Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
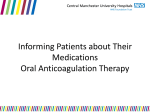
BASIC AND PATIENT-ORIENTED RESEARCH J Oral Maxillofac Surg 65:1454-1460, 2007 Dentoalveolar Procedures for the Anticoagulated Patient: Literature Recommendations Versus Current Practice Brent B. Ward, DDS, MD,* and Miller H. Smith, DDS† Purpose: To evaluate the current practice of oral and maxillofacial surgeons in Michigan regarding perioperative warfarin therapy and dentoalveolar surgery in defined procedure risk groups. Materials and Methods: Surveys were distributed to all surgeons (n ⫽ 188) registered with the Michigan Society of Oral and Maxillofacial Surgeons. Low/moderate/high surgery risk groups were defined based on retrospective data accumulated for procedures on pretransplant liver failure patients. We requested the surgeon’s maximum tolerated International Normalized Ratio (INR) for each risk group. In addition, surgeons were asked if their routine practice for each group included continuation or discontinuation of therapeutic warfarin perioperatively. Results: A 72.6% response rate was achieved. The average maximum INR cutoff values for the various risk groups were: low, 2.68; moderate, 2.28; and high, 2.01. Routine discontinuation of warfarin occurred in these groups 23.6%, 48.8%, and 70.5%, respectively. Using a paired t test, these results showed statistically significant differences in patient management practices (P ⬍ .001) between the low, moderate, and high risk groupings. Conclusion: Lack of uniformity exists regarding warfarin therapy and dentoalveolar surgery. No studies to date involve significant numbers of moderate/high risk procedures to provide evidence-based support of safety with maintenance of therapeutic INR. For moderate or high risk procedures, the majority of surgeons prefer warfarin discontinuation with minimally therapeutic or subtherapeutic levels, a practice that secondarily increases risk for thromboembolism. Based on these preliminary data, we believe a prospective trial to elucidate stronger management guidelines for both the moderate and high risk surgery population is indicated. © 2007 American Association of Oral and Maxillofacial Surgeons J Oral Maxillofac Surg 65:1454-1460, 2007 Warfarin sodium was accepted for use as an anticoagulant in 1954.1 Since this time significant controversy in the surgical community has evolved regarding the risks and benefits of continuing versus cessation of this medication before surgical procedures.2-7 The medical and dental communities have Received from the Department of Surgery, Section of Oral and Maxillofacial Surgery, University of Michigan, Ann Arbor, MI. *Assistant Professor and Program Director. †Resident. Address correspondence and reprint requests to Dr Ward: University Hospital, 1500 E Medical Center Dr, Ann Arbor, MI 481090018; e-mail: [email protected] © 2007 American Association of Oral and Maxillofacial Surgeons 0278-2391/07/6508-0004$32.00/0 doi:10.1016/j.joms.2007.03.003 contributed a wide variety of perioperative management recommendations regarding the maintenance or modification of warfarin before oral surgical procedures because of a high risk of bleeding.8-18 Serious thromboembolic events as well as fatalities have been reported following prolonged discontinuation of warfarin in patients requiring anticoagulation.10,19-21 Therefore, practitioners have sought alternatives to interruption of warfarin therapy such as bridging therapy, using intravenous heparin, or subcutaneous low molecular weight heparin to minimize the interval without anticoagulation.2,3,7,22-24 Multiple case reports and systematic reviews can be found in the literature supporting the continuation of warfarin before oral surgical procedures, assuming that the prothrombin time (in seconds) or the PT ratio remains within a certain range.20,25-42 The develop- 1454 1455 WARD AND SMITH ment of anticoagulant standardization with the international normalized ratio (INR)43-47 and analysis of outcomes data by the American Heart Association/ American College of Cardiology,48,49 European Society of Cardiology,50-52 and British Committee for Standards in Hematology,53,54 have aided in minimizing adverse bleeding