Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
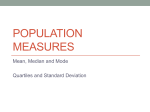
VOLUME 29 䡠 NUMBER 4 䡠 FEBRUARY 1 2011 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I C L E How Long Have I Got? Estimating Typical, Best-Case, and Worst-Case Scenarios for Patients Starting First-Line Chemotherapy for Metastatic Breast Cancer: A Systematic Review of Recent Randomized Trials Belinda E. Kiely, Yu Yang Soon, Martin H.N. Tattersall, and Martin R. Stockler See accompanying editorial on page 347 From the National Health and Medical Research Council Clinical Trials Centre and Sydney Medical School, University of Sydney; Sydney Cancer Centre-Royal Prince Alfred and Concord Repatriation General Hospitals, Sydney, New South Wales, Australia. Submitted May 6, 2010; accepted October 22, 2010; published online ahead of print at www.jco.org on December 28, 2010. Supported by a National Breast Cancer Foundation PhD Scholarship (B.E.K.), a National Health and Medical Research Council Clinical Trials Centre PhD Scholarship, and a Cancer Institute New South Wales Research Scholar Award. Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this article. Corresponding author: Martin R. Stockler, MD, NHMRC Clinical Trials Centre, Locked Bag 77, Camperdown, NSW, 1450, Australia; e-mail: martin.stockler@ sydney.edu.au. © 2010 by American Society of Clinical Oncology 0732-183X/11/2904-456/$20.00 DOI: 10.1200/JCO.2010.30.2174 A B S T R A C T Purpose To estimate scenarios for survival for women with metastatic breast cancer (MBC) who are starting chemotherapy. Patients and Methods We sought randomized, first-line chemotherapy trials for MBC published from 1999 to 2009. We recorded median progression-free survival (PFS) and median overall survival (OS) and extracted the following percentiles (represented scenario) from each OS curve: 90th (worstcase), 75th (lower-typical), 25th (upper-typical), and 10th (best-case). We also estimated these scenarios for each OS curve by multiplying its median by four simple multiples: 0.25 (worst-case), 0.5 (lower-typical), 2 (upper-typical), and 3 (best-case). Estimates were deemed accurate if they were within 0.75 to 1.33 times the actual value. Results From 36 trials (13,083 women), the mean for median PFS was 7.6 months (interquartile range [IQR], 6.0 to 9.0 months), the mean for median OS was 21.7 months (IQR,18.2 to 24.0 months), and the mean for the ratio of median OS to median PFS was 3.0 (IQR, 2.4 to 3.5). The mean for each OS scenario was worst-case, 6.3 months (IQR, 4.8 to 7.5 months); lower-typical, 11.9 months (IQR, 9.9 to 13.2 months); upper-typical, 36.2 months (IQR, 31.1 to 41.3 months); and best-case, 55.8 months (IQR, 47.5 to 60.2 months). Simple multiples of the median gave accurate estimates of the worst-case scenario in 73% of OS curves, lower-typical in 97%, upper-typical in 95%, and best-case in 96%. OS was longer in trials with higher proportions of estrogen receptor–positive tumors (P ⫽ .001) and in trials of trastuzumab-treated human epidermal growth factor receptor 2–positive tumors (P ⫽ .001). Conclusion Simple multiples of an OS curve’s median can accurately estimate typical (half to double the median), best-case (triple the median), and worst-case (one quarter of the median) scenarios for survival. J Clin Oncol 29:456-463. © 2010 by American Society of Clinical Oncology INTRODUCTION Metastatic breast cancer (MBC) is a heterogeneous disease that is essentially incurable. Most women with MBC receive cytotoxic chemotherapy at some stage of their illness. When starting chemotherapy for MBC, women require an understanding of how their cancer and its treatment will affect their life expectancy. Surveys of patients with advanced cancer suggest that all want information about their future,1 most want information about their likely survival time, and many want specific estimates of 456 best-case, average, and worst-case scenarios for survival.2 Information about how to estimate or describe these scenarios is scarce, so it is no surprise that cancer clinicians are often reluctant to estimate and discuss life expectancy.3,4 Survival data from groups of patients with similar characteristics (demographic, disease, and treatment) would be an ideal source of prognostic information but those data are rare. Clinical trials are readily available, easily accessible, and often provide detailed information about survival. Overall survival (OS) curves from clinical trials are usually © 2010 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 Estimating Scenarios for Survival for Metastatic Breast Cancer summarized by their median, and although median survival may be the best single-number description of a survival curve, it is probably not the best way of explaining prognosis to a patient. Providing patients with a single-point estimate of survival based on the median implies unwarranted precision and leaves little room for hope. We previously proposed that providing estimates for the typical range, best-case scenarios, and worst-case scenarios for OS might be a better way of communicating life expectancy and that the percentiles from an OS curve are a useful basis for estimating these scenarios.5 The purpose of this study was to find and summarize survival data from recent, randomized trials of first-line chemotherapy for MBC that would help clinicians estimate and describe prognosis for their patients in this situation. PATIENTS AND METHODS We searched the specialized register maintained by the Secretariat of the Cochrane Breast