Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
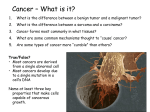
CASE REPORT Primary AdenosquamousCarcinoma of the Liver Which Produces Granulocyte-Colony-Stimulating Factor and Parathyroid HormoneRelated Protein: Association with Leukocytosis and Hypercalcemia Tatsuhiko Hayashi, Akira Mizuki, Takuya Yamaguchi, Tasuku Hasegawa, Takamu Kunihiro, Nobuhiro Tsukada, Kentaro Matsuoka*, Hideki Orikasa* and Kazuto Yamazaki* Abstract parathyroid hormone related protein (PTHrP) are responsible A 55-year-old man was admitted to our hospital with fever and vomiting. Abdominal computed tomography (CT) revealed multiple low density masses in the liver. A diagnosis of primary adenosquamouscarcinoma of the liver was confirmed by histological examination of a necropsy specimen. The present case showed leukocytosis and hypercalcemia with high levels of serum granulocyte-colony-stimu- lating factor (G-CSF) and parathyroid hormone related protein (PTHrP). Recent studies have shown that G-CSF and PTHrPare responsible for the paraneoplastic syndromes with leukocytosis and hypercalcemia. The tumor cells demonstrated positive cytoplasmic immunohistochem- istry staining with anti-G-CSF and anti-PTHrP antibodies. This result suggested that the tumor produced G-CSF and PTHrP. (Internal Medicine 40: 631-634, 2001) Key words: primary liver tumor, paraneoplastic syndrome, cytokine for these types of paraneoplastic syndromes. Wereport here a rare case of primary adenosquamouscarcinoma of the liver associated simultaneously with leukocytosis and hypercalcemia, with some discussion of the literature. Case Report A55-year-old manwas admitted to our hospital for a lowgrade fever and vomiting on June 5, 1999. He had no history of blood transfusion. His family history was not contributory. On physical examination, his body temperature was 37.8°C, his blood pressure was 140/72 mmHg,and his pulse rate was 74/ min and regular. There was no jaundice. Cervical and supraclavicular lymph nodes were not palpable. Abdominal examination revealed a tender liver, extending seven finger-breadths belowthe right costal margin. Therewasno ascites. Table 1 shows the laboratory values on admission. Erythrocyte sedimentation rate (ESR) was 106 mm/h and C-reactive protein (CRP) was 17 mg/dl. Total white blood cell (WBC) count was 27,500/jil, absolute neutrophil (segment and bands) count (ANC) was 23,500/|il (85.5%). Blast and immature cells were not found in the peripheral blood. Blood chemistry was within Introduction the normal range except for elevated aspartate amionotransferase (AST) and alkaline phosphatase (ALP). Hepatitis B viral surface antigen and hepatitis C viral antibody were negative. The levels of serum a-fetoprotein (AFP) and carcinoembryonic antigen (CEA) were within the normal range. The levels of serum carbohydrate antigen 19-9 (199.7 U/ml, normal range <37 U/ml) and squamous cell carcinoma related antigen (6.6 ng/ml, normal range <1.5 ng/ml) were moderately high. Protein induced by vitamin K antagonist-II (PIVKA-II) was also elevated to 45 mAU/ml(normal range <40 mAU/ml). There was markedly elevated ANC,although no evidence of factor (G-CSF) and active infectious disease was found. His serum G-CSFwas el- Adenosquamous carcinoma (ASC) is a tumor composed of both squamouscell carcinoma and adenocarcinoma components. Primary adenosquamouscarcinoma of the liver is rare. All the reported cases were in an advanced stage and had a poor prognosis. On the other hand, it is well known that the paraneoplastic syndromesof leukocytosis and hypercalcemia sometimesoccur in malignancies. Thecoexistence of leukocytosis and hypercalcemia in certain cancers has been reported ( 14-1 8). Granulocyte-colony-stimulating From the Department of Internal Medicine and *the Department of Pathology, Tokyo Saiseikai Central Hospital, Tokyo Recieved for publication June 15, 2000; Accepted for publication December 1 8, 2000 Reprint requests should be addressed to Dr. Nobuhiro Tsukada, the Department of Internal Medicine, Tokyo Saiseikai Central Hospital, 1 -4- 1 7 Mita, Minatoku, Tokyo Internal 108-0073 Medicine Vol. 40, No. 7 (July 2001) 631 Hayashi et al Tablel. Laboratory Data on Admission Erythrocyte sedimentation rate Hematology White blood cell Segment Band Lymphocyte Monocyte Eosinophil Basophil Red blood cell 1 06 mm/h Blood Chemistry Total protein 6. 