Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
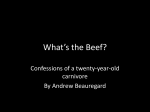
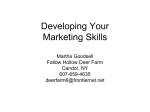
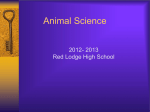
Man VS. Food The effect of red meat on health is an issue often debated in the media, whether that is its links to cancer or to obesity and cardiovascular health. However, is it red meat, or specifically processed red meat that is harmful? And how does red meat increase cardiovascular disease risk? Ischaemic heart disease and stroke are the top two causes of death in the world, accounting for 25.1%, and there is a lack of consensus in scientific papers on the subject. Therefore we feel this was a current and relevant topic to investigate. Aims and Objectives • To investigate the potential detrimental effects of consuming both processed and unprocessed red meat on cardiovascular health . • To look into the mechanisms of red meat (processed and unprocessed) on cardiovascular health. • To examine red meat consumption and cardiovascular health in different cultures and the impact of westernisation • To think about the future – should we stay away from processed red meat altogether? Or is there a safe limit? This site was made by a group of University of Edinburgh medical students who studied this subject over 10 weeks as part of the SSC. This website has not been peer reviewed. We certify that this website is our own work and that we have authorisation to use all the content (e.g. figures / images) used in this website. We would like to thank our tutor Zsanett Bahor for her guidance and support throughout the project. Total Website Word count: 8850 Word count minus Contributions page, References page, Critical Appraisal Appendix, Information Search Report, Word Version appendix and other sections clearly marked as Appendices: 5930 BACKGROUND KNOWLEDGE Epidemiology Cardiovascular disease (CVD) is an umbrella term encompassing diseases of the heart and blood vessels. The 4 main types of CVD are 1: • Coronary heart disease • Stroke • Peripheral Vascular disease • Aortic disease CVD is the largest cause of death in the world, with Ischaemic Heart disease and stroke alone accounting for 25.1% of all deaths 2. Every year in England and Wales, 124,000 deaths are caused by CVD and 1/3 of men and 1/4 of women will die from this disease 3, 4. However, this is compounded by the morbidity related to the disease, as for every death, there are two cases of complications, due to the effects of non-fatal strokes and heart attacks 3. Globally, deaths from CVD are expected to rise to 23.3 million deaths by 2030 2. CVD has a variety of risk factors, many of which are derived from lifestyle and are consequently modifiable. The main ones are 4: • Age • Sex – The cardio-protective effects of oestrogen mean that women are less likely to develop CVD than men 5. • Family history – due to a combination of shared genetic and environmental factors • Smoking • Hypertension • Hypercholestraemia – High total serum or high Low Density Lipoprotein (LDL) concentration increases risk. This is related to both genetics and diet. • Obesity • Hypertension Process of atherosclerosis A key factor in the precipitation of many cardiovascular events is the process of atherosclerosis 6. This is the build up of plaques in the arteries, with stable plaques leading to angina and claudication, and unstable ones to MI and stroke. 1. Endothelial injury The process begins with damage to the endothelium. This damage can be caused by hypertension, exposure to chemicals in smoking, or high blood lipid content. 2. Endothelial Dysfunction The damaged endothelium leads to an increased movement of LDLs to the sub-endothelium and increased monocyte adhesion and activation. 3. Macrophage activation Activated macrophages generate Radical Oxygen Species (ROS) leading to the oxidation of LDLs. They also produce cytokines, attracting further inflammatory cells to the area. Usually macrophages take up LDLs through receptor-mediated endocytosis with a negative feedback system, but oxidised LDL is not recognised. Instead, the modified LDL is absorbed by a scavenger receptor with no negative feedback, leading to a macrophage full of lipid. It is these Foam Cells that form the fatty streaks. 4. Smooth muscle recruitment Growth factors released by the damaged endothelium and activated macrophages cause the migration of smooth muscle cells from the tunica media to tunica intima, and their proliferation in the intima. 5. Fibrous Cap Formation The muscle cells secrete collagen in response to the cytokines released, leading to the formation of a fibrous cap over the foam cell accumulation. The cap is fragile, but its calcification makes it prone to rupture. At this stage, Angina or Claudication may occur. 6. Rupture A rupture of the plaque exposes the blood to collagen, starting the intrinsic coagulation cascade, leading to a thrombus and ischaemia. Alternatively, part of the plaque may break off and become an embolus 3, 7. The process of atherosclerosis. (From Grahams Child, Wikimedia Commons) Diet and CVD As both hypercholestraemia and obesity are risk factors for CVD, it is clear that diet can have a large influence on the likelihood of someone developing the disease. Consuming excess saturated fats has a large effect on developing CVD. As well as raising net blood cholesterol levels, saturated fat also increases blood LDL levels, which are a key component in atherosclerosis 8 . This is the most recognised method by which red meat can contribute to CVD. LDLs are atherogenic as they transport cholesterol to the tissues of the body, where they can be incorporated into blood vessels. High Density Lipoproteins (HDLs) carry cholesterol from the tissues to the liver to be metabolised, and so can be seen as “good cholesterol” 9 . Therefore, as well as net cholesterol levels in the blood, it is also important to have the correct balance of HDL and LDL. Red meat contains relatively high amounts of saturated fat compared to white meats, and so over-consumption will increase the risk of atherosclerosis 3, 10. Although saturated fats and atherosclerosis are a definite cause of CVD, there is controversy as additional factors and mechanisms may be involved. In a meta-analysis that involved 1,218,380 individuals, Micha et al. found that it was the salt and preservatives in processed red meat that caused damage, and that unprocessed meat had no effect of cardiovascular health 11. Furthermore, evidence from studies such as the cohort study by Sinha et al. involving 555,653 participants has shown that although processed meat is worse, increasing unprocessed red meat also increases CVD risk 12 . As such, it is difficult to come to a conclusion, as there are many studies that despite being well designed and with large participation rates, give different results. This controversy is particularly relevant in a public health context, as dietary guidelines should not place restrictions on foods that do not cause harm. MAIN BODY MECHANISMS OF DAMAGE There are many proposed mechanisms as to why the consumption of red meat could be having a detrimental effect on our cardiovascular health and here, we will focus on a few of these in detail. The first mechanism that we will mention is the theory that the microbes in our gut play a role. In a study performed by A. Koeth et al. 13, it is suggested that the metabolism of a chemical known as L- carnitine, a trimethylamine very similar in chemical structure to choline and often found in red meat, contributes to the promotion of atherosclerosis. This was based on a previous study produced by the same research group, that linked microbial breakdown of choline in the gut to CVD pathogenesis, due to it producing a chemical known as trimethylamine N-oxidase (TMAO)14. To investigate if this was also the case for L- carnitine, they performed various experiments on both humans and mice. Firstly, they demonstrated that TMAO was produced when Lcarnitine was broken down by microbiota. They