Cancer Group (CBCG)6 for references coded as “advanced breast cancer” and “chemotherapy” published from January 1999 to June 2009 inclusive. The results were supplemented by searches of MEDLINE and the reference list from a recently published systematic review of MBC chemotherapy trials.7 Two authors independently screened the references and selected trials meeting the following inclusion criteria: randomized trial comparing at least two different chemotherapy regimens being given as first-line chemotherapy for women with MBC, including at least 90 patients enrolled per treatment arm, and Kaplan-Meier curves for OS. We recorded the year of publication, number of treatment arms, names and schedules of the chemotherapy agents, number of participants, median follow-up, patient demographics, and tumor characteristics for each trial. We recorded the median progression-free survival (PFS) and median OS for each treatment group. Each OS curve was independently traced by two authors by using UNSCAN-IT graph digitizing software (Silk Scientific, Orem, UT).8 The median and following percentiles (represented scenarios) were extracted from each OS curve: 90th (worst-case), 75th (lower-typical), 25th (upper-typical), and 10th (best-case; Fig 1). One-, 2-, and 5-year survival percentages were also recorded. Discrepancies were resolved by repeated measurement and discussion. We expected the shape of each OS curve to be approximately exponential allowing its percentiles to be estimated by simple multiples of its median. On the basis of our previous work5,9 and the fact that clinical trial patients are relatively more homogeneous than an unselected clinical population that Proportion Surviving 90th percentile - worst-case scenario 75th percentile 0.8 0.6 Typical scenario Median 0.4 25th percentile 10th percentile best-case scenario 0.2 0 1 2 3 4 5 Time Since Study Entry (years) Fig 1. Survival curve percentiles and their corresponding scenarios. www.jco.org 6 includes a variety of cancers, we hypothesized a priori that the appropriate simple multiples of the median for each percentile would be 0.25 for the 90th, 0.5 for the 75th, 2 for the 25th, and 3 for the 10th. These values were less extreme than those for a true exponential distribution in which the 90th percentile is 0.17 times the median, and the 10th percentile is 3.3 times the median. We also decided a priori that an estimate would be deemed accurate if it was within 0.75 to 1.33 times the actual value, our arbitrary range for reasonable accuracy. We hypothesized that longer median OS would be observed in trials with the following characteristics: higher proportion of women with estrogen receptor (ER) –positive tumors, lower proportion of premenopausal women, lower proportion with visceral metastases, higher proportion with Eastern Cooperative Oncology Group (ECOG) performance status ⬍ 2, lower proportion who had received prior adjuvant chemotherapy, use of a taxane, use of trastuzumab in women with human epidermal growth factor receptor 2 (HER2) –positive tumors, and more recent year of publication. Associations between these factors and median OS were assessed by using simple linear regression. The association between median OS and trastuzumab-treated HER2-positive disease was explored by comparing trials in which all women were HER2-positive and received trastuzumab with trials in which HER2 status was not checked and no women received trastuzumab. The association between median OS and use of a taxane was explored by comparing trials in which all women received a taxane with trials in which no women received a taxane. RESULTS The CBCG register search identified 284 references, and 212 of these related to randomized chemotherapy trials in MBC. Because many of these studies were not about first-line therapy, were small, or were abstracts only with no survival curves, only 27 trials were eligible for this review. The reasons for exclusion are summarized in Figure 2. Supplementary searches of MEDLINE and reference lists identified an additional nine trials. The 36 selected trials included 78 survival curves and 13,083 patients. Thirty-four studies were published in the peerreviewed literature,10-43 and two were published as abstracts only.44,45 A statistically significant difference in PFS was reported in 13 trials (36%),10-13,17,22,30,31,34,37-39,43 and a significant difference in OS was reported in seven trials (19%).11,17,23,27,36,38,43 The characteristics of the trials, including the chemotherapy agents used, are summarized in Table 1. The median follow-up for the 36 trials ranged from 10 months to 102 months with a median of 29 months. Most trials had two treatment groups, and the majority of women enrolled were postmenopausal with visceral metastases and an ECOG performance status of 0 or 1. Approximately 50% of women in these trials had ER-positive tumors. In six trials, trastuzumab was given with chemotherapy to patients with HER2-positive tumors in at least one treatment group, and there were two trials in which all patients enrolled were HER2-positive and all received trastuzumab with chemotherapy. One trial had not reached median OS in one of its treatment groups at the time of reporting.45 Similarly, the follow-up was insufficient for the 25th percentile and 10th percentile to be obtained from the OS curves in 13 and 27 trials, respectively. The mean value and interquartile range (IQR) for median PFS was 7.6 months (IQR, 6.0 to 9.0 moths), for median postprogression survival was 14.0 months (IQR, 10.8 to 15.6 months), for