sequelae for those patients on warfarin. It is clear that before INR standardization, individuals in the past were anticoagulated to a higher degree, especially in North America where a less sensitive thromboplastin was used.55 Monitoring regimens56-62 and therapeutic anticoagulation48,49 has continued to evolve, with resulting improvement in patient safety.45 Recently, investigations with or without the use of topical procoagulant agents63-68 have shown the relative safety of continuing warfarin at therapeutic levels while undertaking certain oral surgical procedures.65,69-87 The definition of the complexity of a procedure varies between patients and practitioners alike, and only recently has risk stratification for postoperative bleeding in oral surgical procedures been attempted using retrospective data from pre-transplant liver failure patients.88 It is evident that most of the current literature supports continuation of warfarin for minor oral surgical procedures, up to 3 to 5 teeth, while the patient remains in a therapeutic range of anticoagulation. To accurately assess how risk of procedure changes the surgeon’s treatment of patients on warfarin, we surveyed the State of Michigan Oral and Maxillofacial Surgeon (OMFS) community to determine their practice habits with anticoagulated patients in various stratified risk groups. Materials and Methods SAMPLE A survey questionnaire was distributed twice to all 188 OMFS registered with the Michigan Society of OMFS in July 2005. Anonymous prepaid postage return envelopes were provided. The surveys were numbered for the sole purpose of preventing duplication of data entry. The individual respondents were never identified with their answers. SURVEY A 2-part questionnaire was developed to allow for simple data acquisition. The questions were as follows: 1) Please indicate the maximal INR you would tolerate for performing procedures in the following groups of patients on warfarin therapy (provided to the nearest 0.5 INR value) - Low risk (1-5 simple ext) - Moderate risk (6-10 simple extractions, 1 impacted extraction, 1 quadrant alveolectomy) FIGURE 1. Maximal INR distribution for low risk dentoalveolar procedures. Ward and Smith. Dentoalveolar Surgery in Anticoagulated Patients. J Oral Maxillofac Surg 2007. - High risk (⬎10 simple extractions, ⬎2 impacted extractions, ⬎2 quadrants alveolectomy, tori removal) 2) Do you routinely discontinue/continue warfarin oral anticoagulant therapy before low/moderate/high risk dentoalveolar surgery? STATISTICAL ANALYSIS Numerical data were entered onto and analyzed using SPSS software (SPSS Inc, Chicago, IL). Frequencies for each question were tallied and investigated for significance using a paired t test (P ⬍ .05). Results All 188 surgeon members of the Michigan Society of OMFS received an initial mailing followed by a duplicate second mailing 2 weeks later. Fifteen of the surgeons were excluded because of retirement or incorrect address. One hundred twenty-seven surveys were returned for data collection for an overall response rate of 72.8%; however, 4 surveys were excluded. Three because of incomplete information, and 1 respondent returned both surveys with the same information. Mean maximal INR values for low, moderate, and high risk surgical procedures were 2.68, 2.28, and 2.01, respectively. Figures 1 through 3 provide frequency distribution of maximum tolerated INR values for each risk grouping. All distributions were statistically significant (P ⬍ .001) for the various risk groups. INR levels below 2.0 were noted 25.2% of the time for low risk, 50.4% for moderate risk, and 66.7% for high 1456 DENTOALVEOLAR SURGERY IN ANTICOAGULATED PATIENTS FIGURE 2. Maximal INR distribution for moderate risk dentoalveolar procedures. FIGURE 4. Warfarin usage before low risk dentoalveolar procedures. Ward and Smith. Dentoalveolar Surgery in Anticoagulated Patients. J Oral Maxillofac Surg 2007. Ward and Smith. Dentoalveolar Surgery in Anticoagulated Patients. J Oral Maxillofac Surg 2007. risk procedures. Routine discontinuation of warfarin for low, moderate, and high risk procedures was indicated 23.6%, 48.8%, and 70.5% of the time respectively (Figs 4-6). The practice of discontinuing warfarin