did this by measuring TMAO plasma levels in 5 human subjects before and after treatment with antibiotics, and again once the flora in the gut were allowed to recover to normal levels. TMAO was barely detected during the treatment period, but was detected during the 2 periods of non-treatment, indicating that gut flora is required for the production of TMAO from L-carnitine. However, we appreciate that this is an extremely small sample size and the results that the study witnessed here could purely be down to chance. The most notable part of the investigation is that they looked at the fasting L-carnitine concentration in a cohort of 2, 595 stable subjects undergoing elective cardiac evaluation, and it’s relation to CVD risk. They saw a significant dose-dependant relationship between the level of fasting plasma L-carnitine concentration and prevalent CVD, which remained true when the results were adjusted for traditional CVD risk factors. However, when they looked at the relationship between the fasting plasma L-carnitine concentrations and incident CVD, there was no significant association, except for in the Cox regression model (which is a statistical analysis method that allows you to look at the survival rates of patients in relation to a given variable) 15 and only in those subjects with currently high levels of plasma TMAO. This suggests that the problem lies with the TMAO, and not the Lcarnitine itself. A systematic review by Dinicolantonio et al. 16 agrees with this finding that it is not the L-carnitine itself that is the problem. This review analysed 13 trials were supplementation of Lcarnitine was compared with control in patients with an acute myocardial infarction. They found that the L-carnitine supplementation caused a 27% reduction in all cause mortality and a 65% reduction in the development of ventricular arrhythmias when compared with placebo , therefore demonstrating that L-carnitine actually has a beneficial effect on the cardiovascular system following an acute coronary syndrome. The proposed mechanism behind this beneficial effect was seen to be multifactorial, but probably is related to L-carnitine’s ability to facilitate the transport of long chain fatty acids from the cytosol of myocardial cells to the mitochondrial matrix, where they undergo β oxidation and the toxic intermediates, that often induce ischaemia, are removed. It is also proposed to reduce left ventricular dilation (LVD) after an acute myocardial infarction, which is significant as LVD is often a strong indicator that the patient may progress to heart failure. This review suffered from the common limitations of such reviews, such as all but one of the trials reviewed having a small sample size, and not all of them being double-blinded. However, this review does propose an interesting new treatment avenue for acute coronary syndromes and highlights a mechanism by which the consumption of red meat may actually be beneficial to patients who have suffered a cardiovascular incident. This should be explored further with the production of a large cohort study. Looking once again at the study by Koeth et al. 13 interestingly, this study found that vegetarians and vegans have less of an ability to produce TMAO from L-carnitine than omnivores do. They compared 23 vegans and vegetarians with 51 omnivores, and found that the non-meat eaters had significantly lower fasting TMAO levels than the omnivores. They also examined a subset of the 23 vegans and vegetarians (although the paper does not put an exact number on the subset) and found that after supplementation with L-carnitine, that they had a markedly reduced ability to synthesise TMAO from L-carnitine. This suggests that your long-term diet has an effect on the microbiota in your gut and, hence, your ability to metabolise certain products. Having deduced that plasma TMAO levels seem to have an effect on the promotion of atherosclerosis, the authors set about determining why this was. Through their investigations, they found various reasons. Firstly, TMAO alters cholesterol and sterol metabolism, by increasing forward cholesterol transport and decreasing reverse cholesterol transport. TMAO also promotes the macrophage cholesterol accumulation and the surface expression of SRC and CD36 on the macrophages, which is important in the formation of foam cells. Finally, TMAO appears to lower the expression of Cxp7a1 enzyme, which is involved in the rate-limiting step of the catabolism of cholesterol. Although this study had flaws such as a small sample size, it highlights a potentially viable reason for the detrimental cardiovascular effects associated with red meat and could highlight a new way to tackle treating CVD. Another proposed mechanism underlying red meat consumption being detrimental to our health is the theory that the iron in red meat can have an influence on our blood pressure, and, as we know, hypertension is a well known risk factor for CVD. Iron is hypothesised to play a detrimental part in atherosclerotic disease because it can enhance oxidative stress due to the Fenton and Haber- Weiss reactions 17. A cross sectional study performed by Tzoulaki et al. 18, looked at 4680 men and woman of a similar age from the UK, USA, China and Japan, and compared an average of 8 blood pressure readings with the amount of meat reportedly consumed by the subjects in the past 24 hours. They measured their results in relation to the total amount of iron, the amount of haem iron (found in meat) and the amount of nonhaem iron (found in vegetables, cereals, beans etc.) consumed by the participants. The results showed that the consumption of red meat was positively associated with blood pressure, with the highest quartile of meat eaters having a 1.25mmHg increase in systolic blood pressure and a 0.73mmHg increase in diastolic blood pressure on average. However, the results also showed that both total iron consumption and non-haem iron intake had an inverse relation to blood pressure. They also found that haem iron intake was positively associated with blood pressure, but the association wasn’t high enough to be statistically relevant. Another paper looking at the effects of red meat consumption on the mortality rate of cardiovascular diseases and cancer 19, found that their results were still moderately attenuated after adjusting for haem iron. This suggests that although haem iron may not have a strong association with increasing blood pressure, it may be having some affect on the survival rates of certain diseases, including CVD. From these studies, it appears that the theory of iron in red meat being involved in the pathogenesis of CVD may be justified, but more research would be needed to clarify these results. However, there is discussion as to whether it is the red meat itself, or the processing of the meat that causes the problem. PROCESSED VS UNPROCESSED RED MEATS Another area in which there is debate is whether there is a significant difference between the effects of unprocessed red meat and processed meat and the incidence of CVD. There have been several claims that consumption of processed meat has a 20-40% higher risk of CVD than unprocessed red meat, which has been claimed to have no association with coronary heart disease11. It has been suggested that the reasoning behind this difference on health is due to the preservatives, such as sodium and nitrous compounds, added to the meat when it is heated and processed. The addition of sodium is claimed to be responsible for up to two thirds of the detrimental cardiovascular health difference between processed and unprocessed meat11. Processed meats, particularly bacon and hot dogs, have been found to contain up to 400% more sodium than unprocessed meats. This inevitably attributes towards a higher blood pressure, affecting cardiovascular health by causing hypertension20. There are many proposed theories as to why high salt intake is linked to hypertension and the precise mechanism still remains unclear. One study