median OS was 21.7 months (IQR, 18.2 to 24.0 months), and for the ratio of median OS to median PFS was 3.0 (range, 2.4 to 3.5). The mean value for 1-year survival was 73% (IQR, 69% to 78%), and the mean value for 2-year survival was 45% (IQR, 38% to 50%). The mean value for © 2010 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 457 Kiely et al Table 1. Characteristics of the 36 Included Trials Trials With Information on Patient Characteristics References (n = 284) Trials Characteristic Insufficient information (n = 30; 10.6%) Not randomized chemotherapy trials in MBC (n = 67; 23.6%) Duplicate references for the same study (n = 22; 7.7%) Not first line (n = 71; 25%) < 90 patients/arm (n = 48; 16.9%) No OS curve (n = 19; 6.7%) Total included (n = 27; 9.5%) Fig 2. Reasons for exclusion of trials. MBC, metastatic breast cancer; OS, overall survival. 5-year survival was 12% (IQR, 7% to 17%), but this information was available in only 14 trials (39%). The distribution of the survival times for each of the selected percentiles (scenarios) is shown in Figure 3. Each distribution was roughly symmetrical with a skew to the right (toward longer survival times). Most values for each scenario fell within a relatively narrow range, indicating the remarkable similarity of survival times among these trials. The mean value for each of the scenarios was worst-case, 6.3 months (IQR, 4.8 to 7.5 months); lower-typical, 11.9 months (IQR, 9.9 to 13.2 months); upper-typical, 36.2 months (IQR, 31.1 to 458 © 2010 by American Society of Clinical Oncology Trial characteristics Year of publication 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 No. of treatment groups compared per trial 2 3 4 Agents used in the 78 treatment groups Anthracycline Taxane Cyclophosphamide Fluorouracil Trastuzumab Carboplatin Methotrexate Gemcitabine Vinorelbine Lapatinib Bevacizumab Capecitabine Patient characteristics No. of patients per group Median Range Age, years Median Range Follow-up, months Median Range Adjuvant chemotherapy, % Median Range ECOG performance status ⬍ 2, % Median Range ER-positive tumors, % Median Range Visceral metastases, % Median Range Premenopausal patients, % Median Range Palliative endocrine therapy, % Median Range No. % 3 3 6 3 3 5 3 3 1 4 2 8 8 17 8 8 14 6 8 3 11 6 31 4 1 86 11 3 50 40 27 18 12 5 3 2 2 1 1 1 64 51 35 23 15 6 4 3 3 1 1 1 No. % 36 100 32 89 23 64 32 89 30 83 28 78 27 75 18 50 11 31 143 90-385 55 50-60 29 10-102 41 4-100 91 66-100 47 16-73 65 40-83 31 0-54 31 4-54 Abbreviations: ECOG, Eastern Cooperative Oncology Group; ER, estrogen receptor. JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 Estimating Scenarios for Survival for Metastatic Breast Cancer Frequency Distribution of Worst Case (90th Percentile) From 78 Curves 30 24 18 12 6 0 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 78 84 90 Time (months) Frequency Distribution of Lower Typical (75th Percentile) From 78 Curves 30 24 18 12 6 0 0 6 12 18 24 30 36 42 48 54 60 66 72 Time (months) Frequency Distribution of Median Survival From 77 Curves 30 24 18 12 6 0 Fig 3. Distribution for survival. 0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 78 84 90 78 84 90 of scenarios Time (months) Frequency Distribution of Upper Typical (25th Percentile) Survival From 58 Curves 30 24 18 12 6 0 0 6 12 18 24 30 36 42 48 54 60 66 72 Time (months) Frequency Distribution of Best Case (10th Percentile) Survival From 26 Curves 30 24 18 12 6 0 0 6 12 18 24 30 36 42 48 54 60 66 72 Time (months) 41.3 months); and best-case, 55.8 months (IQR, 47.5 to 60.2 months). The median and mean times for each percentile (scenario) were almost identical. Simple multiples of the median provided accurate estimates of the selected percentiles (scenarios) for most survival curves: 0.25 ⫻ median accurately estimated the 90th percentile (worst-case) in 73% of curves, 0.5 ⫻ median accurately estimated the 75th percentile (lower-typical) in 97% of curves, 2 ⫻ median accurately estimated the 25th percentile (upper-typical) in 95% of curves, and 3 ⫻ median accurately estimated the 10th percentile (best-case) in 96% of curves. www.jco.org The accuracy of using simple multiples of the median survival was independent of the duration of median survival. Table 2 summarizes associations between the characteristics of each trial and its median OS. Longer median OS was associated with using trastuzumab to treat women with HER2-positive tumors, with using taxane-based chemotherapy, and with having a higher proportion of women with ER-positive tumors. The median OS in the two trials of women with HER2-positive tumors receiving trastuzumab was 16.2 months longer than the median OS in the 29 trials of women with tumors of unknown HER2 status not © 2010 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 459 Kiely et al Table 2. Associations Between Trial Characteristics and Median Survival Trial Characteristic Parameter Estimateⴱ All patients were HER2-positive and receiving trastuzumab† All patients receiving taxane chemotherapy‡ Percentage ER positive Percentage ECOG performance status ⬍ 2 Year of publication Percentage of patients with adjuvant chemotherapy Percentage of premenopausal patients Percentage of patients with visceral disease Median age of patients, years 16.2 5.8 0.3 0.2 0.5 0.1 0.1 ⫺0.05 0.02 95% CI Pearson’s Correlation Coefficient P 7.4 to 25.1 1.7 to 9.9 0.1 to 0.4 ⫺0.1 to 0.5 ⫺0.2 to 1.3 ⫺0.05 to 0.2 ⫺0.1 to 0.4 ⫺0.3 to 0.2 ⫺1.0 to 0.9 0.57 0.50 0.58 0.27 0.24 0.24 0.29 ⫺0.09 0.01 .001 .007 .001 .15 .16 .19 .24 .66 .97 Abbreviations: HER2, human epidermal growth factor receptor 2; ER, estrogen receptor; ECOG, Eastern Cooperative Oncology Group. ⴱ Number of months difference in median overall survival associated with a one-unit increase in trial characteristic. †Compared with trials in which all patients had HER2 status of unknown/negative and received no trastuzumab. ‡Compared with trials in which no patients received taxanes. receiving trastuzumab (95% CI, 7.4 to 25.1 months; P ⫽ .001). Median OS in 14 trials in which all patients received a taxane was 5.8 months longer than in 14 trials in which no patients received a taxane (95% CI, 1.7 to 9.9 months; P ⫽ .007). For every 10% increase in the proportion of women with ER-positive tumors, the median OS increased by 2.5 months (95% CI, 1.1 to 3.8 months; P ⫽ .001). No other trial characteristics were significantly associated with survival. There were insufficient data to perform reliable multivariable analyses. DISCUSSION OS curves were remarkably similar in these trials of first-line chemotherapy for MBC published in the last 10 years. For most of the OS curves, simple multiples of each curve’s median provided accurate estimates of its percentiles, corresponding to worst-case, typical, and best-case scenarios. This meant that for most OS curves, the survival time for the 10% of patients in the worst-case scenario could be accurately estimated as about one quarter of its median or less, the survival of the middle 50% of patients (75th to 25th percentiles, typical scenario) was accurately estimated as ranging from about half to double its median, and the survival time for the 10% of patients in the best-case scenario was accurately estimated as about three times its median or more. In these trials of first-line chemotherapy for MBC, the median OS was typically about three times the median PFS. These observations provide a basis for simple rules of thumb that doctors can use to help estimate and explain life expectancy to women with MBC who are starting chemotherapy. On the basis of prior work,5 we expected and found that the survival curves in this review were flatter at the ends and steeper in the middle than a true exponential curve, and the less extreme multiples of the median were thus appropriate for estimating the 10th and 90th percentiles. We expressed the accuracy of using simple multiples of the median to estimate other percentiles of a given survival curve in terms of how often the estimate was within 0.75 to 1.33 times the actual value. This criterion for accuracy is arbitrary but was specified a priori on the basis of clinical judgment and is symmetrical on a logarithmic scale, as is appropriate for a ratio of two values 460 © 2010 by American Society of Clinical Oncology (estimated:observed). Accuracy was lowest for the worst-case scenario in which multiplying the median by 0.25 tended to underestimate survival. This underestimation probably reflects the exclusion from trials of patients with an obviously poor prognosis, for example by requiring a life expectancy of at least 3 months as an inclusion criterion. The simple multiple of 0.25 is probably still reasonable for routine clinical practice in which patients with a shorter life expectancy are not excluded. This review has important clinical implications. Questions about life expectancy are frequently asked and are difficult to answer, and many patients have a poor understanding of their prognosis.46 There is ample literature providing guidance on how to communicate about prognosis2,47-49 but little on how to estimate life expectancy. This lack of guidance and information is one of the reasons that has been proposed for doctors’ reluctance to discuss prognosis.4,50 On the basis of this review and our previous work, we suggest that questions such as “How long have I got?” are best answered by providing worst-case, typical, and best-case scenarios that are based on simple multiples of the estimated median survival of a group of similar patients. The ideal source of an estimated median survival for a group of similar patients would be a population-based study of similar patients using similar treatments. In the absence of such ideal data, pertinent clinical trials provide a pragmatic and readily available starting point. However, patients in clinical trials are not representative of those seen in routine clinical practice, so adjustments may be required to account for differences that might influence their outcomes. These adjustments may only need to be small for the majority of patients who would meet all or most eligibility criteria for clinical trials. For example, the distribution of median survival times in this review was quite narrow, with 90% of values falling between 16 and 28 months. Patients with characteristics associated with a poor prognosis, such as brain metastases or poor performance status, are often excluded from clinical trials and would require larger adjustments, or preferably different sources of survival data on which to base their survival estimates. Additional studies are needed to determine how survival data from trials should be adjusted for individual patients. Although surveys suggest that the majority of patients with advanced cancer want specific information on the best-case, worst-case, and typical scenarios for their survival,2 patient understanding and JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 Estimating Scenarios for Survival for Metastatic Breast Cancer satisfaction when prognostic information is presented this way has