was statistically significant for each of the procedure risk groups (P ⬍ .001). In patients requiring anticoagulation, INR values are maintained within a therapeutic range set forth by recommendations provided by various anticoagulation committees. An INR range between 2.0 to 3.0 is deemed appropriate for patients at risk for arterial and venous thrombosis.48-54,89 An INR range from 2.5 to either 3.5 or 4.0 is advocated for mechanical heart valves by American Heart Association/American College of Cardiology48,49 and European Society of Cardiology/British Committee for Standards in Hematology50-54 recommendations, respectively. An INR above this range may increase the patient’s risk for a FIGURE 3. Maximal INR distribution for high risk dentoalveolar procedures. FIGURE 5. Warfarin usage before moderate risk dentoalveolar procedures. Ward and Smith. Dentoalveolar Surgery in Anticoagulated Patients. J Oral Maxillofac Surg 2007. Ward and Smith. Dentoalveolar Surgery in Anticoagulated Patients. J Oral Maxillofac Surg 2007. Discussion WARD AND SMITH FIGURE 6. Warfarin usage before high risk dentoalveolar procedures. Ward and Smith. Dentoalveolar Surgery in Anticoagulated Patients. J Oral Maxillofac Surg 2007. spontaneous or surgically induced bleeding episode,90 while an INR below the desired therapeutic level increases the risk for thromboembolism19,91 and ischemic cerebrovascular event.21,92 A recent investigation at our institution monitored surgical complications in pretransplant liver failure patients. This study showed that postoperative bleeding episodes are dependent on the complexity of the dentoalveolar procedures performed, and a significant variation exists between low and high risk procedure groups.88 It cannot be assumed that a direct correlation exists between patients with warfarin anticoagulation and those with liver failure who present with a variety of coagulopathic concerns. Yet retrospective analysis in the liver failure population led to the realization that surgeons consistently placed patients into risk categories based on the number of extractions to be preformed. This evidence caused us to question the current practice and evidence for extensive dentoalveolar procedures in the warfarinized patient population. A comprehensive evaluation of the literature was accomplished in an effort to identify management recommendations based on the risk categories similar to the liver failure study. The majority of publications on warfarin and dentoalveloar surgery argue that no increased risk of postoperative bleeding episodes exists in the surveyed low risk group (1 to 5 simple extractions).20,25,30,32,75,76,79-82,93 A number of reported studies and review articles state that dentoalveolar procedures, even within our moderate and high risk groupings, can be offered without discontinuing warfarin.2,25,81 However, careful evaluation of this litera- 1457 ture shows that the actual procedures were most appropriately classified as low risk procedures and very few reports described treatment within the moderate or high risk categories.25,81 For example, Devani et al81 concluded that dental extractions could be completed safely without modification of warfarin therapy in 33 patients. Review of these data showed that a range of 1 to 9 teeth were extracted in the patients with an average of 2.1 teeth in the treatment group and 2.0 teeth in the control group. None of these patients would qualify for our high risk category, and only a select few would likely qualify for the moderate risk group. Blinder et al77 evaluated for the frequency of postoperative bleeding in patients at various INR levels, concluding that an INR value within the therapeutic range did not effect postoperative bleeding. These investigators concluded that dental extractions could be completed in patients without interruption or diminution of warfarin. Review of their data shows that patients in their therapeutic INR groups received on average 2.06 extractions. Wahl’s2 comprehensive and systematic review sought to evaluate the risks of thromboembolic stroke from discontinuation of anticoagulant medication versus the risk of serious life-threatening postoperative bleeding with therapeutic