Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
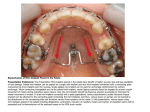
Consent Form for the Insertion of One or More Mini-Screws During the Course of Orthodontic Treatment of: Name of patient: Name of treating doctor 1. Information regarding the procedure Course of procedure: Topical anesthesia Infiltration anesthesia Tissue punch at the insertion site Pilot drill Insertion of (number) mini-implants Coupling of the mini-implant to the orthodontic appliance Removal of the mini-implant (at the conclusion of treatment) Mini-crew system: The potential risks and complications of the planned procedure and the resulting treatment have been discussed in depth, especially the possibility of: General Side Effects/Complications: After the procedure, pain may persist. Generally, it will wear off within a few hours after the procedure. Bleeding or prolonged hemorrhaging are very rare but can occur, especially in patients with hemorrhagic diatheses. Existing allergies or sensitivity (for example, from the anesthetic, disinfectant, latex) may lead to transient swelling, itching, sneezing, skin rash, dizziness or other related reactions. Severe complications affecting vital functions (heart circulation, respiration, kidneys) or permanent damage (for example, organ failure or paralysis) are extremely rare. Specific Side Effects/ Complications: Root damage due to proximity of the mini-screws Soft tissue injury during placement Fracture, loosening or premature loss of mini-screw Inflammation of the soft and hard tissues surrounding the mini-crew Individual risks: Post-operative Care Instructions: For 24 hours after the procedure, please refrain from smoking, drinking alcohol or exercising Do not eat while the area is still numb It is very important to include the area surrounding the mini-screw into your daily oral hygiene routine according to the instructions received from your doctor. In the first days following the insertion, the application of a disinfecting agent (mouth rise) may be required. Regular recall of appointments will be necessary as part of the post-operative care. Please immediately contact your doctor if you experience one of the following symptoms: continuous hemorrhaging, severe swelling, throbbing pain or other later discomfort at the insertion site. 2. Consent I was informed that the above procedures will be performed on me. The reason and the different steps involved have been explained to me. The risks, benefits and alternatives were discussed. I am aware that new information may be obtained during the procedure which may necessitate other, nor previously discussed measures. Possible physical, psychological and professional complications after the procedure have been pointed out to me. All my questions have been answered. I was sufficiently educated regarding the details of the above procedure and any further clarification is not necessary. I understand that I can revoke my consent at any time. I confirm that I have listed all the ailments that I am aware of in the health history. Additions: My decision is well thought through and I require no further time or information to reach a decision. □ I hereby consent to the insertion of mini-screws. I agree to the anesthetic and potentially necessary changes from the anticipated course of action as outlined above. If you refuse certain steps of the treatment, please specify below: □ I do not consent to the proposed treatment. I was informed of the consequences this decision may have. City Date Patient* Doctor Witness *Parent/Guardian for minors