not been assessed, and research in this area is needed. Many patients want realism and honesty from their doctor when discussing prognosis but, at the same time, most also want hope and optimism.48,51,52 We believe estimating and explaining typical, best-case, and worst-case scenarios for survival is preferable to presenting a single-point estimate of the median survival and can help clinicians convey realistic hope. The typical scenario is explained as the most likely outcome, representative of the middle 50% of patients. The best-case scenario is less likely, representing the 10% of patients with the best prognosis, but it is still a possible outcome that can be hoped for. This hope is balanced by presenting the equally possible worst-case scenario, which allows the patient to prepare for the worst. Research is needed to test this belief. We have not attempted to estimate survival from the time of diagnosis of breast cancer or from the time of diagnosis of metastatic disease but acknowledge that these are two other common times for patients to request life expectancy information. The patients in this review will be quite different in terms of their survival time and treatments before beginning palliative chemotherapy, but we have found that after starting chemotherapy, survival times are quite similar. We found that median OS was about three times median PFS (IQR, 2.4 to 3.5 months), as did Saad et al53 in their recent review. This is an observation about summary data from groups of patients, but it raises the hypothesis that doubling the observed time to progression might provide a useful estimate of postprogression survival. If corroborated, a rule of thumb based on this observation might facilitate discussion of prognosis after progression on first-line chemotherapy. The relationship between PFS and OS might also be helpful for planning future studies. This review was not designed to determine individual prognostic and predictive factors in MBC, and individual patient data would be required for this. Prognostic indexes including clinical variables and other measures such as circulating tumor cells can provide more precise information on life expectancy for an individual patient; however, such indexes will never be 100% accurate. Our suggestion to provide patients with estimates for three scenarios could supplement such measures. There will always be best-case, worst-case, and typical scenarios, and it is important to explain these to patients rather than presenting them with a one-point estimate from a prognostic index. It is possible that rules of thumb based on simple multiples could be used to estimate these scenarios from a prognostic index estimate rather than from the median. We did not seek to determine the most effective first-line treatment for MBC; this would require randomized comparisons. Our indirect comparisons of trial characteristics and survival times raise some interesting hypotheses and may help doctors select the most appropriate reference groups on which to base their survival estimates. The treatments associated with the longest OS were trastuzumab in HER2-positive tumors and taxanes. To improve the accuracy of survival estimates for women about to begin trastuzumab and chemotherapy or taxane-based chemotherapy, we suggest doctors start with an OS curve from a pertinent trial that includes these treatments. Although our observations are interesting, they should not be taken as definitive evidence that trastuzumab or taxanes prolong OS. Other characteristics of the patients, treatments, and trials may be responsible, and data from prospective randomized trials are required for such www.jco.org conclusions. There are more appropriate sources of data for determining the effects of trastuzumab and taxanes on survival. The randomized phase III trial by Slamon et al39 reported that the addition of trastuzumab to chemotherapy for women with HER2-positive MBC improved median OS by approximately 5 months. The Cochrane meta-analysis of taxanes in MBC54 reported that taxane-containing regimens significantly prolonged OS; however, when the analysis was restricted to trials of first-line chemotherapy, as in our review, there was no longer a survival benefit. Trials with a higher proportion of women with ER-positive MBC were also associated with longer median OS. Because these patients were not receiving endocrine therapy and many would have exhausted their options for endocrine therapy, this observation supports ER-positive tumors having a more favorable biology regardless of treatment. Whether using simple multiples of the median to calculate estimates of scenarios for survival can be applied to other advanced cancers needs to be determined, but we are encouraged by similar results for advanced non–small-cell lung cancer using the same simple multiples (0.25, 0.5, 2, and 3).9 The accuracy of these rules of thumb will soon be tested by using clinicians’ predictions of survival at baseline in a randomized trial.55 The strengths of this review are that it is comprehensive and applies to contemporary treatment for MBC. It provides simple rules of thumb for doctors to use as a basis to estimate survival times. Although survival estimates will need to be adjusted to account for individual characteristics of the patient, tumor, and treatment, such adjustments probably need only be small for the majority of patients. The main limitation of this review is that it includes only patients in clinical trials who have a better prognosis than patients treated similarly