Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Vision therapy wikipedia , lookup
Visual impairment wikipedia , lookup
Idiopathic intracranial hypertension wikipedia , lookup
Contact lens wikipedia , lookup
Keratoconus wikipedia , lookup
Eyeglass prescription wikipedia , lookup
Retinitis pigmentosa wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
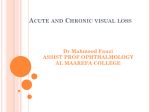
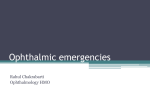
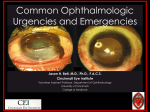
2003.1 VAQ 6 Quiz Clinical 021 CJJ06 Scenario A 19 year old female presents with a painful right eye and decreased vision after being out for most of the night previously at clubs. She is normally myopic. Her visual acuity is 6/24 in her right eye and 6/12 in her left eye. 1. List 3 possible causes for the above lesion a. Trauma i. Blunt/Penetrating ii. Chemicals iii. Contact lens b. Infections- bacterial , viral, fungal , contaminated medications 2. Outline steps in further management. a. Analgesia –oral & local b. Corneal sensation testing c. Slit lamp examination with Fluorescing testing Defects, Seidel’s sign i. Slit lamp exam –epithelial layer, Stroma, Endothelial layer , corneal oedema, infiltrates in AC etc. d. Corneal scrapes e. Intraocular pressure f. Refer to ophthalmologist i. Pachmetry ii. Specular microscopy iii. Cornea topography g. Antibiotics / Antiviral +-Cycloplegics 3. Pseudomonas cover with Fluoro quinolones if contact lens wearer i. Viral … -keratitis HSV, V2V….corneal …. - …epithelium …… Most bacteria can cause only if…the is breached except – N gonorrhoea & H influenza . Viral Keratitis is caused by HSV, VZV( Herpes zoster ophthalmicus) A 50 YO woman presents with a monocular visual loss. 1: List your differential diagnosis. 2: For each differential give 2 features of history and 2 features of examination that would be supportive 3: What are your treatment priorities for central retinal arterial occlusion? 1: Central Retinal Artery Occlusion (Hx: sudden painless profound visual loss, recent amaurosis fugax episodes, vascular risk factors. Ex: Severly reduced VA effected eye, RAPD, fundoscopy: pale retina, cherry red spot) 2: Ischaemic optic neuropathy (eg Giant cell arteritis) Hx: Polymyalgia rheumatic, Jaw claudication, headaches, scalp tenderness, Profound visual loss. Ex: Temporal artery tenderness, RAPD, oedematous optic disk on fundoscopy 3: Retinal Detachment Hx- Flashes and floaters, Shade / curtain. Associated trauma sometimes Ex- Variable VA / RAPD depending on size, Visual field defect. 4: Vitreous Haemorrhage. Hx: Proliferative diabetic retinopathy, trauma, blurred vision of variable severity Ex: Variable VA, Loss of red reflex. No RAPD unless associated retinal detatchment 5: Optic Neuritis: Eg: MS young women, Subacute visual loss, (over days) pain on eye movement Ex: Disk oedema, RAPD, 6: Central Retinal Vein occlusion. Subacute variable visual loss, variable RAPD, VA, blood and thunder retina. CRAO – Rx Urgent ophthalmology advice and referral Poor evidence for intervention but try -Pulsed ocular massage -Acetazolamide 500mg PO / IV. -Consider anterior chamber paracentesis in conjunction with ophthalmology. A 30 YO male presents to ED after an assault with a broomstick. He is GCS 15 with no other apparent injury. 1: List 6 important features of this photo 2: What important diagnoses must be considered. Give 2. 3: Outline 5 important features of your examination. 4: Outline your further investigation 5: His VA is light perception only in the effected eye. Outline your management 1: - Dilated pupil. -Proptosis -Marked subconjunctival haemorrhage / bloody chemosis -Periorbital ecchymosis -Small Hyphema -Corneal opacity (?abrasion / laceration) 2: Retro-orbital haemorrhage / orbital compartment syndrome Ruptured globe / Penetrating eye injury 3: VA – marked reduction in VA implies possible optic nerve ischemia and mandates early management Pupillary reaction / RAPD Consistent with optic nerve ischemia Eye movements (? Entrapment ) Tonometry High IOP (>40)consistent with retroorbital haemorrhage, low/ normal with penetrating eye injury Fundoscopy (may see papiloedema) Fleuroscine stain (?corneal abrasion / ? evidence of penetrating injury/ rupture) 4: CT orbit – may confirm diagnosis / delinate associated injury eg Fracture / entrapment. Should not delay treatment if significant reduction in VA. 5: Needs urgent reduction of orbital pressure. Lateral canthotomy is indicated Urgent opthal involvement (ideally they perform procedure) Analgesia Consider procedural sedation in ED to expediate lateral canthotomy. Note: Ruptured globe is a contraindication and needs exclusion first. Ref http://lifeinthefastlane.com/ophthalmology-befuddler-033-2/ Also dunn and exam feedback SAQ 6 a. Compare and contrast the clinical features of pre-septal and orbital cellulitis (6 marks) Pre-septal Orbital cellulitis Infection More superficial (usually skin source) Deep (sinus, dental source) Sight threatening Unlikely Possible Life threatening Unlikely Possible Visual acuity