Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
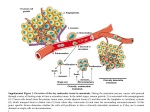
Invasion and metastasis of tumours Invasion & metastasis of tumours is a multistep process involving alterations in adherence, migration, ECM, proliferation etc. Describe how these processes and their regulation may provide therapeutic targets in cancer. Introduction-- Cancer cells become ominous when they acquire the property of invasion and metastasis. Due to this threatening property, targeted therapy is becoming difficult and in-effective in some cancers. Invasion and metastasis clearly demarcates between the aggressive and a non aggressive tumour in that invasion is the ability of the cancer cells to invade surrounding tissue and also actively degrade the tissue whereas metastasis involves the relocation of cell from the primary site to the secondary hospitable site or organ. Invasion and metastasis cascade comprises of different steps which are invasion and migration, intravasation, circulation, extravasation, colonization, proliferation and angiogenesis. (1) Cell migration is common during early embryogenesis, tissue repair and also lymphocyte migration during infection and inflammation and this procedure is smartly adopted by the cancer cells for their movement to other parts in the body. The transformation of epithelial cell type to mesenchymal cell type is called as epithelial-mesenchymal transition which is exploited by the tumour cells for invading tissues and relocating to new organs. Different molecules such as ECM components, integrins, cadherins, cell-cell adhesion molecules, factors of cellular movement, metastasis suppressors and several proteinases such as plasminogen activators, cathepsins, matrix metalloproteinase are all involved in the invasion and migration of the cancer cells. (1) Adherence-- First the cell needs to detach from the basement membrane and adhere to the ECM for migration (Erik Sahai). Generally epithelial cells are involved in protection from invading organisms with the help of tight junctions and their main characteristic features are anchorage dependent and avoiding motility. Adherens junctions play a crucial role in cell-cell adhesions by calcium dependent transmembrane glycoprotein such as cadherins. CDH1 gene encodes E-cadherin, which maintains tissue structure by tightly holding cells together. The main mechanisms involved in the down regulation of Ecadherin are the frame shift mutations in the gene (results in protein inactivation seen in breast cancer), methylation of promoter regions of CDH1 gene causes gene silencing, transcriptional repressors such as Snail, Twist and Slug involved in down regulation of E-cadherin expression, proteoglycans cause steric inhibition of E-cadherin protein and finally germ line mutations in CDH1 gene seen in gastric and colorectal cancers. (1, Gourav). N-cadherin up-regulation also promotes the motile nature of the epithelial cells. In addition to E-cadherin the cytokeratin expression is also reduced which maintains cell polarity. Cytokeratins are also essential for epithelial cell shape and stability which are crucial and can serve as clinical markers in detecting the transition from epithelial to mesenchyme. (1) E-cadherin is linked to the β–catenin on the cytoplasmic side for the cytoskeleton support and loss of Ecadherin can result in free β–catenin levels which translocates from cytoplasm to nucleus where they initiate transcription through binding to Tcf/LEF factors and also involve in production of proteins such as cyclin D1 and the Myc. E-cadherin gene (CDH1) acts as a metastasis suppressor gene which is confirmed from knock-Out experiments of CDH1 gene resulted in invasive cells but on the re-expression of the CDH1 gene resulted in repression of the invasiveness of the cells. (1) Up-regulation of the Ecadherin can be mediated by inhibiting the signalling pathways such as Wnt, TGF- β, FGF, EGF, STAT3 (signal transducer and activator of transcription 3) and NF- κB. Transcription level up-regulation of E-cadherin to curb the invasive behaviour can be possible by repressing the factors such as Snail, Twist and Slug factors which inhibit the GSK-3 β which is essential for Ecadherin regulation. Preventing the phosphorylation of the E-cadherins by RTks and c-Src proteins, which otherwise mediate the ubiquitinated degradation of the cadherins and catenins. (2) Inhibiting the proteolytic cleavage of E-cadherins can up-regulate them and inhibit the metastasis of the cancer cells. (2) Integrins are the cell surface receptors which interact with extracellular ligands such as fibronectin, vitronectin, laminin and collagen. Extracellular ligands acts as signals in transmitting messages to the intracellular side by binding to