in routine clinical practice. There are few data available on the survival of patients outside clinical trials. We suggest that doctors use median OS from a pertinent clinical trial as a starting point and then adjust that median according to the characteristics of the individual patient at hand. Data on the upper-typical and best-case scenarios were not included in many trials because they were published before these results were mature. This was particularly so in the most recent trials with the longest survival times such as those in women with HER2-positive MBC receiving trastuzumab. Publication of survival outcomes after longer follow-up is needed to provide better founded estimates of long-term survival but, unfortunately, such publications are rare. We did not record information on the durations of chemotherapy used in these trials or on second- or subsequent-line chemotherapy used. These factors may affect OS, but a recent meta-analysis of first-line chemotherapy duration suggests effects on survival time are likely to be modest.56 Finally, systematic reviews of this sort are unable to estimate the survival benefits attributable to chemotherapy. Another potential limitation of this review is that the treatments used may not reflect today’s reality, largely because of changes in adjuvant therapy in the last 10 years. Anthracyclines and taxanes are less likely to be used as first-line therapy today because many patients will have received these treatments in the adjuvant setting. Similarly, more targeted treatment options are becoming available and will hopefully lead to longer OS times in subgroups of patients. Even if the median survival times increase with improved treatments, we expect the multiples of the median to remain accurate for estimating scenarios for survival. This is because it was accurate for most of the 78 © 2010 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 461 Kiely et al survival curves in this review, even though the treatments used in each trial varied. To improve accuracy, we suggest that clinicians select an OS curve from a clinical trial in which patients are randomly assigned to receive similar treatment to that being planned for the patient in question and use the median from this curve as the basis for estimating scenarios. OS distributions from recent randomized trials of first-line chemotherapy in MBC were remarkably similar, approximately exponential, and had a median OS of nearly 2 years, on average. Simple multiples of an OS curve’s median gave good estimates of its percentiles corresponding to worst-case (0.25 times the median), typical (0.5 to 2.0 times the median), and best-case (3.0 times the median) scenarios for nearly all OS curves. Presenting women with estimates for a range of scenarios for survival should provide prognostic information that is more accurate, realistic, and hopeful than a single-point estimate and hopefully easier to understand. REFERENCES 1. Innes S, Payne S: Advanced cancer patients’ prognostic information preferences: A review. Palliat Med 23:29-39, 2009 2. Hagerty RG, Butow PN, Ellis PA, et al: Cancer patient preferences for communication of prognosis in the metastatic setting. J Clin Oncol 22:1721-1730, 2004 3. Fallowfield LJ, Jenkins VA, Beveridge HA: Truth may hurt but deceit hurts more: Communication in palliative care. Palliat Med 16:297-303, 2002 4. Hancock K, Clayton JM, Parker SM, et al: Truth-telling in discussing prognosis in advanced life-limiting illnesses: A systematic review. Palliat Med 21:507-517, 2007 5. Stockler MR, Tattersall MH, Boyer MJ, et al: Disarming the guarded prognosis: Predicting survival in newly referred patients with incurable cancer. Br J Cancer 94:208-212, 2006 6. The Cochrane Collaboration. http://www .cochrane.org/ 7. Wilcken N, Dear R: Chemotherapy in metastatic breast cancer: A summary of all randomised trials reported 2000-2007. Eur J Cancer 44:22182225, 2008 8. UN-SCAN-IT Graph Digitizing Software (ed 6). Orem, UT, Silk Scientific, 1988-2009 9. Alam M, Blinman P, Stockler M: Useful estimates of survival for patients starting first line chemotherapy for advanced non-small-cell lung cancer based on a systematic review of recent randomised trials. 13th World Conference on Lung Cancer, San Francisco, CA, July 31-August 4, 2009 10. Ackland SP, Anton A, Breitbach GP, et al: Dose-intensive epirubicin-based chemotherapy is superior to an intensive intravenous cyclophosphamide, methotrexate, and fluorouracil regimen in metastatic breast cancer: A randomized multinational study. J Clin Oncol 19:943-953, 2001 11. Albain KS, Nag SM, Calderillo-Ruiz G, et al: Gemcitabine plus paclitaxel versus paclitaxel monotherapy in patients with metastatic breast cancer and prior anthracycline treatment. J Clin Oncol 26: 3950-3957, 2008 12. Andersson M, Madsen EL, Overgaard M, et al: Doxorubicin versus methotrexate both combined with cyclophosphamide, 5-fluorouracil and tamoxifen in postmenopausal patients with advanced breast cancer: A randomised study with more than 10 years follow-up from the Danish Breast Cancer 462 © 2010 by American Society of Clinical Oncology AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST The author(s) indicated no potential conflicts of interest. AUTHOR CONTRIBUTIONS Conception and design: Belinda E. Kiely, Martin H.N. Tattersall, Martin R. Stockler Collection and assembly of data: Belinda E. Kiely, Yu Yang Soon Data analysis and interpretation: Belinda E. Kiely, Yu Yang Soon, Martin H.N. Tattersall, Martin R. Stockler Manuscript writing: