of neostriatal projection neurons by GABAergic interneurons. Nat Neurosci 1999; 2: 467–72. 47 Koos T, Tepper JM. Dual cholinergic control of fast-spiking interneurons in the neostriatum. J Neurosci 2002; 22: 529–35. 48 Canales JJ, Graybiel AM. A measure of striatal function predicts motor stereotypy. Nat Neurosci 2000; 3: 377–83. 49 Swerdlow NR, Young AB. Neuropathology in Tourette syndrome: an update. Adv Neurol 2001; 85: 151–61. 50 Peterson BS, Staib L, Scahill L, et al. Regional and ventricular volumes in Tourette syndrome. Arch Gen Psychiatry 2001; 58: 427–42. 51 Fredericksen KA, Cutting LE, Kates WR, et al. Disproportionate increases of white matter in right frontal lobe in Tourette syndrome. Neurology 2002; 58: 85–89. 52 Peterson BS, Skudlarski P, Anderson AW, et al. A functional magnetic resonance imaging study of tic suppression in Tourette syndrome. Arch Gen Psychiatry 1998; 55: 326–33. THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com 53 Ziemann U, Paulus W, Rothenberger A. Decreased motor inhibition in Tourette’s disorder: evidence from transcranial magnetic stimulation. Am J Psychiatry 1997; 154: 1277–84. 54 Swerdlow NR, Karban B, Ploum Y, Sharp R, Geyer MA, Eastvold A. Tactile prepuff inhibition of startle in children with Tourette’s syndrome: in search of an “fMRI-friendly” startle paradigm. Biol Psychiatry 2001; 50: 578–85. 55 Vandewalle V, van der Linden C, Groenewegen HJ, Caemaert J. Stereotactic treatment of Gilles de la Tourette syndrome by high frequency stimulation of thalamus. Lancet 1999; 353: 724. 56 Wolf SS, Jones DW, Knable MB, et al. Tourette syndrome: prediction of phenotypic variation in monozygotic twins by caudate nucleus D2 receptor binding. Science 1996; 273: 1225–27. 57 Muller-Vahl KR, Berding G, Brucke T, et al. Dopamine transporter binding in Gilles de la Tourette syndrome. J Neurol 2000; 247: 514–20. 58 Leckman JF, Cohen DJ, Price RA, et al. The pathogenesis of Gilles de la Tourette’s syndrome: a review of data and hypothesis. In: Shah NS, Shah AB, eds. Movement disorders. New York: Plenum Press, 1986: 257–72. 59 Hallett JJ, Harling-Berg CJ, Knopf PM, Stopa EG, Kiessling LS. Antistriatal antibodies in Tourette syndrome cause neuronal dysfunction. J Neuroimmunol 2000; 111: 195–202. 60 Taylor JR, Morshed SA, Parveen S, et al. An animal model of Tourette’s syndrome. Am J Psychiatry 2002; 159: 657–60. 61 Anderson SA, Eisenstat DD, Shi L, Rubenstein JL. Interneuron migration from basal forebrain to neocortex: dependence on Dlx genes. Science 1997; 278: 474–76. 62 Cohen DJ. Finding meaning in one’s self and others: clinical studies of children with autism and Tourette’s syndrome. In: Kessel F, Bornstein M, Sameroff A, eds. Contemporary constructions of the child: essays in honor of William Kessen. Hillsdale, NJ: Lawrence Eribaurn Associates, 1991: 159–75. 63 Cohen DJ, Leckman JF. The child and adolescent with Tourette’s syndrome: changing perspectives on phenomenology and treatment. In: Kurlan R, ed. Handbook of Tourette’s syndrome and related tic and behavioral disorders. New York: Marcel Dekker, 1993: 461–80. 64 Jankovic J. Tourette’s syndrome. N Engl J Med 2001; 345: 1184–92. 65 Robertson MM, Banerjee S, Kurlan R, et al. The Tourette syndrome diagnostic confidence index: development and clinical associations. Neurology 1999; 53: 2108–12. 66 World Health Organization. Multiaxial classification of child and adolescent psychiatric disorders: international classification of disease and related health problems, 10th revision (ICD-10). Cambridge: Cambridge University Press, 1998: 43–45. 67 American Psychiatric Association. Diagnostic and statistical manual, fourth edition text revision (DSM-IVTR). Washington, DC: American Psychiatric Association Press, 2000: 108–16. 68 Leckman JF, Riddle MA, Hardin MT, et al. The Yale global tic severity scale (YGTSS): initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry 1989; 28: 566–73. 