integrin receptors which in turn bind to the actin cytoskeleton and brings cell proliferation, survival, polarity, motility and differentiation. Up-regulation of integrins via c-Met receptor phosphorylation and activation can result in cell migration. Integrin such as αvβ3 mediates the high expression of a protein called periostin which is involved in preventing apoptosis of cancer cell via activating Akt/PKB pathway (2). Integrins play a crucial role in the tumour malignancy by activating the signalling pathways such as RTKs (Met, EGFR and Her2) through α6β4 which binds to the laminin of the ECM. Expression of αvβ3 and α3β1 integrins helps the circulating cells to bind to the vascular endothelial cells for extravasation. (Gourav) Figure-1 a) E-cadherin β-catenin and Wnt pathway b) Signalling pathways involved in EMT (epithelial mesenchymal transition) (1). Motility-- Cell motility is regulated by small GTPases such as Rho, cdc42, Rac, intgerin focal assembly and disassembly, secreted and plasma membrane proteases and actinmyosin contraction. (Gourav) Proteins such as ARP2/3 form a complex in the nucleation of actin and cofilin proteins involve in polymerization of the actin in the tumour cells. (Erik) Rearrangement of actin-cytoskeleton and degradation of adhesion complexes by producing lamellipodia in the moving direction and integrins helps in forming new focal contacts with the ECM and also dissolves the rear end connections by secreting proteases. The cell shape is regulated by proteins such as Rho GTPases which upon activation by RTKs can bring cell motility. Rac and Cdc42 belong to Rho protein family increase the expression of the MMPs (1). CD44 are transmembrane glycoproteins can communicate with the matrix components which act as adhesion molecules by binding to collagen, osteopontin, laminin, MMPs (Matrix metalloproteinases), fibronectin, chondroitin sulphate and heparin sulphate. These proteins act as receptors for the ligands such as hyaluronic acid. The cytoplasmic domain of the Cd44 is attached to proteins such as ankyrin and other proteins (Ezrin-moesinradixin) which interacts with actin cytoskeleton. The expression of c-Met receptor and its extracellular domain activation is induced by HGF ligand which results in auto-phosphorylation of the receptor. The signal is activated cytoplasmically by expression of Cd44v6 which interacts with the MEK or MAPK (1). In conclusion CD44v6 expression can result in cell migration through altering the actin cytoskeleton. (1). Expression of anti apoptotic proteins such as BCL2, BCl-XL and XIAP can resist the death and also loss of caspase-8 expression can increase the metastatic efficiency. (Gourav) Cancer cells secrete CSF1 receptors which attaches to the macrophages and these macrophages in turn stimulate the cancer cells by secreting EGF which results in motility of the cancer cells. The mechanism of EGF in cell invasiveness is mediated through Ras activation and dephosphorylation and also down-regulation of FAK (Focal Adhesion Kinase). Figure-2 Cd44 structure involved in the actin contraction and cell motility MMPs also contribute to the cell motility by secreting enzymes which degrade the matrix which will make a way for the cancer cells. The soluble MMPs secreted in the ECM are further activated by other enzymes and these MMPs are regulated by TIMPs (tissue inhibitors of MMPs) which keep the MMPs under control by inhibiting them to stop invasion and metastasis. Collagenases involve in degradation of the collagen, gelatinases in gelatin degradation, matrilysins degrade cell surface molecules such as E-cadherins and CD95-ligands. MMPs are inhibited through transcription, pro-MMP activation and MMP inhibition. Interferons block the transcription of MMPs by inhibiting MAPK-ERK signalling pathway. Antisense oligonucleotides or RNAi (RNA-interference) could be an alternative approach. Direct inhibition of MMPs by pseudo-mimetica (batimastat or marimastat) can be possible but the results are not accurate. Proteolytic enzyme uPA (urokinase plasminogen activator) can increase the activity of MMPs by binding to its auto receptor present on the stromal cell. So inhibition of uPA-uPAR system can be an active target in inhibiting tumour growth and metastasis. (1) On the contrary the immune system response is suppressed by the cancer cells by releasing factors such as TGF-β, IL-10 and IL-23 which suggest the cooperative role of immune cells for the cancer cells. (Gourav). Recent studies have revealed a nexus between the chronic inflammation and metastasis. Cytokines such as Cox-2 secreted by inflammatory cells and cytokine mediated NF-κB activation could result in tumour progression. Cells such as macrophages can also mediate tumour progression by responding