warfarin. More than 2,014 surgical procedures were reviewed without alteration of warfarin and concluded that severe postoperative bleeding not controlled with local measures is rare and often corresponds with supratherapeutic anticoagulation. Meanwhile, 4 patients experienced fatal embolic complications following withdrawal of their medication. It was then acknowledged that “many authorities state that dental extractions can be performed with minimal risk at or above therapeutic levels of anticoagulation.”2 Regardless, in this report an overall average of 2.60 extractions per patient were performed, well under what would be deemed high risk dentoalveolar procedures. Interestingly, the only study evaluating patients undergoing more than 10 extractions was completed by Bailey et al25 in 1983. This report evaluated the continuation of warfarin therapy in 25 patients and compared these data with non-anticoagulated age-matched controls. The number of extractions in patients in the treatment arm ranged from 1 to 20 teeth, with an average of 6.24 teeth.25 The investigators surmised that extractions with therapeutic anticoagulation could be accomplished and any postoperative bleeding could be easily managed using a specific protocol. It is interesting that 75% of patients (3 out of 4) with 10 or more extractions were recorded as having late postoperative bleeding scores. One may interpret the literature inappropriately and assume there is adequate evidence supporting extraction of any number of teeth in anticoagulated patients; however, in our es- 1458 timation, the paucity of prospective or retrospective data on patients receiving more than 5 extractions and/or other invasive dentoalveolar procedures does not provide adequate information to evaluate the safety for all daily outpatient treatment. Our study shows that there exists a significant disparity regarding patient management among OMFS for various risk-stratified dentoalveolar surgical procedures in warfarin anticoagulated patients. It was surprising to see that more than 23% of surgeons routinely discontinued warfarin for low risk procedures. The literature supports that the completion of low risk dentoalveolar procedures is safe if INR values, or similarly past use of PT-ratios, are in a therapeutic range.20,25,30,32,75,76,79-82,93 Bleeding episodes are noted to occur in both experimental and control groups, and are often adequately controlled using local measures only.32,36,80,82,94 Rarely, reversal of anticoagulation is warranted, and most often hemorrhage is caused by supratherapeutic levels of warfarin.30,32,95-98 In addition, trials evaluating the effectiveness of anticoagulant or antifibrinolytic99 products have shown significant benefit in avoiding postoperative bleeding episodes in patients taking warfarin.69-74,83,84 Studies have shown that aggressive local management using local anesthetic with vasoconstrictors, curettage of periodontally compromised teeth, placing absorbable gelatin or oxidized cellulose materials, obtaining primary closure with sutures, and avoidance of unnecessary antibiotics postoperatively can aid in preventing postoperative hemorrhage.77,80,81,100 Based on the current survey results, the majority of patients are purposely subtherapeutic with respect to warfarin levels at the time of surgery for moderate (50%) and high risk (67%) procedures. This practice may be justifiable given the lack of data in the literature for higher risk procedures. Bridging therapy with administration of intravenous anticoagulation in a hospital setting101 or intramuscular or subcutaneous anticoagulation in an outpatient setting have been attempted to minimize the time spent at inadequately anticoagulated levels100,102-106; however, these strategies may not be cost effective,107,108 and have their own associated risks.109 Overall, a lack of uniformity exists regarding literature recommendations for warfarin and dentoalveolar surgery and the current practice of OMFS. It is evident that trends in the literature point to the ability to continue warfarin in therapeutic ranges for dentoalveolar surgery procedures; however, data are lacking throughout moderate and higher risk groups, as we have defined them, and