Belinda E. Kiely, Yu Yang Soon, Martin H.N. Tattersall, Martin R. Stockler Final approval of manuscript: Belinda E. Kiely, Yu Yang Soon, Martin H.N. Tattersall, Martin R. Stockler Cooperative Group—Danish Breast Cancer Cooperative Group (DBCG). Eur J Cancer 35:39-46, 1999 13. Epirubicin-based chemotherapy in metastatic breast cancer patients: Role of dose-intensity and duration of treatment. J Clin Oncol 18:3115-3124, 2000 14. Batist G, Ramakrishnan G, Rao CS, et al: Reduced cardiotoxicity and preserved antitumor efficacy of liposome-encapsulated doxorubicin and cyclophosphamide compared with conventional doxorubicin and cyclophosphamide in a randomized, multicenter trial of metastatic breast cancer. J Clin Oncol 19:1444-1454, 2001 15. Biganzoli L, Cufer T, Bruning P, et al: Doxorubicin and paclitaxel versus doxorubicin and cyclophosphamide as first-line chemotherapy in metastatic breast cancer: The European Organization for Research and Treatment of Cancer 10961 Multicenter Phase III Trial. J Clin Oncol 20:31143121, 2002 16. Bishop JF, Dewar J, Toner GC, et al: Initial paclitaxel improves outcome compared with CMFP combination chemotherapy as front-line therapy in untreated metastatic breast cancer. J Clin Oncol 17:2355-2364, 1999 17. Bontenbal M, Creemers GJ, Braun HJ, et al: Phase II to III study comparing doxorubicin and docetaxel with fluorouracil, doxorubicin, and cyclophosphamide as first-line chemotherapy in patients with metastatic breast cancer: Results of a Dutch Community Setting Trial for the Clinical Trial Group of the Comprehensive Cancer Centre. J Clin Oncol 23:7081-7088, 2005 18. Cassier PA, Chabaud S, Trillet-Lenoir V, et al: A phase-III trial of doxorubicin and docetaxel versus doxorubicin and paclitaxel in metastatic breast cancer: Results of the ERASME 3 study. Breast Cancer Res Treat 109:343-350, 2008 19. Conte PF, Guarneri V, Bruzzi P, et al: Concomitant versus sequential administration of epirubicin and paclitaxel as first-line therapy in metastatic breast carcinoma: Results for the Gruppo Oncologico Nord Ovest randomized trial. Cancer 101:704712, 2004 20. Costanza ME, Weiss RB, Henderson IC, et al: Safety and efficacy of using a single agent or a phase II agent before instituting standard combination chemotherapy in previously untreated metastatic breast cancer patients: Report of a randomized study— Cancer and Leukemia Group B 8642. J Clin Oncol 17:1397-1406, 1999 21. Di Leo A, Gomez HL, Aziz Z, et al: Phase III, double-blind, randomized study comparing lapatinib plus paclitaxel with placebo plus paclitaxel as firstline treatment for metastatic breast cancer. J Clin Oncol 26:5544-5552, 2008 22. Ejlertsen B, Mouridsen HT, Langkjer ST, et al: Phase III study of intravenous vinorelbine in combination with epirubicin versus epirubicin alone in patients with advanced breast cancer: A Scandinavian Breast Group Trial (SBG9403). J Clin Oncol 22:2313-2320, 2004 23. Fountzilas G, Dafni U, Dimopoulos MA, et al: A randomized phase III study comparing three anthracycline-free taxane-based regimens, as first line chemotherapy, in metastatic breast cancer: A Hellenic Cooperative Oncology Group study. Breast Cancer Res Treat 115:87-99, 2009 24. Fountzilas G, Kalofonos HP, Dafni U, et al: Paclitaxel and epirubicin versus paclitaxel and carboplatin as first-line chemotherapy in patients with advanced breast cancer: A phase III study conducted by the Hellenic Cooperative Oncology Group. Ann Oncol 15:1517-1526, 2004 25. Harris L, Batist G, Belt R, et al: Liposomeencapsulated doxorubicin compared with conventional doxorubicin in a randomized multicenter trial as first-line therapy of metastatic breast carcinoma. Cancer 94:25-36, 2002 26. Heidemann E, Stoeger H, Souchon R, et al: Is first-line single-agent mitoxantrone in the treatment of high-risk metastatic breast cancer patients as effective as combination chemotherapy? No difference in survival but higher quality of life were found in a multicenter randomized trial. Ann Oncol 13: 1717-1729, 2002 27. Jassem J, Pieńkowski T, Płuzańska A, et al: Doxorubicin and paclitaxel versus fluorouracil, doxorubicin, and cyclophosphamide as first-line therapy for women with metastatic breast cancer: Final results of a randomized phase III multicenter trial. J Clin Oncol 19:1707-1715, 2001 28. Katsumata N, Watanabe T, Minami H, et al: Phase III trial of doxorubicin plus cyclophosphamide (AC), docetaxel, and alternating AC and docetaxel as front-line chemotherapy for metastatic breast cancer: Japan Clinical Oncology Group trial (JCOG9802). Ann Oncol 20:1210-1215, 2009 29. Langley RE, Carmichael J, Jones AL, et al: Phase III trial of epirubicin plus paclitaxel compared with epirubicin plus cyclophosphamide as first-line chemotherapy for metastatic breast cancer: United JOURNAL OF CLINICAL ONCOLOGY Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 Estimating Scenarios for Survival for Metastatic Breast Cancer Kingdom National Cancer Research Institute trial AB01. J Clin Oncol 23:8322-8330, 2005 30. Miller K, Wang M, Gralow J, et al: Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med 357:2666-2676, 2007 31. Nabholtz JM, Falkson C, Campos D, et al: Docetaxel and doxorubicin compared with doxorubicin and cyclophosphamide as first-line chemotherapy for metastatic breast cancer: Results of a randomized, multicenter, phase III trial. J Clin Oncol 21:968-975, 2003 32. Namer M, Soler-Michel P, Turpin F, et al: Results of a phase III prospective, randomised trial, comparing mitoxantrone and vinorelbine (MV) in combination with