Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
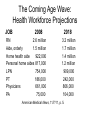
The Coming Age Wave: Perspectives of a LTC Geriatrician Peter Jaggard, MD CMD Vice President of Medical Affairs Presbyterian Homes, IL The Coming Age Wave: US Population 65+ (in millions) 80 70 60 50 40 30 20 10 0 1980 2000 2020 2030 The Coming Age Wave: Health Workforce Projections JOB 2008 RN 2.6 million Aide, orderly 1.5 million Home health aide 922,000 Personal home aides 817,000 LPN 754,000 PT 186,000 Physicians 661,000 PA 75,000 2018 3.2 million 1.7 million 1.4 million 1.2 million 909,000 242,000 806,000 104,000 American Medical News, 11/7/11, p. 5. The Coming Age Wave: US National Health Expenditures • 2009: $2.5 Trillion • 2019: $4.6 Trillion (before health reform) 6.3% annual growth • 2019: $4.3 Trillion (after health reform) 5.7% annual growth Cutler et.al., The Impact of Health Reform on Health System Spending, (Washington and New York), Center for American Progress and The Commonwealth Fund, May 2010. Cited by Glenn Steele , MD at the McEachern Symposium, Kellogg School of Management, 5/11/11 $2.5 Trillion Health Bill (2009): Where It Came From • • • • • • • • • 32% 20% 12% 10% 5% 4% 3% 7% 6% private health insurance Medicare out of pocket Medicaid Federal Medicaid state and local VA, DOD, CHIP Government Public Health other third party payers and programs investment $2.5 Trillion Health Bill (2009): Where It Went • 31% Hospital Care • 20% Physicians and Clinics • 10% Prescription Drugs • 7% Dental Services, other Professionals • 7% Govt. admin., net cost health insurance • 6% Investment • 6% Nursing facilities, CCRCs • 5% other health, residential, personal care • 3% Home Health Care • 3% Government Public Health Activities • 3% other medical products – DME, etc. Medicare and Health Reform: A Look Back and Down the Road • 2010: 47.5 Mill beneficiaries • 2010: $523 Billion expenditures • Affordable Care Act: $500 Bill in cuts over 10 years (nearly 10% of Medicare budget) Medicare Now: 2011 Cuts for NFs • 11% cut for post-acute NF services due to $4 Billion cost overrun last year • NFs receive about 20% of revenue from post-acute care • Reductions may force some NFs out of Medicare business, if it is a money loser Medicare 2012: Cuts for MDs? • 29.5% physician reimbursement cut set for 2012 • This coming due because of Sustainable Growth Rate formula which has been “fixed” annually by Congress for years • SGR projected cuts were used during health reform debate for overly optimistic projections of cost savings • Lack of action may force many MDs out of Medicare, reducing patient access to PCP The Coming Age Wave: Concerns of a Geriatrician • Who will take care of frail older adults? • How will their care be paid for? • Will quality of care be sacrificed for cost savings? Health Care for the Coming Age Wave: The “Triple Aim” of Reform • Lower Cost • Improve Quality of Individual Care • Increase Access and thereby Improve Health of Population The Coming Age Wave: Are ACOs the Answer? ACOs offer solutions through variety of strategies: • Hospital-physician integrated networks • Shared savings model • Health information technology • Clinical decision support • Health information exchanges • Disease management • Care coordination • Use of physician extenders (APN, PA) What Does the Experience of the 1990s Reveal about the Proposed Components of ACOs? • Little or no evidence of effectiveness • Need a more evidence-based approach • Revisit assumptions on which strategic changes are made • Rather than focus on structure, focus on processes to bring people into interaction who need it Lawton Burns, PhD., presentation at McEachern Symposium, Kellogg School of Management, 5/11/11 Where are Achievable Savings? • Accountable Care Organizations looked at as a mechanism by which to control costs of care for episodes of illness • “The savings generated by ACOs, in many cases, are expected to result from reduced inpatient admissions.” (CMS) – from Henry Allen, Senior Attorney for Advocacy, AMA Reducing NF Hospitalizations as a Potential Medicare Cost-Saver • 8.5% of all Medicare hospitalizations are from NFs • 40% of these occur within 90 days of NF admit • Nearly 1/5 of Medicare hospital discharges are readmitted within 30 days; 27% of these are for CHF, 21% for pneumonia • From 1984 to 2009, rehospitalization rate at 60 days had increased from 22.5% to 31% The INTERACT Project: A Working Solution to Reducing Transfers from LTC – Acute Care • • • • • INTERventions to Reduce Acute Care Transfers Multi-site, ongoing research in LTC Measures and tracks hospitalization rate at NF QI tool to assess avoidable hospitalizations QI tools to assist nursing staff in early identification, assessment, communication, and documentation of change of condition INTERACT II Results • NHs in Massachusetts, NY, Florida • 6-month study period compared to previous year 6-month period • 24% reduction in hospitalizations for 17 NHs rated as “engaged” in INTERACT process • 6% reduction in hospitalizations in 8 NHs rated as “not engaged” • 3% reduction in 11 NHs used as a comparison NF Hospitalizations: Presbyterian Home McGaw Center • • • • NF average census 170; 27% subacute Staff physicians rounding 3-4 X weekly Full-time APN Hospitalization rate 2.07/1000 pt-days (cp with rate of approx 4 in published study) • Med A 30-day rehospitalization 9.9% (Chicago area average 17%) Whose Care Costs Medicare the Most? • 20% of Medicare population accounts for 2/3 of Medicare expenditures • Spending for beneficiaries with 5 or more chronic conditions as a percentage of Medicare spending has risen from 52% (1984) to 76% (2002). Buckets for Cost Savings • Big: Lifestyle modifications for young and middle aged adults • Medium: Higher quality, more costeffective care strategies • Smaller: administrative efficiency Comorbidity, Trajectories of Decline, and Transitional Care • Multiple illness = more acute episodes of care • Acute on Chronic diseases = various trajectories of functional decline; more transitions of care • Transitions of care are increasingly more complex, fragmented, and dangerous for older adults (Home-hospital-SNF-home care-etc.) Looming Challenges • In the face of the coming age wave, Medicare cuts, and limited resources, how will we care for older adults with complex needs? • Will we manage the data/IT wave, or will it dictate care? • Will health care organizations keep their focus on their core mission and values, the care of and respect for the patient? Or will that be lost behind a wave of new bureaucracies, information systems, and data gathering? “Who is my Neighbor?” - A Story Seeing, Caring and Transitioning Those in Need • A complex patient • A caring spirit • Hands-on treatment • Providing continuity of care through a difficult transition for the patient, even at some cost to the provider A Few Suggestions • Develop systems of care that improve quality by filling gaps in transitions of care for older adults • Help patients define realistic goals of care and execute advance care planning • Develop collaborative inter-institutional professional relationships along the continuum (Hospital-SNF-Home Care-Hospice) • Use IT systems and data wisely; EMR systems need active human input and management • EMRs are not a panacea; med errors still happen A Few Suggestions • Develop clinical protocols that will help older adults reduce hospitalizations • Emphasize team care at all sites of care to maximize care, function, and independence of older adults • Develop or review your organization’s mission and values • Renew your commitment to honor, respect, and care for each person in your care as you help them navigate the changing waves of healthcare