Normal Usually reduced Eye movements Normal Painful/reduced Proptosis No Possible Neurological signs No Possible Organisms Skin (staph) more prevalent Gram negs more prevalent Generally unwell/URTI Possible Possible Toxic, severe headache Unlikely Possible b. List three features essential for managing orbital cellulitis (3 marks) Broad spectrum IV Abs i. Staph cover (eg flucloxacillin, vancomycin alternative) ii. Gram neg cover (3rd generation ceph) Urgent ophthalmology review and admission, consideration of surgical intervention CT to confirm Dx and identify surgically amenable lesions VAQ 2 An 18 year old man presents with right eye pain. There is no history of trauma. His vital signs are: Temp 38oC Pulse 110/min BP 120/80 mmHg SaO2 98% RA A contrast enhanced CT scan is performed – 2 slices are shown. a) Describe 4 features seen on the CT scan (4 marks) Proptosis of right eye and/or retrobulbar oedema Periorbital oedema of right eye Right intra-orbital gas or air/fluid level Right orbital abscess or right orbital (post septal) cellulitus with gas formation b) Outline the important features of the eye examination in this patient (2 marks) Range of movement of eye +/or pain on movement Visual acuity a. List 3 differentials with 3 key symptoms / signs and management in the table below: Differential Symptoms Management 5. a. Differential Acute angle closure glaucoma Symptoms 1. severe pain 2. systemically unwell 3. fixed, semi-dilated pupil Management Acetazolamide 500mg IV stat then 250mg PO q8hr or mannitol Pilocarpine 2% 1drop q5min x 6 then QID Timolol 0.5% 1drop BD +/prednisone 0.5% Analgesia Urgent referral for surgery Acute anterior uveitis 1. photophobia (Iritis) 2. hypopyon 3. small or irregular pupils Urgent referral if hypopyon +/- steroids if no corneal infection Scleritis 1. gradual onset pain 2. thickened sclera with blue nodules 3. associated systemic disease (RA, gout, syphilis, TB, sarcoid, HT, drugs) Analgesia, topic steroids if no infection Cycloplegics Urgent referral 2011-2 New Format VAQs Question 1 A 4 year old boy is brought into your emergency department following an injury sustained to his right eye from a small rubber ball thrown by his brother earlier that day. a) Please describe the photograph (4 marks) b) What is the diagnosis (1 mark) c) What are the potential complications of this injury (4 marks) Question 1 Answers a) Please describe the photograph (4 marks) Blood in anterior chamber: approximately 30 - 40% of chamber height Mild conjunctival injection of right eye Equal pupillary size No other obvious trauma to orbit or peri-orbital area Child not in distress b) What is the diagnosis (1 mark) Small to moderate hyphaema secondary to blunt trauma. c) What are the potential complications of this injury (4 marks) Short to Medium Term - Rebleeding - Decreased visual acuity Pain due to increase IOP Retinal damage (ie retinal detachment) Long term - Glaucoma - Iron pigmentation staining to the cornea References: Dunn’s page 1108 – Ocular Trauma Cameron’s page 610 – Ocular Emergencies VAQ 6 While waiting for the Ct need in the last patient the triage nurse tells you of a 30 year old male waiting to be seen whose child threw a toy soldier at his eye. Question 1 List 2 salient positives and 2 salient negatives in the picture supplied Question 2 What are 3 complications of this injury VAQ 6 Answers Question 1 List 2 salient positives and 2 salient negatives in the picture supplied. Sub conjunctiva haemorrhage Hyphema in the anterior chamber almost obscuring the inferior half of the pupil Pupil looks to be normal shape – but abnormal according to marking scheme. 30% pass rate for this question may have been because the abnormalities were not obvious apart from the hyphema No other surrounding traumatic injury – lid or face laceration, ecchymosis or swelling Question 2 List 3 complications of this injury. Raised intra ocular pressure Glaucoma Optic atrophy , Field loss Corneal opacification References – Cameron, 4th ed page 610, Exam report. VAQ 2 A 25 year old male presents with photophobia, increasing left eye pain and decreased vision Question 1 List 2 important positive and 2 important negatives in this photograph Question 2 As pert of your initial assessment what are 3 salient historical features that you must explore Question 3 What are 3 important examination finding that you will attempt to illicit VAQ 2 Answers Question 1 List 2 important positive and 2 important negatives in this photograph Conjunctival injection Hypophyon – inflammatory cells in the anterior chamber of the eye. Opacified cornea Discharge and the nature of the discharge Question 2 As pert of your initial assessment what are 3 salient historical features that you must explore? Contact lens wearer Previous eye issues, surgery or keratitis Trauma Foreign body Systemic symptoms Question 3 What are 3 important examination finding that you will attempt to illicit? Visual acuity Pupils reaction to light Slit lamp exam and fluorocene staining References – Exam report.