Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Idiopathic intracranial hypertension wikipedia , lookup
Vision therapy wikipedia , lookup
Blast-related ocular trauma wikipedia , lookup
Contact lens wikipedia , lookup
Keratoconus wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
Eyeglass prescription wikipedia , lookup
Cataract surgery wikipedia , lookup
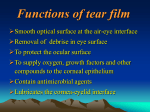
Lecture 17 Conjunctiva is the visible layer in which I see redness if irritation happens. Viral conjunctivitis: Pink eye due to a viral infection… Might be a recent cold, sore throat, or URTI of viral origin. It might be concomitant with infection, or come after cold is cleared. Symptoms of viral conjunctivitis: pink eye (not red) with copious amounts of watery discharge (a lot of tears), and some signs of cold like low-grade fever and swollen lymph nodes. Usually clears out by itself in 1-3 weeks. One week mostly and in extreme cases may stay up to 3 weeks. Only supportive treatment is needed (artificial tears and ocular decongestants). Viral conjunctivitis is contagious so patient should be warned to use his own things like tissue, pillows, or towels. Many come with no signs of cold, but actually received virus from another person at home. Allergic conjunctivitis: Cause is allergy. They have general allergic reactions caused by antigens. Major symptom is itching. Somehow red eye and watery discharge are also symptoms of allergic conjunctivitis. If patient doesn’t take vaccine, he’ll develop allergic rhinitis every season. Best treatment is removal of cause of allergy and staying away from it. Ocular decongestants and antihistamines, systemic oral antihistamines, and cold compresses can be used. Bacterial conjunctivitis is a bacterial infection. Staph. epidermidis and Staph. aureus are already present around the eye. Symptoms here include purulent discharge (not watery discharge). Red eye and purulence are expected. Purulence leads to key symptom which is eyes being closed together on awakening. Topical antibiotic is needed. Sometimes newborns develop minor blockage of nasolacrimal drainage (duct blocks). It can be infectious, but here we aren’t talking about conjunctivitis in which all eye is red and purulent. Corneal edema Cornea has 5 layers; outermost is epithelial while innermost is endothelial. Cornea itself is avascular and takes all nutrition and oxygen from tear film. It is responsible for refractive property. If edema happens in any of the layers, inaccuracy of vision results since light has to cross water layer before reaching lens. They say corneal edema is self-treated if you could recognize it, although the doctor has never done. We are supposed to see edema in cornea (bulging of cornea). Over-wearing of contact lenses can cause it since they don’t allow for gas exchange. Vision of person might be clear but with a frame around what he sees. To remove water accumulation around the cornea, hypertonic saline (2-5%) is used. Water moves to high solute concentration and edema goes away. We have isotonic saline (0.9%) in community pharmacies. Hypertonic saline isn’t present there; it can be found in ophthalmic-clinic pharmacies. Dry eye Very common eye disorder. It happens in all ages for different reasons. Eye isn’t necessarily red. It might annoy the patient and he would have sandy or gritty feeling ()تراب أو حصى Tear film consists of 3 layers. The bulky layer is the middle aqueous layer. An oily layer of meibom is on the outer layer that prevents the evaporation of tear film. Goblet glands hold tear film on the surface. Normally, secretions of all glands are distributed by blinking while excess is washed away and drained. Dry eye results if any discontinuity happens. It gives the feeling that the surface of the cornea isn’t covered continuously by tear film, so glands as a reflex produce more tears again, and that’s why excess tearing is a symptom although we have a dry eye condition. Some causes of dry eye are known, others aren’t: Aging. Meibomial glands that secrete meibom undergo dystrophy as a person ages. If dystrophy happens, less meibom is secreted so outermost layer will be deficient resulting in more evaporation of tear film. Lid defects whether in blinking, distribution of tear film, secretions, surgeries, cancer removal that affected the eyelid, or anything affecting its innervation or movement. Sjogren’s syndrome initially characterized by dry eye or mouth, the person may develop rheumatoid arthritis later in disease. Bell’s palsy: paralysis of nerve supplying eyelid. Secretions and blinking are inhibited. Solution is by knowing reason of dry eye. Non pharmacological can be used for treatment in milder cases of known cause. If person is going on a trip in a hot weather or going for swimming, he can take artificial tears or demulcent to relieve dry eye. If case wasn’t treated by artificial tears, vitamin A can be used. If very severe eye dry and 3-4 applications aren’t working, we go for more drastic measures: a) Ocular inserts (Ocuserts “lenses”) or Na hyaluronate can be used. Act as nice demulcents on eye surface with good lubricant properties. b) Occlusion of lacrimal drainage system to increase available tear pool (For people with Bell’s palsy or very severe dry eye, they might go for stitching to increase retention of tears and decrease drainage) “”بيقطبوا طرف عينهم Artificial tears Dry spots on eye surface might be from lipids or mucous. They are substituted by drop of artificial tears. Drop must mix on tear film, stabilize it, and stay there for a long time to decrease drainage (so must be a little viscous), thus neutral oils and some surfactants are present in formula. Washing out happens with blinking, so repetitive application is needed. Lubricants More viscous preparations can be applied at night, while less viscous during the day. Artificial tear solutions are sterile preparations. 