to the hypoxic conditions of the tumour cells and release factors such as (VEGF, IL-8, PGE2) for blood supply, protease such as MMP9, uPA for the activation of the blood supply factors and also release growth factors EGF, IGF for the growth of the tumour cells. (Gourav) Figure-3 uPA system regulates the MMPs which are involved in cell motility and cancer metastasis. Intravasation— Cancer cells penetrate the endothelial cells for reaching to the target site through blood vessels or lymph vessels. Although most of the cancer cells reach their desired site via blood vessels, lymphatic vessels also aid in the transfer of these cancer cells. Moreover lymph vessels are more hospitable and advantageous to the cancer cells by not having a continuous basement membrane, pericyte coating and connection between endothelial cells are weak. (1) Expression of VEGF-C can promote lymph angiogenesis for the entry of the cancer cells in to the lymph. (1) In addition transcription factors such as Twist can promote metastasis by increasing the rate of haematogenous intravasation which has to be explored. (GOURAV P GUPTA) Circulation—Most of the cancer cells confront the challenges for their survival in the blood circulation by becoming anchorage independent, evade anoikis, autocrine growth signalling and sustaining the high oxygen and lymphocyte concentrations. Cancer cells avoid these hazards by forming micro-emboli by binding to the thrombocytes and erythrocytes. The main mechanism involved in that these cancer cells express tissue factor proteins which interact with proteins present on the platelets and results in the formation of micro-emboli. Circulating tumour cells can also serve as diagnostic marker and also knock out platelet mice studies revealed the low metastasis of the tumour cells indicating the importance and role of platelets in the metastasis of cancer cells. (1) The direction of the cancer cells is guided by the chemokines specifying their homing to specific organs. Chemokines regulate tumour formation by angiogenesis modulation, immune system activation, guiding to specific locations and autocrine growth stimulation. Malignant breast cancer cell express the CXCR4 receptor and these receptors ligands are found in liver, lung and bone cells. CXCR4 receptor expression in the lymph node metastasis is seen in melanomas and mammary carcinomas. Antibody mediated degradation of chemokines could serve as a therapeutic target. Angiogenic chemokine monoclonal antibodies significantly inhibit tumour vasculature and growth is seen in SCID mouse experiments in NSCLC (nonsmall cell lung cancer). (1) Extravasation-- Once Cancer cells are in circulation the reaching of the cells to desired locations is possible either by overcoming the stagnation in the lungs by squeezing through the capillaries or by binding to the circulating endothelial cells so that they can reach to the target destination via the endothelial cells. Although some of the cancer cells take an alternate route via arterial-venous shunt pathway but the main route is through the capillaries. (1) Tumour cells may also proliferate in the lumen of the blood vessels and break the endothelial walls either by secreting VEGF ligands or secreting proteases for their way to the desired organs. (1) (Gourav P gupta) Colonization, proliferation and angiogenesis-- Based on the principle of SeedSoil hypothesis which says that for the seed survival the compatible soil is necessary. For colonization in the new site the cancer cells need to survive in the new atmosphere which is only occasionally possible and the non proliferating cancer cells called as micro-metastases can serve as identification markers in the blood and bones through the α-EpCAM antibodies. (1) Target site recruits hematopoietic cells which release VEGF1 signals which draw endothelial cells expressing MMP9 receptors to the site for blood and nutrient supply making conducive environment for the survival of the incoming cancer cells. (Gourav p Gupta). Lung metastasis studies confirmed the ligand-receptor interactions o the cancer cells with the target cells. For example expression of α3β1 integrin on tumour cell binds to the laminin-5 on the target cell in the lung and also expression of CXCR4 on breast cancer cells binds to CXCL-12 expressing cells in the lungs. (Gourav P Gupta). Conclusion— In summary, there are some current anti VEGF drugs, selective MMPs inhibitors and also E-cadherin up-regulators along with other small kinase inhibitors which are quite effective in inhibiting the invasion and metastasis but they are not completely curing the disease. So new drug targets which are effective, are only possible by in-depth understanding of the mechanisms involved in invasion and metastasis.