suggests that there may be blood volume expansion due to water retention21. Additionally, regular high sodium consumption weakens arterial compliance and causes endothelial damage20, thus contributing towards the process of atherosclerosis and increasing the chances of developing coronary heart disease. This claim has been supported by further evidence that has demonstrated that a low-sodium diet appears to significantly reduce the risk of heart failure and other coronary diseases22. However, it is important to consider that sodium intake is not the sole cause of hypertension and therefore we must acknowledge other factors that may cause an increase in blood pressure and eventually, CVD. Furthermore, the addition of nitrates and related compounds in processed meats have been hypothesized to influence cardiovascular health. It has been suggested that they have atherosclerotic promoting properties and cause vascular dysfunction11. However another study suggested that dietary nitrates and nitrites may have protective properties on the cardiovascular system22. Therefore, it is evident that we must consider the other mechanisms underlying the destructive effects of processed meat on cardiovascular health. When nitrites enter the human gastric system with certain food additives, it produces a compound called N-Nitrosamines which has been found to have destructive effects on the cardiovascular system23. Upon treating rats with N-Nitrosamines, they found that LDL levels increased whilst HDL levels markedly decreased. High levels of LDL contributes to atherosclerosis by inducing inflammatory cells to the arterial wall whereas low HDL means that these cells and excess cholesterol are not removed from the arterial lumen23. Together, it is evident that N-Nitrosamines are likely to increase the risk of CVD simply by promoting the atherosclerotic process. The potential factors in processed meat that cause a detrimental effect on the cardiovascular system in comparison to unprocessed red meat opens up many areas of potential research. Another way in which processed red meat has been said to contribute to CVD is through the consumption of high amounts of advanced glycation end products, as discussed in many papers24,25,26. Advanced glycation end products (AGEs) are modifications of proteins or lipids that have become nonenzymatically glycated and oxidised after exposure to sugars. The presence and build-up of AGEs in both intracellular and extracellular structures has been shown to contribute to the development of atherosclerosis25,26,27. Elevated levels of AGEs have been reported in those particularly suffering from type-2 diabetes with coronary heart disease, confirming that AGEs induce vascular injury by a variety of mechanisms28. AGEs are most commonly endogenously formed. This process is regularly linked with diabetes, as sufferers have accumulations of AGEs as a result of hyperglycaemia and increased oxidative stress29. CVD is a long-term complication of diabetes, and therefore someone with high AGE levels and diabetes is much more likely to go on to suffer from CVD. On the other hand, AGEs have been shown to originate from exogenous sources, such as diet29. AGEs are naturally present in animal products, but the process of cooking, in particular broiling, roasting, searing, grilling and frying, accelerates new formation24,25. Prolonged heating and high temperatures when processing food can also have this effect29. Foods particularly high in protein and lipids e.g. meat, egg yolks and cheese are seen to have high levels of AGEs26, but one prominent study, by Uribarri et al., found that it was meats in particular that contained the highest levels. Moreover, a more recent article for ‘Today’s Dietician’ confirmed that it is in fact red meats rather than white where AGEs are most prevalent24. Uribarri et al. concluded that the build-up of AGEs due to the processing of meats and other animal products offers a valid explanation for the detrimental health effects seen within the Western diet25. This study was interesting and robust, as it carried out research into a less publicised risk factor for CVD; its main strength being that it was carried out on a multi-ethnic population, so it took into account differences in cultural eating habits. However, participants were only sampled from the same area, Manhattan, and therefore the study may not be representative of the wider population. Several receptors have been identified for AGEs; however, the most important in vascular injury is named RAGE27. The interaction of AGEs with RAGE has been shown to increase oxidative stress and induce a state of endothelial cell activation27. In the vasculature, the main pathological outcome of AGE interaction with endothelial surface RAGE is the induction of intracellular ROS28. Through a variety of signalling pathways, ROS induction leads to the activation of many genes, including tumour necrosis factors, interferon-γ, cell adhesion molecules and interleukins 1, 6 and 8. These genes are very important in the process of inflammation and atherosclerosis28. Another mechanism, by which AGEs cause vascular injury, is the trapping of LDL in the subendothelium. There is increased retention of LDL in the wall of the aorta and increased detection by macrophages at this site. Therefore, there is increased localisation of AGE-LDL in blood vessels leading to increased production of foam cells, which, as discussed previously, go on to form fatty streaks, the precursors of atheromatous plaques29. In addition, AGEs have been shown to quench nitrous oxide (NO) availability and activity within the wall of blood vessels 28. Nitrous oxide is essential in the maintenance of the vasculature, as it inhibits leukocyte adhesion to vessel walls, vascular smooth muscle growth and platelet adhesion and aggregation. All of these processes may lead to the progression of atherosclerosis if not effectively regulated27. Furthermore, the structure and function of many important matrix molecules can be severely altered by AGEs28. Collagen is one of these molecules, found in the vessel wall with a particularly long-half life, and is a major target for AGE modification29. AGEs accumulate on these proteins and can cause formation of cross-links27, which trap other molecules such as immunoglobulins, LDL and soluble plasma proteins inside28. The cross-linking leads to an increased extracellular matrix area, which leads to an increase in the stiffness of the blood vessels27. Arterial stiffness puts a greater pressure on the heart, as it has to increase its contractility to ensure the same volume of blood is being ejected as if the arteries were healthy. This can lead to hypertrophy of the heart, increasing the likelihood of a cardiac event. There is a considerable amount of research into the ways of pharmacologically preventing the accumulation of AGEs within the body, particularly looking at blocking the interaction between AGE ligands and their receptor, RAGE27. However, more immediately, institutions such as the American Heart Association have come up with some solutions to avoiding AGE overconsumption25. A greatly reduced intake of AGEs can be accomplished by an increased consumption of legumes, fish, low-fat milk products, fruits, vegetables and wholegrain, and by reducing the consumption of fatty meats, solid fats and highly processed food, especially processed red meat25. The method of preparing and cooking food can also prevent AGE intake. Preparing meat by marinating it in lemon juice or vinegar for up to an hour before cooking has been shown to form less than half the amount of AGEs than in untreated meat25. Finally, cooking methods such as stewing, steaming, poaching and boiling could be better publicised in order to educate the general public about low AGE-producing cooking methods25. As discussed, AGEs have a variety of mechanisms by which they can accelerate the process of atherosclerosis, increasing the likelihood of cardiac events in those who have high