9 g/dl 27,500/^,1 Albumin 84% Sodium 1.5% Potassium 5 % Chloride 6.5% Calcium 3% Blood urea nitrogen 0% Creatinine 390x l 04/|al Total bilirubin 2.9 g/dl 1 35 mEq// 3.6 mEq// 95 mEq// 1 2.6 mg/dl 1 2 mg/dl 0. 6 mg/dl 0.8 mg/dl Hemoglobin 8.5 g/dl Aspartate aminotransferase Hematocrit 26.3 % Alanine aminotransferase Platelet 493x 1 OVjxl Lactate dehydrogenase Serology Alkaline phosphatase C-reactive protein 1 7 mg/dl y-Glutamyltranspeptidase Hepatitis B viral surface antigen (-) Cholinesterase Hepatitis C viral antibody (-) Others Tumor marker G-CSF oc-fetoprotein 1.2 ng/ml PTHrP Carcinoembryonic antigen 1.4 ng/ml Intact PTH Carbohydrate antigen 19-9 199.7 U// Interleukinl a SSC 6.6 ng/ml Interleukinl p PIVKA-II 45 mAU/ml Interleukin-6 36 IU// 24 IU// 246 IU// 654 IU// 45 IU// 1 ,6 1 0 IU// 79 pg/ml l O PMol// 6 pg/ml 10.5 pg/ml <10 pg/ml 95.7 pg/ml G-CSF: granulocyte-colony-stimulating factor, PTHrP: parathyroid hormone related protein, intact PTH: intact parathyroid hormone, SSC: squamous cell carcinoma related antigen, PIVKA-II: protein induced by vitamin K antagonist -II. evated to 79 pg/ml (normal range <6-21 pg/ml). The serum level of interleukin la (10.5 pg/ml, normal range <7.8 pg/ml) and interleukin 6 (95.7 pg/ml, normal range <4 pg/ml) were high, while interleukin lp (<10 pg/ml) was within the normal range. On August 2, 1999, his serum level of calcium was elevated to 12.6 mg/dl and the serum level of PTHrP was high ( 10 PMol//, normal range <0.6 PMol//), while serum intact PTH was low (6 pg/ml, normal range 10-65 pg/ml). Computed tomograghy (CT) showed multiple nodules located in the anterior and medial segment of the liver (Fig. 1). A fine-needle biopsy of the liver tumor revealed squamous cell carcinoma. Since there wasno evidence of other primary sites, a diagnosis of primary squamous cell carcinoma of the liver was made. However, because of the rapid development of the liver tumor, the patient died of liver failure 64 days after admission to the hospital. Uponautopsy, the liver weighed 4,300 g, and showed a solid whitish tumor, 5 cmin diameter, located in the anterior segment of the liver, with diffuse small nodules invading into two lobes (Fig. 2). Histologic examination revealed that the liver tumor was composedmainly of squamous cell carcinoma and partly of focal areas of adenocarcinoma (Fig. 3). No carcinomas were found in the gallbladder, stomach, pancreas or other organs. Finally, a diagnosis of primary ASCwas confirmed. In addition, the tumor was immunostained using antisera against G-CSF (Fig. 4) and PTHrP (Fig. 5). Some tumor cells were positively stained. This demonstrated that the tumor produced G-CSF and PTHrP. 632 Figure 1. Abdominal computed tomography scan showed multiple low density masses in the anterior and medial segment of the liver. Discussion Adenosquamouscarcinoma (ASC) is a tumor which is composed of elements of both adenocarcinoma and squamous cell carcinoma. Since the description of Pianzola and Drut in 1971 (1), only 34 cases (including the present case) of a primary Internal Medicine Vol. 40, No. 7 (July 2001) G-CSFand Hepatic AdenosquamousCarcinoma Figure 2. Uponautopsy, the liver demonstrated a solid whitish tumor, 5 cm in diameter, located in the anterior segment, with diffuse small nodule invasion into two lobes. Figure 4. Immunostaining of the tumor tissue with monoclonal anti -G-CSF antibodies demonstrated positive cytoplasmic stain- Figure 3. Microscopic findings of the tumor obtained from the autopsy showed both squamous cell carcinoma and adenocarcinomacomponents. HEstain, x75. Figure 