further investigation through randomized trials is necessary. Based on these data, we are presently moving forward with a protocol for a prospective trial that we hope will create guidelines DENTOALVEOLAR SURGERY IN ANTICOAGULATED PATIENTS specifically for the moderate and high risk dentoalveolar surgery populations with therapeutic anticoagulation levels. Acknowledgment The authors thank Dr Joseph Helman for his guidance, and the Michigan Society of Oral and Maxillofacial Surgeons for their support. References 1. Young KM: Laboratory medicine: The history of warfarin. Vet Clin Path 34:76, 2005 2. Wahl MJ: Dental surgery in anticoagulated patients. Arch Intern Med 158:1610, 1998 3. Wahl MJ: Myths of dental surgery in patients receiving anticoagulant therapy. J Am Dent Assoc 131:77, 2000 4. Carter G, Goss AN, Lloyd J, et al: Current concepts of the management of dental extractions for patients taking warfarin. Aust Dent J 48:89, 2003 5. Jeske AH, Suchko GD: Lack of a scientific basis for routine discontinuation of oral anticoagulation therapy before dental treatment. J Am Dent Assoc 134:1492, 2003 6. Herman WW, Konzelman JL Jr, Sutley SH: Current perspectives on dental patients receiving coumarin anticoagulant therapy. J Am Dent Assoc 128:327, 1997 7. Dios PD, Feijoo JF: Tooth removal and anticoagulant therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92:248, 2001 8. Ziffer AM, Scopp IW, Beck J, et al: Profound bleeding after dental extractions during dicumarol therapy. N Engl J Med 256:351, 1957 9. Scopp IW, Fredrics H: Dental extractions in patients undergoing anticoagulant therapy. Oral Surg Oral Med Oral Pathol 11:470, 1958 10. Tulloch J, Wright IS: Long-term anticoagulant therapy: further experiences. Circulation 9:823, 1954 11. Mulligan R, Weitzel KG: Pretreatment management of the patient receiving anticoagulant drugs. J Am Dent Assoc 117: 479, 1988 12. Mulligan R: Response to anticoagulant drug withdrawal. J Am Dent Assoc 115:435, 1987 13. Marietta M, Bertesi M, Simoni L, et al: A simple and safe nomogram for the management of oral anticoagulation prior to minor surgery. Clin Lab Haematol 25:127, 2003 14. Todd DW: Anticoagulated patients and oral surgery. Arch Intern Med 163:1242, 2003 15. Todd DW: Anticoagulant therapy: consideration of modification in conjunction with minor surgery. J Oral Maxillofac Surg 61:1117, 2003 16. Lloyd RE: Dental surgery in the anticoagulated patient. Br Dent J 194:530, 2003 17. Milligan PE, Banet GA, Gage BF: Perioperative reduction of the warfarin dose. Am J Med 115:741, 2003 18. Davis FB, Sczupak CA: Outpatient oral anticoagulation: guidelines for long-term management. Postgrad Med 66:100, 1979 19. Akbarian M, Austen G, Yurchak PM, et al: Thromboembolic complications of prosthetic cardiac valves. Circulation 37: 826, 1968 20. Behrman SJ, Wright IS: Dental surgery during continuous anticoagulant therapy. J Am Dent Assoc 62:172, 1961 21. Marshall J: Rebound phenomena after anticoagulant therapy in cerebrovascular disease. Circulation 28:329, 1963 22. Roser SM, Rosenbloom B: Continued anticoagulation in oral surgery procedures. Oral Surg Oral Med Oral Pathol 40:448, 1975 23. Ansell JE: The perioperative management of warfarin therapy. Arch Intern Med 163:881, 2003 24. Douketis JD: Perioperative anticoagulation management in patients who are receiving oral anticoagulant therapy: A practical guide for clinicians. Thromb Res 108:3, 2002 WARD AND SMITH 25. Bailey BM, Fordyce AM: Complications of dental extractions in patients receiving warfarin anticoagulant therapy. A controlled clinical trial. Br Dent J 155:308, 1983 26. Benoliel R, Leviner E, Katz J, et al: Dental treatment for the patient on anticoagulant therapy: Prothrombin time value– What difference does it make? Oral Surg Oral Med Oral Pathol 62:149, 1986 27. Greenberg MS, Miller MF, Lynch MA: Partial thromboplastin time as a predictor of blood loss in oral surgery patients receiving coumarin anticoagulants. J Am Dent Assoc 84:583, 1972 28. Kovacs B, Toth K, Kerenyi G: Post-extraction hemostasis during coumarin anticoagulant therapy with a locally applied coagulation-active substance. Int J Oral Surg 5:3, 1976 29. Kwapis BW: Anticoagulant therapy and dental practice. J