levels in their body, particularly as a result of consuming large quantities of processed red meat. In order to avoid an increased risk of CVD, processed red meat should be avoided. Having explored the detrimental health effects of processed red meats, we have acknowledged that it’s increasing consumption may be due to the westernisation of our diets. WESTERNISATION In the last fifty years or so, the westernisation of diets has had detrimental health effects in both thriving cities and isolated communities all over the world, particularly concerning those in developing countries where the sudden influx of fatty and sugary foods has caused the incidence of non-communicable diseases to sky rocket30. This aptly named “meat-sweet” diet is characterised by an increased consumption of saturated fats, red and processed meats, and a low intake of fruits, vegetables and fibre31. The dramatic change in lifestyle in recent years, where it is now far more convenient to buy a pre-prepared, fat-laden burger than to cook a healthy family meal, is a huge risk factor of developing diabetes and coronary heart disease32. Genetically speaking, humans existing today are not completely dissimilar to the Stone Age hunter-gatherers in the late palaeolithic era33. Although varying greatly both seasonally and location-wise, the diets of Palaeolithic humans consisted mainly of animal protein from game; the meat from which was leaner, containing far less fat, than twenty first century factory farmed beef33. With this high intake of red meat, one would expect our Palaeolithic ancestors to have had atherosclerotic arteries and high blood pressure; however, due to the meat containing a higher degree of polyunsaturated fats and the people having a more active lifestyle, this is not the case33. Conversely, a sedentary lifestyle and high intake of saturated fats has contributed to the modern man being at risk of “diseases of civilisation”, such as hypertension, diabetes and cancer33. A study in Japan found positive correlations between mortality from coronary heart disease in men (ages 55 to 59 years old) and an increase in western foods, such as those containing animal protein and cholesterol34. This study considered dietary changes throughout the whole country, in both traditional rural areas and modern urban areas, making it more applicable worldwide. In Alaskan natives, where the traditional diet is hugely reliant on fat, it is interesting to see that replacing this with a similarly fatty western diet still increases the risk of CVD. This is thought to be due to specific fatty acids rather than the total fat intake; the fatty acid make-up of the traditional marine based Alaskan diet promotes better cardiovascular health compared to that of a typical western diet35. Nowadays, with 35% of Scottish men suffering from hypertension and CVD being the UK’s biggest killer36, it is suggestive that it is not the meat itself, but what we are doing to it and how it is being eaten which is contributing to the premature deaths of thousands of individuals. The meat we eat nowadays is completely different to the wild game that our ancestors once ate; factory-farmed meats differ hugely in their lipid profile and chemical pollutant content37. Long-chain unsaturated omega-3 fatty acids are abundant in plant materials, and are also present in the meat of game animals. The consumption of this n-3 fatty acid by humans was far greater in Palaeolithic times, and it has been shown to increase the concentration of HDLs, lower blood pressure and have a beneficial effect on cardiac muscle rhythmic stability37. Modern meat contains more saturated fatty acids38, which are linked to an increased risk of coronary heart disease39. Cattle that have been fed solely on grass have much higher concentrations of conjugated linoleic acid (CLA) in their meat tissue; this is an isomer of octadecadienoic acid and the principle dietary source of it is from ruminant meat and milk 40. CLA has been found to comprise of anti-carcinogenic and anti-atherogenic properties in animal studies40, reiterating that what we feed domesticated livestock has huge implications on the quality of the meat. There are also major health implications involved in this high-demand production of meat; feeding cows ruminant waste material in an effort to relieve the tension between food supply and demand is what brought about bovine spongiform encephalopathy, or mad cow disease41. So, looking at what we have found in our research, how much, if any read meat is safe? SO HOW MUCH, IF ANY, RED MEAT IS SAFE? Whilst we have gone into depth on the pathophysiology of how red/ processed meat affects CVD risk, there is also a wealth of epidemiological evidence – and disagreement – on the subject. The Seven Countries Study42 sparked current interest, as it was the first to find a significant correlation between red meat and CVD. Since, many studies have agreed, linking red meat with stroke and ischaemic heart disease43, atherosclerosis44, and acute coronary syndrome45. However more recently, scrutiny has changed to the processing procedures of meats. Micha et al.‘s large meta-study found the increased salt and preservatives in processed meat to be the disease causing mechanism rather than the fat content found in all red meat, only finding a link between CVD and processed meats11. However, there are conflicting studies which claim that while processed red meat is indeed more detrimental to cardiovascular health, unprocessed red meat is still associated with a 13% increased risk of death from cardiovascular causes for every additional daily portion46. Whilst associations aren’t always consistent, there is enough significant evidence to link processed red meat consumption with CVD. Whether unprocessed red meat consumption is also a risk factor is more controversial, and difficult to assess as diet is very complex, as are the mechanisms and risk factors for CVD. These inconsistencies limit the reliability of current recommended intakes for red meat. The government’s current guidelines, issued by the Department of Health, recommend that anyone eating more than 90g of red/processed meat per day should aim to cut down to 70g a day, which is the UK daily average47. This recommendation is based on links between eating these foods and bowel cancer, but does not evaluate or provide information on red/processed meat intake as a risk factor for CVD. Considering that coronary heart disease is the leading cause of death in the UK and worldwide1, this is not something to be overlooked. For example, Pan A et al.19 estimated from analysis of two large cohort studies that by reducing the amount of red/processed meat eaten a day by half, to around 42g, 9.3% of deaths in men and 7.6% of deaths in women could be prevented. This same research found a dose-response relationship between red meat intake and all-cause mortality, which is a good basis to recommend cutting down consumption. Graph to show dose-response relationship between red meat intake and mortality. Reproduced with permission from Pan A[19] The EPIC study48 looked at meat consumption and mortality across 10 European countries, considering a very heterogeneous diet across a large sample size. It found no statistically significant associations between red meat intake and CVD, but concluded that Europeans consuming high amounts of processed meat are at an increased risk of an early death, especially due to CVD. Furthermore, it was estimated that 3.3% of deaths could be prevented if these men and women ate less than 20g of processed meat a day. Current government guidelines47 don’t reflect this advice, as they don’t highlight that processed meat is considered to have a greater negative impact on health11,19,48,49 than unprocessed red meat in their dietary recommendations. However, it is important to take into consideration other confounding factors when looking at complex disease processes such as those involved with CVD. Men and women with a higher intake of red