standard FAC/FEC in front-line therapy of metastatic breast cancer. Eur J Cancer 37:1132-1140, 2001 33. O’Brien ME, Wigler N, Inbar M, et al: Reduced cardiotoxicity and comparable efficacy in a phase III trial of pegylated liposomal doxorubicin HCl (CAELYX/Doxil) versus conventional doxorubicin for first-line treatment of metastatic breast cancer. Ann Oncol 15:440-449, 2004 34. Paridaens R, Biganzoli L, Bruning P, et al: Paclitaxel versus doxorubicin as first-line singleagent chemotherapy for metastatic breast cancer: A European Organization for Research and Treatment of Cancer Randomized Study with cross-over. J Clin Oncol 18:724-733, 2000 35. Parnes HL, Cirrincione C, Aisner J, et al: Phase III study of cyclophosphamide, doxorubicin, and fluorouracil (CAF) plus leucovorin versus CAF for metastatic breast cancer: Cancer and Leukemia Group B 9140. J Clin Oncol 21:1819-1824, 2003 36. Reyno L, Seymour L, Tu D, et al: Phase III study of N,N-diethyl-2-[4-(phenylmethyl) phenoxy] ethanamine (BMS-217380-01) combined with doxorubicin versus doxorubicin alone in metastatic/ recurrent breast cancer: National Cancer Institute of Canada Clinical Trials Group Study MA.19. J Clin Oncol 22:269-276, 2004 37. Robert N, Leyland-Jones B, Asmar L, et al: Randomized phase III study of trastuzumab, paclitaxel, and carboplatin compared with trastuzumab and paclitaxel in women with HER-2-overexpressing metastatic breast cancer. J Clin Oncol 24:27862792, 2006 38. Seidman AD, Berry D, Cirrincione C, et al: Randomized phase III trial of weekly compared with every-3-weeks paclitaxel for metastatic breast cancer, with trastuzumab for all HER-2 overexpressors and random assignment to trastuzumab or not in HER-2 nonoverexpressors: Final results of Cancer and Leukemia Group B protocol 9840. J Clin Oncol 26:1642-1649, 2008 39. Slamon DJ, Leyland-Jones B, Shak S, et al: Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med 344:783-792, 2001 40. Sledge GW Jr, Hu P, Falkson G, et al: Comparison of chemotherapy with chemohormonal therapy as first-line therapy for metastatic, hormone-sensitive breast cancer: An Eastern Cooperative Oncology Group study. J Clin Oncol 18:262-266, 2000 41. Sledge GW, Neuberg D, Bernardo P, et al: Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as frontline chemotherapy for metastatic breast cancer: An intergroup trial (E1193). J Clin Oncol 21:588-592, 2003 42. Fountzilas G, Papadimitriou C, Dafni U, et al: Dose-dense sequential chemotherapy with epirubicin and paclitaxel versus the combination, as firstline chemotherapy, in advanced breast cancer: A randomized study conducted by the Hellenic Cooperative Oncology Group. J Clin Oncol 19:2232-2239, 2001 43. Marty M, Cognetti F, Maraninchi D, et al: Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: The M77001 study group. J Clin Oncol 23:4265-4274, 2005 44. Lueck H, Minckwitz GV, Du Bois A, et al: Epirubicin/paclitaxel (EP) vs. capecitabine/paclitaxel (XP) in first-line metastatic breast cancer (MBC): A prospective, randomized multicentre phase III study of the AGO breast cancer study group. J Clin Oncol 24:18s, 2006 (suppl; abstr 517) 45. Forbes JF, Kennedy J, Pienkowski T, et al: BCIRG 007: Randomized phase III trial of trastuzumab plus docetaxel with or without carboplatin first line in HER2 positive metastatic breast cancer (MBC). J Clin Oncol 24:18s, 2006 (suppl; abstr LBA516) 46. Barnett MM: Does it hurt to know the worst? Psychological morbidity, information preferences and understanding of prognosis in patients with advanced cancer. Psychooncology 15:44-55, 2006 47. Clayton JM, Hancock KM, Butow PN, et al: Clinical practice guidelines for communicating prognosis and end-of-life issues with adults in the advanced stages of a life-limiting illness, and their caregivers. Med J Aust 186:S77, S79, S83-S108, 2007 48. Hagerty RG, Butow PN, Ellis PM, et al: Communicating with realism and hope: Incurable cancer patients’ views on the disclosure of prognosis. J Clin Oncol 23:1278-1288, 2005 49. Helft PR: Necessary collusion: Prognostic communication with advanced cancer patients. J Clin Oncol 23:3146-3150, 2005 50. Lamont EB, Christakis NA: Complexities in prognostication in advanced cancer: “To help them live their lives the way they want to.” JAMA 290: 98-104, 2003 51. Kutner JS, Steiner JF, Corbett KK, et al: Information needs in terminal illness. Soc Sci Med 48: 1341-1352, 1999 52. Davey HM, Butow PN, Armstrong BK: Cancer patients’ preferences for written prognostic information provided outside the clinical context. Br J Cancer 89:1450-1456, 2003 53. Saad ED, Katz A, Buyse M: Overall survival and post-progression survival in advanced breast cancer: A review of recent randomized clinical trials. J Clin Oncol 28:1958-1962, 2010 54. Ghersi D, Wilcken N, Simes J, et al: Taxane containing regimens for metastatic breast cancer. Cochrane Database Syst Rev 2:CD003366, 2005 55. Stockler MR, O’Connell R, Nowak AK, et al: Effect of sertraline on symptoms and survival in patients with advanced cancer, but without major depression: A placebo-controlled double-blind randomised trial. Lancet Oncol 8:603-612, 2007 56. Gennari A, Sormani M, Nanni O, et al: Impact of first-line chemotherapy duration in metastatic breast cancer: A systematic review. J Clin Oncol 28:15s, 2010 (suppl; abstr 1023) ■ ■ ■ www.jco.org © 2010 by American Society of Clinical Oncology Information downloaded from jco.ascopubs.org and provided by at UNIVERSITY LIBRARY UTRECHT on May 2, 2011 from Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 143.121.239.115 463