69 Leckman JF, King RA, Scahill L, Findley D, Ort SI, Cohen DJ. Yale approach to assessment and treatment. In: Leckman JF, Cohen DJ, eds. Tourette’s syndrome tics, obsessions, compulsions: developmental psychopathology and clinical care. New York: John Wiley and Sons, 1998: 285–309. 70 Freeman RD, Fast DK, Burd L, Kerbeshian J, Robertson MM, Sandor P. An international perspective on Tourette syndrome: selected findings from 3,500 individuals in 22 countries. Dev Med Child Neurol 2000; 42: 436–47. 71 Leckman JF, Hardin MT, Riddle MA, Stevenson J, Ort SI, Cohen DJ. Clonidine treatment of Tourette’s syndrome. Arch Gen Psychiatry 1991; 48: 324–28. 72 Scahill LD, Chappell PB, Kim YS, et al. Guanfacine in the treatment of children with tic disorders and ADHD: a placebo-controlled study. Am J Psychiatry 2001; 158: 1067–74. 73 Tourette Syndrome Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. Neurology 2002; 58: 527–36. 74 Goetz CG, Tanner CM, Wilson RS, Carroll VS, Como PG, Shannon KM. Clonidine and Gilles de la Tourette’s syndrome: double-blind study using objective rating methods. Ann Neurol 1987; 21: 307–10. 75 Singer HS, Brown J, Quaskey S, Rosenberg LA, Mellits ED, Denckla MB. The treatment of attention-deficit hyperactivity disorder in Tourette’s syndrome: a double-blind placebo-controlled study with clonidine and desipramine. Pediatrics 1995; 95: 74–81. 76 Shapiro AK, Shapiro E. Controlled study of pimozide vs placebo in Tourette’s syndrome. J Am Acad Child Psychiatry 1984; 23: 161–73. 1585 For personal use. Only reproduce with permission from The Lancet Publishing Group. SEMINAR 77 Eggers C, Rothenberger A, Berghaus U. Clinical and neurobiological findings in children suffering from tic disease following treatment with tiapride. Eur Arch Psychiatry Neurol Sci 1988; 237: 223–29. 78 Shapiro E, Shapiro AK, Fulop G, et al. Controlled study of haloperidol, pimozide and placebo for the treatment of Gilles de la Tourette’s syndrome. Arch Gen Psychiatry 1989; 46: 722–30. 79 Sallee FR, Nesbitt L, Jackson C, Sine L, Sethuraman G. Relative efficacy of haloperidol and pimozide in children and adolescents with Tourette’s disorder. Am J Psychiatry 1997; 154: 1057–62. 80 Robertson MM, Schnieden V, Lees AJ. Management of Gilles de la Tourette syndrome using sulpiride. Clin Neuropharmacol 1990; 13: 229–35. 81 George MS, Trimble MR, Robertson MM. Fluvoxamine and sulpiride in comorbid obsessive-compulsive disorder and Gilles de la Tourette syndrome. Hum Psychopharmacol 1993; 8: 327–34. 82 Sallee FR, Kurlan R, Goetz CG, et al. Ziprasidone treatment of children and adolescents with Tourette’s syndrome: a pilot study. J Am Acad Child Adolesc Psychiatry 2000; 39: 292–99. 83 Bruggeman R, van der Linden C, Buitelaar JK, Gericke GS, Hawkridge SM, Temlett JA. Risperidone versus pimozide in Tourette’s disorder: a comparative double-blind parallel-group study. J Clin Psychiatry 2001; 62: 50–56. 84 Dion Y, Annable L, Sandor P, Chouinard G. Risperidone in the treatment of Tourette syndrome: a double-blind, placebo-controlled trial. J Clin Psychopharmacol 2002; 22: 31–39. 85 Scahill L, Leckman JF, Schultz RT, Katsovich L, Peterson BS. A placebo-controlled trial of risperidone in Tourette syndrome. Neurology (in press). 86 Silver AA, Shytle RD, Philipp MK, Wilkinson BJ, McConville B, Sanberg PR. Transdermal nicotine and haloperidol in Tourette’s disorder: a double-blind placebo-controlled study. J Clin Psychiatry 2001; 62: 707–14. 87 Silver AA, Shytle RD, Sheehan KH, Sheehan DV, Ramos A, Sanberg PR. Multicenter, double-blind, placebo-controlled study of mecamylamine monotherapy for Tourette’s disorder. J Am Acad Child Adolesc Psychiatry 2001; 40: 1103–10. 88 Gilbert DL, Sethuraman G, Sine L, Peters S, Sallee FR. Tourette’s syndrome improvement with pergolide in a randomized, double-blind, crossover trial. Neurology 2000; 54: 1310–15. 89 Marras C, Andrews D, Sime E, Lang AE. Botulinum toxin for simple motor tics: a randomized, double-blind, controlled clinical trial. Neurology 2001; 56: 605–10. 