5. Immunostaining of the tumor tissue with monoclonal anti-PTHrP antibodies demonstrated positive cytoplasmic staining of the tumor cells. Avidin-biotin peroxidase complex method, xl50. liver tumorwith similar composite histology of areas of adenocarcinoma and squamouscell carcinoma, such as ASC, mucoepidermoidcarcinoma or adenoacanthoma, have been reported (2-4). Amongthose 34 cases, ASC was found in only 26 cases, including the present case, with definitive histological studies. This histologic type of hepatic ASCis not consistently found in a particular site within the liver and shows no evidence of being related to hepatitis virus. ASC typically develops in the gallbladder, the extrahepatic bile duct, or the pan- creas, but rarely in the liver. The diagnosis of primary ASCof the liver should be madewhenboth malignant squamousand glandular elements are present, and primary cancers of the gallbladder, pancreas, extrahepatic bile duct, or lungs should be ruled out. ASCof the liver is currently assumed to originate Internal Medicine Vol. 40, No. 7 (July 2001) ing of the tumor cells. Avidin-biotin xl50. peroxidase complex method, from the intrahepatic bile duct. This tumor is considered to be a subtype of cholangiocarcinoma,whichis not a commontype of liver malignancy. However, the histogenesis of the tumor is still largely unknown.Someinvestigators support the theory that the tumor might develop by transformation of pre-existing adenocarcinoma in the transitional areas between adenocarcinoma and squamous cell carcinoma (5, 6). Concerning the pathogenesis, somereports have demonstrated that ASCis associated with hepatolithiasis (7, 8) or hydatid cysts (1, 9) which have been proposed as etiological factors. But the present case did not have these complications. It is well known that both leukocytosis and hypercalcemia are considered to be paraneoplastic syndromes associated with 633 Hayashi et al a variety of malignancies. Recently, it has been reported that G-CSFis responsible for this kind of paraneoplastic syndrome. More than 200 cases of G-CSF-producing tumors have been reported since Asano et al (10) reported the first case of a patient with lung cancer in 1977. The present case had associated leukocytosis, even in the absence of active infectious diseases, and had an elevated level of serum G-CSF. Positive staining of the tumor cells by immunohistochemistry with monoclonal anti- carcinoma of the liver resected by right trisegmentectomy: Report of a case and review of the literature. J Gastroenterol 32: 843-847, 1997. 3) Miki M, Mizuno Y, Yamaguchi T, et al. Adenosquamous carcinoma of the liver associated with high fever and hypercalcemia. Nippon Shokakigeka Gakkai Zasshi 31: 1559, 1998 (in Japanese). 4) Kurashita Y, Okushima N, Isa T, et al. A case of adenosquamous carcinoma of the liver presenting as liver cystadenocarcinoma. Nippon Shokakibyo Gakkai Zasshi 96: A264, 1999 (in Japanese). 5) Barr RJ, Hancock DE. Adenosquamous carcinoma of the liver. Gastroen- Concerning the biological relationship of G-CSF and tumor growth, it has been reported that G-CSFalso stimulates nonhematopoietic tumor cells. G-CSF-producing tumor cells expressed a G-CSFreceptor which induces tumor cell growth by G-CSFvia the autocrine pathways (1 1). For this reason GCSF-producing tumors usually grow rapidly and the prognosis is extremely unfavorable. Recent studies have shownthat the G-CSF producing tumor is a multi-cytokine-producing tumor which secretes IL-1 and IL-6 in addition to G-CSF(12). IL-1 levels may exceed those of G-CSFand IL-6. The present case also showed elevated serum levels of IL-1 and IL-6. This suggests that IL-1 mayplay an important role in the regulation of G-CSF and IL-6 production in this G-CSF producing hepatic nomaof the liver. Acase report and review of the literature. terology 69: 1326-1330, 1975. G-CSFantibodies revealed that the tumor cells produce G-CSF. 6) Hamaya K, Nose S, Mimura T, Sasaki K. Solid adenosquamous carci- tumor. Jpn 41: 834-840, 1991. Acta Pathol 7) Hu TJ, Chen MF, Jan YY, Chen TJ. Adenosquamous carcinoma of the liver. Report of two cases. Chang Keng I Hsueh ll: 152-159, 1988. 