meat are more likely to be current smokers, to drink alcohol and to have a higher BMI. They are less likely to consume fruits and vegetables and to be physically active 19,48. All of the above are key determinants in the risk of developing cardiovascular disease50,51,52. This could imply that in fact red/processed meat consumption is not a significant risk factor in the development of CVD, but rather a confounding factor of another variable. Researchers adjusted data to eliminate the aforementioned confounding variables11,19, 48,51 but these statistical adjustments may not be significant enough. For example, a low socioeconomic status is associated with eating more processed foods and fattier, cheaper cuts of meat 53. It is also strongly associated with increased prevalence of smoking54, obesity55 and lower consumption of fruits and vegetables54. Therefore it could be the case that the trends between red/processed meat consumption and CVD are actually due to the overarching factor of socioeconomic status. Table to show cardiometabolic risk factor hazard ratio between vegetarian and nonvegetarian adventists. Reproduced with permission from Le LT[57] To work around this, we can look at studies of populations with very similar health behaviours, with meat intake being one of the only significant variables. Epidemiological study of Adventists, a Christian denomination, allows one such opportunity, as the Church doctrine places a strong emphasis on healthy living, including abstinence from tobacco and alcohol 56. Vegetarianism is also encouraged by the Church, with around 50% of Adventist members following a vegetarian diet and the rest following a diet similar to the rest of the western population57. One review of three large Adventist Cohorts found that vegetarians had greatly reduced risks of developing hypertension, type-2 diabetes, metabolic syndrome and obesity which can explain why in all three cohorts analysed, vegetarians had 26% to 68% lower risks of mortality from ischaemic heart disease, CVD, and cerebrovascular disease57. These figures were significant even having been adjusted for age, sex, smoking status, race, educational level, alcohol and other factors related to CVD. These results back up the epidemiological and pathophysiological evidence we have previously reviewed – that reduction in consumption of meat is cardio-protective. Another study analysing mortality between vegetarians and nonvegetarians found that vegetarians had an ischemic heart disease death rate ratio of 0.78 compared to non-vegetarians, and that even ‘semi-vegetarians’ (those who ate fish only or meat less than once a week) had a death rate reduction of 0.66 implying that a reduction in meat consumption is still beneficial, if not as good as abstinence. Benefits When considering how much red meat to consume you must not only look at the detrimental effects but also the benefits. Red meat is nutritional and a source of vitamins and minerals that are essential to health. A 100g portion of raw ground beef contains 36%, 29% and 84% of your Vitamin B3, B6, and B12 recommended daily nutrient intakes (RNIs) respectively. It also provides 20% of your Iron, 66% of your Zinc and 28% of your Selenium RNIs.58 Red meat is a better source of haem iron than either poultry or fish, and also more bioavailable than non-haem iron from plant sources. Iron-deficiency anaemia is a major nutritional problem affecting high and low socioeconomic populations worldwide.59 Red meat is also the largest source of Vitamin B12 in the diet with just 100g supplying nearly your entire daily-recommended intake. The methylation cycle occurs in all cells in the body and it requires adequate levels of B12 as well as B6 and folate. Without these nutrients the enzymes cannot function properly leading to increased levels of homocysteine – a risk factor for cardiovascular disease and stroke. So in moderation red meat can have protective effects.59 CONCLUSION Upon reviewing the evidence, we believe that unprocessed lean red meat consumption, in moderation, is not a risk factor for cardiovascular disease and is an important dietary source of protein and nutrients. We came to this conclusion as there is not enough evidence associating unprocessed red meat with cardiovascular disease, particularly when consumed in moderate quantities as part of a balanced diet. However, the same cannot be said of processed red meat, which has much evidence linking it to CVD. Whether there are safe limits to processed red meat intake is controversial, but from the studies we have reviewed we can conclude that there are great benefits to reducing consumption to low levels, although complete abstinence from processed red meats appears to be more cardio-protective still. What is obvious is that the health properties of processed and unprocessed meats are vastly different, and that it is an important public health issue that government guidelines should be updated to advise people more accurately on healthy food choices. We found multiple limitations and inconsistencies across the literature, which could have an impact on the validity of their results and be the cause of current conflicting information. Studies regularly didn’t monitor cooking methods, fat content of different cuts of meat or degree of fat trimming and, as discussed, dietary fat has a large impact on CVD risk. There were inconsistencies in how studies classified processed and unprocessed meat and data collection was usually by selfreported questionnaire – a method notorious for the introduction of bias. There is also a lack of studies focusing solely on lean unprocessed red meat. Furthermore, confounding variables are numerous and important when considering both CVD and diet, as we have previously discussed, and studies may not have taken accounted for these accordingly. Further research in this area is needed in order to clarify how cardio-protective reducing red and processed meats may be, ideally in the form of large clinical trials where a prescribed diet is monitored and followed up over a long period of time. PROJECT DIARY Week 1 This was the first time the group met with Ms Bahor and so the purpose of the meeting was to brain storm ideas of where we wanted to take the project. Ms Bahor had deliberately left the project description vague so that we could control it from the start. We narrowed the ideas down to “diet’s of the world” or the “effect of red meat in the diet”. With little prior knowledge in the group we opted to go away and research these topics over the following week to make an informed decision about what topic to take on. Week 2 In our second meeting, we discussed that although that many of the topics we spoke about last week were interesting, such as the health benefits of the Mediterranean diet, or Vegan vs Vegetarian Vs Omnivorous diet, we needed to focus on something more specific for our project. Many of us had looked specifically at the possible harmful effects of red meat so we decided to follow this route. We thought this would be a good topic as it was specific, with plenty of primary research in many areas relating to red meat, may be linked to heart disease, or how supposedly animal proteins from food can ‘switch on’ cancer promoters such as IGF-1. Because of this we decided not to narrow our research to one disease, but rather for now look at the many harmful effects that eating red meat ma cause. Week 3 A lot of the studies looked at the difference between consuming processed and unprocessed red meat and so we thought it was important to explore the difference between the two. Potential health effects include looking at CVD, hypertension, stroke, cancer, diabetes. We also should also look at the mechanism of consuming red meat on ONE of these diseases. Probably focus on cardiovascular and cancer then include a small section about additional diseases that have been seen to be linked with red meat consumption. Everyone gave a short summary of their article and everything is going