90 Azrin NH, Nunn RG. Habit-reversal: a method of eliminating nervous habits and tics. Behav Res Ther 1973; 11: 619–28. 91 Piacentini J, Chang S. Behavioral treatments for Tourette syndrome and tic disorders: state of the art. Adv Neurol 2001; 85: 319–31. 92 McDougle CJ, Goodman WK, Leckman JF, Barr LC, Heninger GR, Price LH. The efficacy of fluvoxamine in obsessive-compulsive disorder: effects of comorbid chronic tic disorder. J Clin Psychopharmacol 1993; 13: 354–58. 93 McDougle CJ, Fleischmann RL, Epperson CN, Wasylink S, Leckman JF, Price LH. Haloperidol addition in fluvoxaminerefractory obsessive-compulsive disorder: a double-blind, placebocontrolled study in patients with and without tics. Arch Gen Psychiatry 1994; 51: 302–08. 94 McDougle CJ, Epperson CN, Pelton GH, Wasylink S, Price LH. A double-blind, placebo-controlled study of risperidone addition in serotonin reuptake inhibitor-refractory obsessive-compulsive disorder. Arch Gen Psychiatry 2000; 57: 794–801. 95 Singer HS, Giuliano JD, Zimmerman AM, Walkup JT. Infection: a stimulus for tic disorders. Pediatr Neurol 2000; 22: 380–83. 96 Garvey MA, Perlmutter SJ, Allen AJ, et al. A pilot study of penicillin prophylaxis for neuropsychiatric exacerbations triggered by streptococcal infections. Biol Psychiatry 1999; 45: 1564–71. Uses of error Tackers on the diaphragm K Thijssens, C Hoff, J Meyerink An 84-year-old woman had suffered from heartburn, nausea, vomiting, and postprandial abdominal pain. Her history contained bilateral hip prosthesis and repeated pulmonary embolism. A chest radiograph and endoscopy showed a type IV diaphragmatic hernia with a tortuous intrathoracic stomach and a grade II oesophagitis. A laparoscopic hernia repair was performed. The stomach was reduced into the abdominal cavity and the hernial sac resected. The resulting defect in the diaphragm was deemed too large for primary closure and a coated polyester mesh was attached to the crura with 5 mm titanium helical fasteners or tackers. After an uneventful recovery the patient suddenly developed a cardiogenic shock on the 14th postoperative day (central venous pressure 14 cm H2O, arterial oxygen saturation 70%). Chest radiography revealed no abnormality, including pneumothorax. With the medical history in mind the primary diagnosis of pulmonary embolism was made above the diagnosis of cardiac tamponade. When maximum supportive care, including intravenous fluids and high doses of inotropic agents, respiratory support, and human recombinant tissue plasminogen activator was ineffective, a cardiac ultrasound was done, establishing cardiac tamponade. Pericardiocentesis yielded 300 mL of blood per hour. A left thoracotomy was subsequently done. There was active bleeding of the epicardium from a number of pointed lesions, just opposite the tackers which had penetrated the pericardium. The offending tackers were removed and the defects in the epicardium sutured. The patient then went on to recover without further complications and was discharged 18 days after thoracotomy. One obvious point to make is that in spite of a history of pulmonary embolism, cardiac tamponade should have been considered from the onset of obstructive shock. In fact the administration of alteplase had a detrimental effect on the course of cardiac tamponade, which was already present at that time. Furthermore it is essential to consider the use of tackers in this and possibly other areas of endoscopic surgery. These 5 mm titanium helical tackers are introduced under manual pressure. Since the layers of tissue that are to be fastened are compressed there is no possibility of accurately controlling their depth of penetration. Department of Surgery, Medisch Centrum Leeuworden, Henri Dunantweg 2, 8934 AD Leeuworden, Netherlands (K Thijssens MD, C Hoff MD, J Meyerink MD) 1586 THE LANCET • Vol 360 • November 16, 2002 • www.thelancet.com For personal use. Only reproduce with permission from The Lancet Publishing Group.