8) Horiuchi T, Sakaguchi M, Oka S, et al. A case report of adenosquamous carcinoma of the liver with hepatolithiasis. Nippon Shokakigeka Gakkai Zasshi 24: 880-884, 1991 (in Japanese). 9) Tokunaga S, Matsuo T, Shimokawa I, et al. An autopsy case of adenosquamous carcinoma of the liver. Shokakigeka 8: 1657-1660, 1985 (in Japanese). 10) Asano S, Urabe A, Okabe T, Sato N, Kondo Y. Demonstration of granulopoietic factors in the plasma of nude mice transplanted with a human lung cancer and in the tumor tissue. Blood 49: 845-852, 1977. 1 1) Tachibana M, Miyakawa A, Tazaki H, et al. Autocrine growth of transitional cell carcinoma of the bladder induced by granulocyte-colony stimulating factor. Cancer Res 55: 3438-3443, 1995. 12) Suzuki A, Takahashi T, Okuno Y, et al. IL-1 production as a regulator of G-CSF and IL-6 production in CSF-producing cell lines. Br J Cancer 65: Furthermore, hypercalcemia also occurred in the present 515-518, 1992. case. His serum PTHrPlevels were elevated. PTHrPhas been 13) Broadus AE, Ikeda K, et al. Humoral hypercalcemia of canidentified as a major causative peptide for hypercalcemia in cer. IdentificationManginof M, a novel parathyroid hormone-like peptide. N Engl J malignancies (13). The immunohistochemistry study of the Med 319: 556-563, 1988. present tumor tissue demonstrated positive staining for PTHrP. 14) Yoneda T, Nishimura R, Kato I, Ohmae M, Takita M, Sakuda M. FreThis suggests that the tumor produces PTHrPwhich is respon- quency of the hypercalcemia-leukocytosis syndrome in oral malignansible for hypercalcemia. The concomitant existence of leuko- cies. Cancer 68: 617-622, 1991. cytosis and hypercalcemia has been reported in cancers of the 1 5) Yazawa S, Toshimori H, Nakatsuru K, Katakami H, Takemura J, Matsukura S. Thyroid anaplastic carcinoma producing granulocyte-colony-stimulatoral mucosa (14), thyroid (15), lungs (16), gallbladder (17), ing factor and parathyroid hormone-related protein. Intern Med34: 584588, 1995. and cholangiocarcinoma (18). It is still uncertain whether leukocytosis and hypercalcemia are complicated randomly or if 16) Sakamoto A, Katakami H, Mukae H, et al. Simultaneous production of there are some factors commonlyregulating them. IL-l is a parathyroid hormone-related protein (PTHrP) and granulocyte-colonyfactor (G-CSF)in lung cancer patient with hypercalcemia osteoclast-activating factor which causes hypercalcemia syn- stimulating and leukocytosis. Nippon Kyobu Shikkan Gakkai Zasshi 33: 34-38, 1995 ergistically with PTHrP (19). IL- 1 is also a hemopoetin- 1 , which Japanese). potentiates G-CSF-induced leukocytosis. Sato et al (19) re- 17)(in Kuroki M, Uto H, Ido A, et al. A case of gallbladder cancer producing ported that IL-1a has dual effects on the development of leu- granulocyte-colony-stimulating factor and possible parathyroid hormone kocytosis and hypercalcemia. However, the detailed mecha- related protein. Nippon Shokakibyo Gakkai Zasshi 97: 478-483, 2000 Japanese). nism of hypercalcemia-leukocytosis syndromeis not clear. In 18)(in Aizawa M, Koshiyama H, Inoue D, et al. Postoperative aggravation of order to elucidate it, further investigation will be necessary. hypercalcemia-leukocytosis syndromein a case of squamouscell type References 1) Pianzola LE, Drut R. Mucoepidermoid carcinoma of the liver. AmJ Clin Pathol 56: 758-761, 1971. cholangiocarcinoma. Intern Med 36: 232, 1997 (letter). 19) Sato K, Fuji Y, Kakiuchi T, et al. Paraneoplastic syndrome of hypercalcemia and leukocytosis caused by squamouscarcinoma cells (T3M-1)pro- ducing parathyroid hormone-related protein, interleukin la, and granulocyte-colony-stimulating factor. Cancer Res 49: 4740-4746, 1989. 2) Takahashi H, Hayakawa H, Tanaka M, et al. Primary adenosquamous 634 Internal Medicine Vol. 40, No. 7 (July 2001)