on the right track: diabetes, hypertension, CHD, pancreatic cancer, bowel cancer, stomach and liver cancer, stroke and type 2 diabetes were explored in these articles. Week 4 In this meeting, we decided to consolidate the objectives of our project. We also decided to focus on the effects of red meat consumption on cardiovascular health and not cancer. Our finalised aim is: To investigate the potential detrimental effects of eating both processed and unprocessed red meat on cardiovascular health. We came up with several ideas for objectives: • To look into the mechanism of red meat (processed and unprocessed) on CV health. • To look at the substances that differentiate processed and unprocessed red meats and their differing effects on CV health. • Red meat consumption and CV health in different cultures and westernisation • Cooking method and redness of the meat • To look at other diseases that red meat has been demonstrated to have a negative effect on • To think about the future – should we stay away from processed red meat altogether? Compare normal diet to vegetarianism • To see if we there should be a daily limit to red meat consumption. • To look at other risk factors of CV health and red meat consumption e.g. socioeconomic group, age, smokers, alcohol (processed meat is cheaper) Conor would also write the critical appraisal for the group, but we would all make contributions after the presentations next week. Week 5 We continued with members presenting their critical appraisals. Then went onto discuss these themes: Physiological mechanisms, processed vs unprocessed, westernisation of diets and should we avoid meat altogether. Week 6 Lucy and Kerr presented their informal critical appraisal. We discussed how everybody was feeling in regards to the delegation of parts of the essay. We spoke about what we had written over the past week and explained certain bits of it and what our plans were to achieve in the coming week. Izzy explained advanced glycation end products. Amy explained the mechanisms of process meats leading to cardiovascular problems. For next week we are to continue our parts of the essay, to feedback to the group in the next session. Week 7 Amy and Jacqueline presented their critical appraisals Planned to all read Connor’s paper this week so we can point out anything we think he has missed or things we want to query about his critical appraisal when he presents it next week James read out his section on epidemiology, risk factors and mechanisms of cardiovascular disease. Jobs still to do: • Conclusion • Critical appraisal • Collate references • Search history and search methods report • Put all together onto website • Contributions page • Order on website Essay outline – James – Background – Jacqueline – General mechanisms – Amy and Izzy – processed vs unprocessed mechanisms – Kerr – westernisations – Alice and Lucy – What is healthiest – Conclusion 2. 3. 4. Worked out we’re roughly on track for word count Complete sections and reference properly Everyone to put up their sections on to Facebook so we can all read and find out what overlaps/ what is missing Week 8 This week: Alice presented her critical appraisal on a paper about meat and fat intake as risk factors for pancreatic cancer. Conor also presented his critical appraisal, but as his paper will be the group’s critical appraisal, we asked him the relevant questions and gave him feedback, rather than our tutor. James has nearly finished the introduction and no one had any improvements that they thought should be made to the conclusion. For next week: 3. We will collate our references and Alice will check that it is all done properly. 4. We will all read and comment on each others sections. 5. We will email the relevant organisations and people about being able to use their diagrams in our project. We aim to be finished by the next meeting on Monday. CONTRIBUTIONS • James Hazelwood’s role was to do most of the research of background knowledge for this project. He wrote the ‘background knowledge’ page on the epidemiology of CHD, pathophysiology of CHD and UK recommendations of meat consumption. • Amy Walter researched the differences in processed and unprocessed red meat and their different health effects on the cardiovascular system. She looked at the addition of preservatives during processing, which mainly included sodium and nitrate compounds. Also, along with Izzy Utting, Amy wrote the search report. • Alice McKinnes researched government guidelines on red/processed meat intake, vegetarian vs none vegetarian diets, and epidemiological evidence on what, if any, amounts of red meat are safe to consume. Also collated the • • • • • references and, along with Lucy Dobbs, wrote the conclusion. Lucy Dobbs researched the long term effects of eating red meat and wrote part of the how much red meat, if any, is safe? She also wrote the conclusion in conjunction with Alice McKinnes. Izzy Utting researched processed red meat and the mechanisms by which it causes detrimental cardiovascular health effects. Looked further into advanced glycation end products and wrote this part of the website. She also cowrote the search report with Amy Walter. Izzy was the creative genius behind the drawing designs. Kerr Hartop researched the evolution of the western diet and comparisons of our diet effects on health to other cultures around the world. Jacqueline Quinn helped to research effects of meat on the cardiovascular system and wrote the section on the mechanisms of eating red meat resulting in poor health. Conor Rankin edited the website, putting together the pages from the other members. He also wrote the critical appraisal appendix, organised the project diary and wrote the contributions page. CRITICAL APPRAISAL Mediterranean diet and CHD: the Greek European Prospective Investigation into Cancer and Nutrition Cohort Aims: • To investigate the association of adherence to the Mediterranean diet (MD) with cardiovascular disease (CVD) incidence, • Assess the morality in the ‘Greek European Prospective Investigation into Cancer and Nutrition cohort’ (GEPIC). Population: The study used a cohort of volunteers aged 20-86 recruited between 1994-1999 from all over Greece, with data being collected until 2009. Study Design: Cohort-study Study Size: 23929 adult men and women without CVD or cancer at enrollment. Statistical Tests: This study used a cox regression to evaluate the effect of several variables on the time it takes for CHD to develop and the results showed adherence to MD leads to a statistically significant (p=0.003) reduction in morality. Outcome Measure: The study measured the number of participants developing coronary heart disease (CHD) and morality of CHD in relation to MD. This was an appropriate measurement as the cohort study allowed a inverse causal association to be formed between a MD and CHD. Main Results: 636 participants (426 male and 210 female) developed CHD, among them 240 died. There was a dose response pattern with higher adherence to MD inversely associated with a reduction in CHD morality – a two point increase in MD score leads to a CHD morality reduction by 19% in males and 25% in females. There was also an association of traditional risk factors (obesity, smoking and old age) with CHD and death. Sources of Bias: There are several potential biases that could have adversely affected this study: (i) Recall bias as patients had to fill in the food frequency questionnaire (FFQ) retrospectively with their dietary habits and this could tend to the null, people are more likely to underreport their health damaging behaviours. This is confirmed by the study as women have a stronger inverse association of MD and CHD, possibly due to women having a better recollection and more accurate reporting; (ii) Follow up data was collected by interview which gives rise to observation bias, any participants who develop CHD could be probed for answers to match the expected hypothesis. Strengths: • The study design allowed a causal link to be established between the MD and CHD as CHD was measured using incidence (diagnosis during the study) over prevalence. The study excluded subjects with prevalent cardiac disease or cancer and any participate without follow up data to reduce bias. • With 23,929 participants, the GEPIC is a large study making the results more reliable. Furthermore there are slightly more females than males in the study which is representative of the population. Weaknesses: 5. The authors of this study found a correlation between males eating meat and CHD however they do not distinguish between different types of meat, particularly processed and non-processed meat, which could have different effects on health. 