1st group: Cellulose ethers. A lot of cases may benefit from them. They vary in viscosity according to branching. Methylcellulose is applied from 0.2-1% (concentration) HEC and HPC are less viscous. They adhere nicely on tear film, making a cohesive film on eye surface. They stabilize tear film and prevent evaporation. Nice emollient properties, non-irritant and non-toxic. They stay 3-4 hours before being washed out. 2nd and 3rd groups of polymeric substances are PVA and PVP. “Same group but have different effects”. Rationale behind using them is that it was found that tears of patients with dry eyes have higher osmolarity. This might be due to composition, secretions, or glands making tears hypertonic; thus making tear film insufficient. We aim for returning tonicity to normal. So, first we try to find the reason behind dry eye, if none was found, we use ethyl cellulose. If it doesn’t work, go for PVA or PVP. Here we are not solving the problem; but finding an artificial tear substituent that would return isotonicity. PVP has surface active properties. Its replacement is better for mucin (deeper layer) than for outermost layer. “If dry eye problem was due to goblet cell secretions, PVP might work better”. In moderate to severe cases, these preparations need to be instilled more frequently, making them annoying. Carbomer has gelling effect. 4th is Retinol Solution We could try it as a last resort if all other previous categories didn’t work. It could help when the reason of dry eye is related to mucin. There is controversy about vitamin A’s effect. Some say it’s excellent and some say it causes dry eye. When people take Roaccutane (for acne), they face dry eye and dry skin; but at the same time it has been proposed that Retinol Palmitate, when applied to the eye, enhances conjunctival proliferation and enhances secretion of mucin from goblet cells. So, when given orally, it affects membrane and meibomial gland secretions, thus causing dry eye while when retinol palmitate is applied topically on the surface of the eye, it enhances proliferation and goblet cell secretions. All ophthalmic preparations should be sterile. Sterility is maintained with multiple uses by addition of preservatives. BAK (Benzalkonium Chloride) causes break down of tear film at preservative concentrations. Other preservatives may be used as alternatives or combination of another preservative with BAK may be introduced (when using more than one preservative, lower concentrations are used of them than if any is used alone) BAK usually causes no problem if used in a formulation for mydriasis or decongestants where tear film is healthy, since tear film would be substituted by a fresh one if it was broken up. “This doesn’t happen in dry eye where a problem with tear film is present” For people are allergic to BAK or other preservatives, Preservative-free Formulations are used. These come in single-use dispensers which are more expensive. Discard solution after 12 hours. All previous groups can be used during the day. Ointments are used at night. They give good lubricating properties. Ointment mixes on the surface and melts when applied to conjunctiva. In people with lid paralysis, ointment is applied, and then eye is closed. This enhances vision in the morning. Decongestants Systemic absorption does take place, but concentration is very low, so side effects are rare. They shouldn’t be given for more than 3 days because of rebound congestion. They might cause dryness of ocular surface for some people. *Xerosis* Nephazoline is mainly the decongestant of choice. Its mydriatic effect may annoy people with lightly pigmented irises (blue or green eyes) “Eye drops may be misused by addicts; they may drink them or mix them in heroin injections. Some use them to hide redness of the eye resulting from congestion after whatever they take. Some put them in water of Sheesha.” Antihistamines are almost always put with decongestants in formulations since patients usually come for signs of both. When talking about allergic conjunctivitis, systemic or ophthalmic preparations may be used. Irrigants are applied to surface ocular tissue. They are sterile. They may be used when patients have a foreign body sensation in the eye, or to wash eye surface between lenses or dressing changes. Preservatives in irrigants would adhere to contact lenses. So they shouldn’t be applied while contact lenses are worn. Irrigants were used in labs. A cup, in which a sterile irrigant such as normal saline or sodium borate is put, was used. Person used to wash eye in cup. It is no longer used since cup should also be sterile or else contamination might happen. Hyperosmotics Saline (2-5%) can be used if corneal edema is present. Solution Lower concentration (2%) Ointment Higher concentration (5%) Instilled in the first few waking hours since edema is mostly present in the morning. Hyperosmotics shouldn’t be used if cornea is traumatized unless the doctor himself prescribes them, since their use would lead to dehydration of the eye. Antiseptics may be used for people with recurrent blepharitis. They are applied on surface of the eye. We don’t have Silver protein and Witch Hazel. Boric acid and Zinc sulphate are mostly used. Boric acid is not supposed to be irritant since it is used on the surface of eye lid, unlike irrigants in which we wash eye with. Boric acid powder may be used for cockroach control. For blepharitis; Boric acid solution, zinc sulphate solution, or diluted baby shampoo applied to eye surface by cotton pad may be used. Multivitamins Retinol palmitate is a vitamin that can be given topically for the eye. It was proposed that a lot of eye and vision problems can be related to vitamins’ deficiency (Vitamins A, C, E and zinc), so there is a tendency for oral (not topical) administration of multivitamins to increase vision accuracy. Taken by people in older ages if there is a possibility of deficiencies. Prosthesis of eye ball Whether there is a defect in the lid or not, or the lid was paralyzed, the artificial eye must be washed with a sterile, buffered isotonic solution of 0.25% tyloxapol and 0.02% BAK. If for any reason the eye ball was lost, like due to an accident or cancer, a prosthetic eye may be implanted. (Huge operation is needed) Long time ago, they used to put an eye ball and stabilize it inside. Now, an implant that holds muscles is put inside and prosthetic eye on the surface. Washing either with prosthetic eye in its place (eye is opened widely and washed), or by removal of eye by suction or by hand, eye washed out and then returned back to its place. Patient should be notified not remove eye frequently and wash since edges may be damaged. (Daily washing of eye in its place, while eye removal and washing every 2-3 weeks) Please refer back to the slides. Those are only notes. Dima Moayad