Am Dent Assoc 66:172, 1963 30. Shira RB, Hall RJ, Guernsey LH: Minor oral surgery during prolonged anticoagulant therapy. J Oral Surg Anesth Hosp Dent Serv 20:93, 1962 31. Tomasi NJ, Wolf JE: Presurgical management of a patient receiving anticoagulant therapy: Report of case. J Am Dent Assoc 88:1028, 1974 32. Waldrep AC Jr, McKelvey LE: Oral surgery for patients on anticoagulant therapy. J Oral Surg 26:374, 1968 33. Yoshimura Y, Oka M, Kishimoto H, et al: Hemodynamic changes during dental extraction and post-extraction bleeding in patients with prosthetic heart valves. Int J Oral Maxillofac Surg 16:425, 1987 34. Mehta DK: Dental surgery in the anticoagulated patient. Br Dent J 194:530, 2003 35. Malden NJ: Warfarin and extractions. Br Dent J 194:65, 2003 36. Gibbons AJ, Evans IL, Sayers MS, et al: Warfarin and extractions. Br Dent J 193:302, 2002 37. Gibbons AJ, Sugar AW: Evidence for continuing warfarin during dental extractions. Br Dent J 194:65, 2003 38. Balderston RH: Warfarin and extraction. Br Dent J 194:408, 2003 39. Brown AE: Warfarin and extractions. Br Dent J 193:668, 2002 40. Gibbons AJ, Sugar AW: Re: Sugar AW et al: Can warfarin be continued during dental extraction? Results of a randomised controlled trial. Br J Oral Maxillofac Surg 41:280, 2003 41. Dunn AS, Turpie AG: Perioperative management of patients receiving oral anticoagulants: A systematic review. Arch Intern Med 163:901, 2003 42. Gibbons AJ, Sugar AW: Oral anticoagulation and dental extractions. Br J Haematol 119:1137, 2002 43. Troulis MJ, Head TW, Leclerc JR: Dental extractions in patients on an oral anticoagulant: A survey of practices in North America. J Oral Maxillofac Surg 56:914, 1998 44. Gohlke-Barwolf C: Anticoagulation in valvar heart disease: New aspects and management during non-cardiac surgery. Heart 84:567, 2000 45. Ansell J, Hirsh J, Dalen J, et al: Managing oral anticoagulant therapy. Chest 119:22S, 2001 (suppl 1) 46. Muthukrishnan A, Bishop K: An assessment of the management of patients on warfarin by general dental practitioners in South West Wales. Br Dent J 195:567, 2003 47. Webster K, Wilde J: Management of anticoagulation in patients with prosthetic heart valves undergoing oral and maxillofacial operations. Br J Oral Maxillofac Surg 38:124, 2000 48. Hirsh J, Fuster V, Ansell J, et al: American Heart Association/ American College of Cardiology Foundation guide to warfarin therapy. Circulation 107:1692, 2003 49. Fuster V, Ryden LE, Asinger RW, et al: ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: Executive summary. A Report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation): Developed in Collaboration With the North American Society of Pacing and Electrophysiology. J Am Coll Cardiol 38:1231, 2001 1459 50. Lung B, Gohlke-Barwolf C, Tornos P, et al: Recommendations on the management of the asymptomatic patient with valvular heart disease. Eur Heart J 23:1252, 2002 51. Butchart EG, Gohlke-Barwolf C, Antunes MJ, et al: Recommendations for the management of patients after heart valve surgery. Eur Heart J 26:2463, 2005 52. Levy S, Breithardt G, Campbell RW, et al: Atrial fibrillation: Current knowledge and recommendations for management. Working Group on Arrhythmias of the European Society of Cardiology. Eur Heart J 19:1294, 1998 53. Guidelines on oral anticoagulation: Third edition. Br J Haematol 101:374, 1998 54. Update. Guidelines on oral anticoagulation: Third edition. Paper presented at the British Society for Hematology, 2005. http://www.bcshguidelines.com 55. Beirne OR, Koehler JR: Surgical management of patients on warfarin sodium. J Oral Maxillofac Surg 54:1115, 1996 56. Attermann J, Andersen NT, Korsgaard H, et al: Precision of INR measured with a patient operated whole blood coagulometer. Thromb Res 110:65, 2003 57. Fuller JL, Weinert SE: Evaluation of the Accuracy and Precision of the CoaguChek S Monitor. Indianapolis, IN, Roche Diagnostics Corporation, 2001, pp 1-4 58. Gardiner C, Williams K, Mackie IJ, et al: Patient self-testing is a reliable and acceptable alternative to laboratory INR monitoring. Br J Haematol 128:242, 2004 59. Lizotte A, Quessy I, Vanier MC, et al: Reliability, validity and ease of use of a portable point-of-care coagulation