6. Data was collected by follow up interview, which isn’t completely reliable as variation between interviewers could have resulted in bias. 7. The study did take into consideration and adjust for some confounding factors such as education level but didn’t take into account others such as cooking methods, e.g. frying food in butter, which increase the risk of CHD. Conclusion: We as a group, feel that the study design and the results identified make it a valid study. The authors addressed the aims confirming that adhering to the MD has an inverse association with CHD and that other health damaging behaviours also contribute. Although there were some sources of bias they did not affect the reliability of the results as the sample size was so large. MD and CHD Paper INFORMATION SEARCH REPORT An unhealthy diet is considered a major risk factor for many diseases. There has been recent interest in the news and several hypotheses suggest that red meat consumption has a particular detrimental effect on health. In order to get an overview of this topic, we watched the documentary “World’s Best Diet”, which allowed us to enhance our understanding of the different global diets and their correlation with the general health of the nation. We decided to examine this relationship further and looked at several studies that showed a significant relationship between red meat intake and cancer, diabetes and CVD. We used a wide range of online databases, including Google Scholar, PubMed, and particularly Ovid MEDLINE, on which we carried out a MeSH search. In order to narrow our research, we focused specifically on the effects and mechanisms of red meat on cardiovascular health. We looked at a combination of meta-analyses and primary research articles, which focused on certain aspects of CVD such as hypertension, stroke and coronary heart disease. Vegetarian and Seventh-day Adventist diets were also of particular interest to us, especially in connection to the incidence of CVD. The meta-analyses were useful for comparing large and diverse populations. The key words we used in these searches included “red meat” or “processed meat”. We exploded “heart disease” in the MeSH search so that it would encompass all types of coronary heart diseases. We made the results more specific by combining “red meat” AND “heart disease” with the Boolean operator. When trying to access articles, it was often difficult to obtain the full text. The abstract was rarely sufficient for our depth of research and therefore this proved a problem in some cases. We overcame this by signing up to websites or using the university access login. REFERENCES References 1. NHS Choices. Coronary Heart Disease. [Online] Available from: http://www.nhs.uk/Conditions/Coronary-heartdisease/Pages/Introduction.aspx [Accessed 9th November 2014]. (Website). 2. World Health Organisation. The top 10 causes of death. [Online] Available at: http://www.who.int/mediacentre/factsheets/fs310/en/ [Accessed 9 Nov. 2014]. (Website – discusses the current and predicted causes of death across the world). 3. NHS Choices. Atherosclerosis. [Online] Available from: http://www.nhs.uk/Conditions/Atherosclerosis/Pages/Introducti on.aspx [Accessed 9 Nov. 2014]. (Website) 4. Newby D, Grubb N and Bradbury. Cardiovascular Disease. In Walker B, Colledge N, Ralston S and Penman I. (eds.) Davidson’s Principles and Practice of Medicine. Edinburgh: Churchill Livingston/Elsevier; 2014. p. 525—643. (Textbook- provides clinically relevant information on the pathophysiology of CVD) 5. Rosano G, Chierchia S, Leonardo F, Beale C and Collins P. Cardioprotective effects of ovarian hormones. Eur Heart J 1996; 17(suppl D):15-19. (Review article) 6. Burnett J. Lipids, lipoproteins, atherosclerosis and cardiovascular disease. Clin Biochem Rev 2004;25:2. (Review article) 7. Revest P. The cardiovascular system. In Naish J, Revest P, and Syndercombe Court D. (eds) Medical Sciences. Edinburgh: Saunders/Elsevier;2009. p. 571—641 (Textbook ) 8. Nicolosi R. Dietary fat saturation effects on low-density-lipoprotein concentrations and metabolism in various animal models. Am J Clin Nutr 1997;65(5):1617-1627. (Review article) 9. Holness M, Sudgen M and Naish J. Energy Metabolism. In Naish J, Revest P, and Syndercombe Court D. (eds.) Medical Sciences. Edinburgh: Saunders/Elsevier;2009. p. 89— 127 (Textbook) 10. Williams, P. Nutritional composition of red meat. Nutr Diet 2007;64(4):113-119. (Review article) 11. Micha R, Wallace S and Mozaffarian D. Red and Processed Meat Consumption and Risk of Incident Coronary Heart Disease, Stroke, and Diabetes Mellitus: A Systematic Review and Meta-Analysis. Circulation 2010;121(21):22712283. (Primary Research paper – systematic review and metaanalysis of the effects of red and processed meat on CVD risks) 12. Sinha R, Cross A, Graubard B, Leitzmann M and Schatzkin A. Meat Intake and Mortality. Arch Inter Med 2009;169(6):562. (Primary Research Paper – Cohort study examining the effects of red meat on health in the USA) 13. Koeth RA, Wang Z, Levison BS, Buffa JA, Org E, Sheeny BT, Britt EB, Fu X et al. Intestinal microbiota metabolism of Lcarnitine, a nutrient in red meat, promotes atherosclerosis. Nat Med 2013;19:578-585. (Primary research paper) 14. Wang Z, Klipfell E, Bennett BJ, Koeth R, Levison BS, DuGar B, Feldstein AE, Britt EB et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011;472:57–63 (Primary research paper) 15. Hayward Medical Communications. What is a cox model? http://www.medicine.ox.ac.uk/bandolier/painres/download/what is/cox_model.pdf (accessed 8th November 2014). (Website) 16. DiNicolantonio JJ, Lavie CJ, Fares H, Menezes AR and O’Keefe JH. L-carnitine in the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-analysis. Mayo Clin Proc 2013;88(6):544-551. (Review article) 17. Muñ0z-Bravo, Gutiérrez-Bedmar M, GómezAracena J, García-Rodríguez A and Fernández-Crehuet Navajas J. Iron: Protector or Risk Factor for Cardiovascular Disease? Still Controversial. Nutrients [Online] 2013;5:2384-2404. Available from: doi:10.3390/nu5072384. [Accessed 8th November 2014] (Review article) 18. Tzoulaki I, Brown IJ, Chan Q, Van Horn L, Ueshima H, Zhao L, Stamler J and Elliot P. Relation of iron and red meat intake to blood pressure: cross sectional epidemiological study. British Med J 2008;337:258 (Primary research paper) 19. Pan A, Sun Q, Bernstein AM, Schulze MB, Manson JE, Stampfer MJ et al. Red meat consumption and mortality; results from 2 prospective cohort studies. Arch Intern Med [Online] 2012;172(7):555-563. Available from: doi:10.1001/archinternmed.2011.2287 [Accessed 28th October 2014] (Primary research paper) 20. Micha R, Michas G, Lajous M and Mozaffarain D. Processing of meats and cardiovascular risk: Time to focus on preservatives. BMC Med 2013;11(136) (Primary research paper) 21. Blaustein M, Zhang J, Chen L and Hamilton B. How does salt retention raise blood pressure? Am J Physiol Regul Integr Comp Physiol 2006;290(3):514-23. (Review article) 22. Kaluza J, Akesson A and Wolk A. Processed and unprocessed red meat consumption and risk of heart failure: A prospective study of men. Circ Heart Fail [Online] 2014;7(4):552-7. Available from: doi: 10.1161/CIRCHEARTFAILURE.113.000921 [Accessed 14th November 2014] (Primary research paper) 23. Sheweita SA, EL-Bendery HA