Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
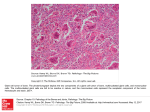
CHERUBISM Cherubism is a rare developmental jaw condition that is generally inherited as an autosomal dominant trait with high penetrance but variable expressivity. Several investigators have reported a higher disease penetrance in male than in females. Sporadic cases also can occur and are thought to represent spontaneous mutations. In two reports published simultaneously by laboratories on different continents, the gene for cherubism was mapped to chromosome 4p16. Mutations subsequently were identified in the SH3BP2 gene within this locus. The protein encoded by this gene is believed to function in signal transduction pathways and to increase the activity of osteoclasts and osteoblasts during normal tooth eruption. It has been suggested that mutations in the SH3BP2 gene may lead to pathologic activation of osteoclasts and disruption of jaw morphogenesis. However, the molecular pathogenesis of cherubism remains poorly understood. The name cherubism was applied to this condition because the facial appearance is similar to that of the plump-cheeked little angels (cherubs) depicted in Renaissance paintings. Although cherubism also has been called familial fibrous dysplasia, this term should be avoided because cherubism has no relationship to fibrous dysplasia of bone. CLINICAL AND RADIOGRAPHIC FEATURES Although some examples of cherubism may develop as early as 1 year of age, the disease usually occurs between the ages of 2 and 5 years. In mild cases the diagnosis may not be made until the patient reaches 10 to 12 years of age. The clinical alterations typically progress until puberty. Then stabilize and slowly regress. The cherublike facies arises from bilateral involvement of the posterior mandible that produces angelic chubby cheeks. In addition, there is an “eyes upturned to heaven” appearance that is due to a vide rim of exposed sclera noted below the iris. This latter feature is due to involvement of the infraorbital rim and orbital floor that tilts the eyeballs upward, as well as to stretching of the upper facial skin that pulls the lower lid downward. On occasion, affected patients also reveal marked cervical lymphadenopathy. The mandibular lesions typically appear as a painless, bilateral expansion of the posterior mandible that tends to involve the angles and ascending rami. The bony expansion is usually bilaterally symmetrical; in severe cases, most of the mandible is involved. Milder maxillary involvement occurs in the tuberosity areas; in severe cases, the entire maxilla can be affected. Extensive bone involvement causes a marked widening and distortion of the alveolar ridges. In addition to the aesthetic and psychologic effect, the enlargements may cause tooth displacement or failure of eruption, impair mastication, crate speech difficulties, or rarely lead to loss of normal vision or hearing. Although there have been rare reports of unilateral cherubism, it is difficult to accept these as examples of this disease unless there is a strong family history. Radiographically, the lesions are typically multilocular, expansile radiolucencies. The appearance is virtually diagnostic as a result of their bilateral location. Less commonly, the lesions appear as unilocular radiolucencies. Although cherubism typically involves only the jaws, involvement also has been reported rarely in other bones such as the ribs and humerus. No unusual biochemical findings have been reported in patients with cherubism. If laboratory results do not suggest the diagnosis of hyperparathyroidism, then most children with multiple symmetrical giant cell granulomas represent examples of cherubism. However, multiple giant cell lesions may be seen in association with other conditions, including Ramon syndrome, JaffeCampanacci syndrome, and a Noonan-like syndrome. It has been suggested that the bony lesions of cherubism represent a phenotypic picture common to a number of disease processes that the bony lesions of cherubism represent a phenotypic picture common to a number of disease processes that arise from multiple, distinct, initiating pathogenetic events. HISTOPATHOLOGIC FEATURES The microscopic findings of cherubism are essentially similar to those of isolated giant cell granulomas, and they seldom permit a specific diagnosis of cherubism in the absence of clinical and radiologic information. The lesional tissue consists of vascular fibrous tissue containing variable numbers of multinucleated giant cells. The giant cells tend to be small and usually aggregated focally. Like the giant cells in central giant cell granulomas, the giant cells in cherubism express markers suggestive of osteoclastic origin. Foci of extravasated blood are commonly present. The stroma in cherubism often tends to be more loosely arranged than that seen in giant cell granulomas. In some cases, cherubism reveals eosinophilic, cufflike deposits surrounding small blood vessels throughout the lesion. The eosinophilic cuffing appears to be specific for cherubism. However, these deposits are not present in many cases, and their absence does not exclude a diagnosis of cherubism. In older, resolving lesions of cherubism, the tissue becomes more fibrous, the number of giant cells decreases, and new bone formation is seen. TREATMENT AND PROGNOSIS The prognosis in any given case is unpredictable. In most instances the lesions tend to show varying degrees of remission and involution after puberty. By the fourth decade, the facial features of most patients approach normalcy. In spite of the typical scenario, some patients demonstrate very mild alterations, whereas other reveal grotesque changes that often are very slow to resolve. In occasional patients, the deformity can persist. The question of whether to treat or simply observe a patient with cherubism is difficult. Excellent results have been obtained in some cases by early surgical intervention with curettage of the lesions. Conversely, early surgical intervention sometimes has been followed by rapid regrowth of the lesions and worsening deformity. A course limited only to observation may result in extreme and sometimes grotesque facial deformity, with associated psychologic problems and functional deformity that may necessitate extensive surgery. Several investigators have suggested the use of calcitonin in severe cases, but such therapy is contraindicated because of the risk of development of postirradiation sarcoma. The optimal therapy for cherubism has not been determined.