device in a pharmacist-managed anticoagulation clinic. J Thromb Thrombolysis 14:247, 2002 60. McBane RD II, Felty CL, Hartgers ML, et al: Importance of device evaluation for point-of-care prothrombin time international normalized ratio testing programs. Mayo Clin Proc 80: 181, 2005 61. Tay MH, Tien SL, Chua TS, et al: An evaluation of point-of-care instrument for monitoring anticoagulation level in adult cardiac patients. Singapore Med J 43:557, 2002 62. Havrda DE, Hawk TL, Marvin CM: Accuracy and precision of the CoaguChek S versus laboratory INRs in a clinic. Ann Pharmacother 36:769, 2002 63. Matthew IR, Browne RM, Frame JW, et al: Tissue response to a haemostatic alginate wound dressing in tooth extraction sockets. Br J Oral Maxillofac Surg 31:165, 1993 64. Mattsson T, Anneroth G, Kondell PA, et al: ACP and surgical in bone hemostasis. A comparative experimental and histologic study. Swed Dent J 14:57, 1990 65. Martinowitz U, Mazar AL, Taicher S, et al: Dental extraction for patients on oral anticoagulant therapy. Oral Surg Oral Med Oral Pathol 70:274, 1990 66. Sheller B, Tong D: Dental management of a child on anticoagulant therapy and the International Normalized Ratio: Case report. Pediatr Dent 16:56, 1994 67. Carr MM, Mason RB: Dental management of anticoagulated patients. J Can Dent Assoc 58:838, 1992 68. Muthukrishnan A: Re: Webster K, Wilde J. Management of anticoagulation in patients with prosthetic heart valves undergoing oral and maxillofacial operations. Br J Oral Maxillofac Surg 40:266, 2002 69. Al-Belasy FA, Amer MZ: Hemostatic effect of n-butyl-2-cyanoacrylate (histoacryl) glue in warfarin-treated patients undergoing oral surgery. J Oral Maxillofac Surg 61:1405, 2003 70. Borea G, Montebugnoli L, Capuzzi P, et al: Tranexamic acid as a mouthwash in anticoagulant-treated patients undergoing oral surgery. An alternative method to discontinuing anticoagulant therapy. Oral Surg Oral Med Oral Pathol 75:29, 1993 71. Carter G, Goss A: Tranexamic acid mouthwash–A prospective randomized study of a 2-day regimen vs 5-day regimen to prevent postoperative bleeding in anticoagulated patients requiring dental extractions. Int J Oral Maxillofac Surg 32:504, 2003 72. Carter G, Goss A, Lloyd J, et al: Tranexamic acid mouthwash versus autologous fibrin glue in patients taking warfarin undergoing dental extractions: A randomized prospective clinical study. J Oral Maxillofac Surg 61:1432, 2003 1460 73. Della Valle A, Sammartino G, Marenzi G, et al: Prevention of postoperative bleeding in anticoagulated patients undergoing oral surgery: Use of platelet-rich plasma gel. J Oral Maxillofac Surg 61:1275, 2003 74. Halfpenny W, Fraser JS, Adlam DM: Comparison of 2 hemostatic agents for the prevention of postextraction hemorrhage in patients on anticoagulants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 92:257, 2001 75. Zanon E, Martinelli F, Bacci C, et al: Safety of dental extraction among consecutive patients on oral anticoagulant treatment managed using a specific dental management protocol. Blood Coagul Fibrinolysis 14:27, 2003 76. Barrero MV, Knezevic M, Martin MT, et al: Cirugia oral en pacientes en tratamiento con anticoagulantes orales. Pauta de actuacion. Medicina Oral 7:63, 2002 77. Blinder D, Manor Y, Martinowitz U, et al: Dental extractions in patients maintained on oral anticoagulant therapy: Comparison of INR value with occurrence of postoperative bleeding. Int J Oral Maxillofac Surg 30:518, 2001 78. Blinder D, Manor Y, Martinowitz U, et al: Dental extractions in patients maintained on continued oral anticoagulant: Comparison of local hemostatic modalities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 88:137, 1999 79. Campbell JH, Alvarado F, Murray RA: Anticoagulation and minor oral surgery: Should the anticoagulation regimen be altered? J Oral Maxillofac Surg 58:131, 2000 80. Cannon PD, Dharmar VT: Minor oral surgical procedures in patients on oral anticoagulants–A controlled study. Aust Dent J 48:115, 2003 81. Devani P, Lavery KM, Howell CJ: Dental extractions in patients on warfarin: Is alteration of anticoagulant regimen necessary? Br J Oral Maxillofac Surg 36:107, 1998 82. Evans IL, Sayers MS, Gibbons AJ, et al: Can warfarin be continued