and Mostafa MH. Novel study on Nnitrosamines as risk factors of cardiovascular diseases. Biomed Res Int [Online] 2014:817019. Available from: DOI: 10.1155/2014/817019 [Accessed 14th November 2014] (Primary research paper) 24. Zanteson L. Advanced Glycation End Products. Today’s Dietician, 2014;16(3):10 (Review article) 25.Uribarri J et al. Advanced Glycation End Products in Foods and a Practical Guide to Their Reduction in the Diet. J Am Diet Assoc, 2010;110(6):911916 (Primary research paper) 26. Vlassara, H., Cai, W., Crandall, J., Goldberg, T., Oberstein, R., Dardaine, V., Peppa, M. and Rayfield E. J. (2002) ‘Inflammatory mediators are induced by dietary glycotoxins, a major risk factor for diabetic angiopathy’, Proceedings of the National Academy of Sciences of the United States of America, 99(24), pp. 15596– 15601. (Primary research paper) 27. Goldin A, Beckman JA, Schmidt AM and Creager MA. Advanced Glycation End Products: Sparking the Development of Diabetic Vascular Injury’, Circulation 2006;114:597-605. (Review article) 28. Bastaa G, Schmidt AM and De Caterinaa R. Advanced glycation end products and vascular inflammation: implications for accelerated atherosclerosis in diabetes. Cardiovasc Res 2004;63:582–592. (Review article) 29. Goh S and Cooper ME. The Role of Advanced Glycation End Products in Progression and Complications of Diabetes. Journal Clin Endocrinol Metabol, 2008;93(4):1143-1152. (Review Article) 30. Popkin B. The Nutrition Transition in the Developing World. Dev Policy Rev. 2003;21(5-6):581597. (Review article) 31. Cross A. Higher red meat consumption is associated with increased risk of all-cause, cardiovascular, and cancer mortality. Evid Based Nurs. 2012;15(4):121-122. (Primary research paper) 32. Odeegard AO. Western-Style Fast Food Intake and Cardiometabolic Risk in an Eastern Country. J Am Heart Assoc. 2012;126:182188. (Primary research paper) 33. Eaton SB, Konner M, Shostak M. Stone agers in the fast lane: Chronic degenerative diseases in evolutionary perspective. Am J Med. 1988;84(4);739-749. (Review article) 34. Kagawa Y. Impact of westernization on the nutrition of Japanese: Changes in physique, cancer,longevity and centenarians. Prev Med. 1978;7(2):205-217. (Primary research paper) 35. Bersamin A, Luick BR, King IB, Stern JS, Zindenberg-Cherr S. Westernizing Diets Influence Fat Intake, Red Blood Cell Fatty Acid Composition, and Health in Remote Alaskan Native Communities in the Centre for Alaska Native Health Study. J Am Diet Assoc. 2008;108(2):266-273. (Primary research paper) 36. Bhf.org.uk. British Heart Foundation – Blood pressure [Online] 2014 [cited 4 November 2014]. Available from: http://www.bhf.org.uk/research/heart-statistics/riskfactors/blood-pressure.aspx 37. McMichael A, Bambrick H. Meat consumption trends and health: casting a wider risk assessment net. Public Health Nutr. 2005;8(04) (Editorial Comment) 38. Wood JD et al. Effects of fatty acids on meat quality: a review. Meat Sci. 2004;66(1):21-32 (Review article) 39. Bernstein AM, Sun Q, Hu FB, Stampfer MJ, Manson JE, Willet WC. Major Dietary Protein Sources and Risk of Coronary Heart Disease in Women. Circulation. 2010;122(9):876-883 (Primary research paper) 40. McAfee A, McSorley E, Cuskelly G, Moss B, Wallace J, Bonham M et al. Red meat consumption: An overview of the risks and benefits. Meat Sci. 2010;84(1):1-13. (Review article) 41. Mcmichael A. Bovine spongiform encephalopathy: its wider meaning for population health. BMJ. 1996;312(7042):13131314. (Editorial comment) 42. Menotti A, Kromhout D, Blackburn H, Fidanza F, Buzina R and Nissinen A. Food intake patterns and 25-year mortality from coronary heart disease: Cross-cultural correlations in the Seven Countries Study. Eur J Epidemiol 1999;15:507–515. (Primary Research Paper) 43. Fung T, Stampfer M, Manson J, Rexrode K, Willett W, Hu F. Prospective Study of Major Dietary Patterns and Stroke Risk in Women. Stroke. 2004;35(9):2014-2019. (Primary Research Paper) 44. Fraser, G. Associations between diet and cancer, ischemic heart disease, and all-cause mortality in non-Hispanic white California Seventh-day Adventists. Am J Clin Nutr 1999;70(3):532S–538S. (Primary Research Paper) 45. Kontogianni MD et al. Relationship between meat intake and the development of acute coronary syndromes: the CARDIO2000 case–control study. Eur J Clin Nutr 2007;62(2):171–177. (Primary Research Paper) 46. Harvard Health. Cutting red meat-for a longer life – Harvard Health Publications [Online]. 2012 [cited 20 October 2014]. Available from: http://www.health.harvard.edu/newsletters/Harvard_Mens_Heal th_Watch/2012/June/cutting-red-meat-for-a-longerlife (Review Article) 47. Department of Health. Red Meat Link to Bowel Cancer [Press Release] 3rd May 2012. Available at: http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/ mediacentre/pressreleases/dh_124670 [Accessed 26th October 2014] (Website) 48. Rohrmann S, Overvad K, Bueno-deMesquita HB, Jakobsen MU, Egeberg R, Tjjønneland A et al. Meat consumption and mortality – results from the European Prospective Investigation into Cancer and Nutrition. BMC Med [Online] 2013;11:63. Available from: doi: 10.1186/1741-701511-63 [Accessed 28th October] (Primary Research Paper) 49. Binnie MA, Barlow K, Johnson V and Harrison C. Red meats: Time for a paradigm shift in dietary advice. Meat Sci [Online] 2014;98(3):445-451. Available from: DOI: 10.1016/j.meatsci.2014.06.024 [Accessed 3rd November 2014] (Review Article) 50. Lim SS, Vos T, Flaxman A, Danaei G, Shibuya K, Adair Rohani H et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet Glob Health [Online] 2014;384(9954):1549-1640. Available from: http://ac.els-cdn.com/S0140673612617668/1s2.0-S0140673612617668-main.pdf?_tid=c5f2abac-63a0-11e4be9a00000aab0f01&acdnat=1415050469_19baec7c81cf5b6c336460 5528ffc8c0 [Accessed 3rd November 2014] (Primary Research Paper) 51. Wang X, Ouyang Y, Liu J, Zhu M, Zhao G, Bao W and Hu FB. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. Br Med J [Online] 2014;349:g4490. Available from: Doi: 10.1136/bmj.g4490 [Accessed 3rd November 2014] (Primary Research Paper) 52. Lavie CJ, Milani RV and Ventura HO. Obesity and cardiovascular disease: risk factors, paradox, and impact of weight loss. J Am Coll Cardiol [Online] 2009;53(21):1925-32. Available from: doi: 10.1016/j.jacc.2008.12.068. [Accessed 3rd November 2014] (Primary Research Paper) 53. Darmon N and Drewnowski A. Does social class predict diet quality? Am J Clin Nutr [Online] 2008;87(5):1107-1117. Available from: http://ajcn.nutrition.org/content/87/5/1107.full [Accessed 3rd November 2014] (Review Article) 54. Hiscock R, Bauld L, Amos A and Platt S. Smoking and socioeconomic status in England: the rise of the never smoker and the disadvantaged smoker. J Public Health[Online] 2012;34(3):390-396. Available from: doi: 10.1093/pubmed/fds012 [Accessed 3rd November 2014] (Primary Research Article) 55. McLaren L. Socioeconomic status and obesity. Epidemiol Rev [Online] 2007;29(1):29-48. Available from: doi: 10.1093/epirev/mxm001 [Accessed 3rd November 2014] (Review Article) 56. Butler TL, Fraser GE, Beeson WL, Knutsen SF, Herring RP, Chan J et al. Cohort profile: The Adventist Health Study-2 (AHS-2) Int. J. Epidemiol [Online] 2008;37:260–265. Available from: doi: 10.1093/ije/dym165. [Accessed 3rd November 2014] (Primary Research Article) 57. Le LT and Sabate. Beyond meatless, the health effects of vegan diets: findings from the Adventist cohorts. Nutrients [online] 2014;6(6):2131-2147. Available from: doi: 10.3390/nu6062131 [Accessed on 3rd November] (Primary Research Article) 58. Self Nutrition Data. Nutrition Facts and Analysis for Beef, variety meats and by-products, spleen, cooked, braised [Online]. 2014 [accessed 7 November 2014]. Available from: http://nutritiondata.self.com/facts/beefproducts/3477/2 (Website) 59. McAfee A, McSorley E, Cuskelly G, Moss B, Wallace J, Bonham M et al. Red meat consumption: An overview of the risks and benefits. Meat Science. 2010;84(1):1-13. (Review Article)