during dental extraction? Results of a randomized controlled trial. Br J Oral Maxillofac Surg 40:248, 2002 83. Ramstrom G, Sindet-Pedersen S, Hall G, et al: Prevention of postsurgical bleeding in oral surgery using tranexamic acid without dose modification of oral anticoagulants. J Oral Maxillofac Surg 51:1211, 1993 84. Souto JC, Oliver A, Zuazu-Jausoro I, et al: Oral surgery in anticoagulated patients without reducing the dose of oral anticoagulant: A prospective randomized study. J Oral Maxillofac Surg 54:27, 1996 85. Street AM, Leung W: Use of tranexamic acid mouthwash in dental procedures in patients taking oral anticoagulants. Med J Aust 153:630, 1990 86. Sindet-Pedersen S, Ramstrom G, Bernvil S, et al: Hemostatic effect of tranexamic acid mouthwash in anticoagulant-treated patients undergoing oral surgery. N Engl J Med 320:840, 1989 87. Assael LA: Hemostasis is a shared responsibility. J Oral Maxillofac Surg 61:1377, 2003 88. Weideman E: Risk assessment of long term post-operative bleeding following tooth extraction(s) in the pre-transplant liver failure patient. J Oral Maxillofac Surg 63:33, 2005 (suppl 1) 89. Hirsh J, Dalen J, Anderson DR, et al: Oral anticoagulants: Mechanism of action, clinical effectiveness, and optimal therapeutic range. Chest 119:8S, 2001 (suppl 1) DENTOALVEOLAR SURGERY IN ANTICOAGULATED PATIENTS 90. Brickey DA, Lawlor DP: Transbronchial biopsy in the presence of profound elevation of the international normalized ratio. Chest 115:1667, 1999 91. Wood JC, Conn HL Jr: Prevention of systemic arterial embolism in chronic rheumatic heart disease by means of protracted anticoagulant therapy. Circulation 10:517, 1954 92. Kearon C, Hirsh J: Management of anticoagulation before and after elective surgery. N Engl J Med 336:1506, 1997 93. Alexander R, Ferretti AC, Sorensen JR: Stop the nonsense not the anticoagulants: A matter of life and death. N Y State Dent J 68:24, 2002 94. Gibbons AJ: Oral surgery in patients taking anticoagulant therapy. J Oral Maxillofac Surg 62:644, 2004 95. Wood GD: Antibiotic prescribing and warfarin enhancement. Br Dent J 175:241, 1993 96. Wood GD, Deeble T: Warfarin: Dangers with antibiotics. Dent Update 20:350, 1993 97. Bandrowsky T, Vorono AA, Borris TJ, et al: Amoxicillin-related postextraction bleeding in an anticoagulated patient with tranexamic acid rinses. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 82:610, 1996 98. Malden N: The great warfarin debate. Br Dent J 195:2, 2003 99. Lieblich S: Tranexamic acid rinses in anticoagulated patients. J Oral Maxillofac Surg 54:657, 1996 100. Scully C, Wolff A: Oral surgery in patients on anticoagulant therapy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 94:57, 2002 101. Sen P, Sen R: Re: Sugar AW et al: Can warfarin be continued during dental extraction? Results of a randomised controlled trial. Br J Oral Maxillofac Surg 41:132, 2003 102. Mehra P, Cottrell DA, Bestgen SC, et al: Management of heparin therapy in the high-risk, chronically anticoagulated, oral surgery patient: A review and a proposed nomogram. J Oral Maxillofac Surg 58:198, 2000 103. Johnson-Leong C, Rada RE: The use of low-molecular-weight heparins in outpatient oral surgery for patients receiving anticoagulation therapy. J Am Dent Assoc 133:1083, 2002 104. Todd DW, Roman A: Outpatient use of low-molecular weight heparin in an anticoagulated patient requiring oral surgery: Case report. J Oral Maxillofac Surg 59:1090, 2001 105. Jafri SM: Periprocedural thromboprophylaxis in patients receiving chronic anticoagulation therapy. Am Heart J 147:3, 2004 106. Hewitt RL, Chun KL, Flint LM: Current clinical concepts in perioperative anticoagulation. Am Surg. Mar 65:270, 1999 107. Zusman SP, Lustig JP, Bin Nun G: Cost evaluation of two methods of post tooth extraction hemostasis in patients on anticoagulant therapy. Community Dent Health 10:167, 1993 108. Eckman MH, Beshansky JR, Durand-Zaleski I, et al: Anticoagulation for noncardiac procedures in patients with prosthetic heart valves. Does low risk mean high cost? JAMA 263:1513, 1990 109. Bloomer CR: Excessive hemorrhage after dental extractions using low-molecular-weight heparin (Lovenox) anticoagulation therapy. J Oral Maxillofac Surg 62:101, 2004