Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
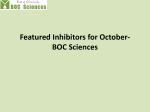
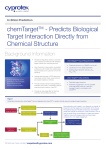
NEW MODEL OF NONCLINICAL CARDIAC RISK ASSESSMENT Kramer JK1, Myatt, GJ.2; Obejero-Paz, C.1, Bruening-Wright, A.1 Brown AM. 1ChanTest Corp., Cleveland, OH, USA. 2Leadscope Inc., Columbus, OH, USA 2.) hERG Is Not The Best Predictor of TdP When Drug Affects Multiple APD30 Shortened 0 APD30 is Shortened 1.E+00 -30 1.E‐01 hERG IC50 1.E‐02 0.9 APD Prolonged -60 hERG IC50 1.E‐01 Prolonged -80 -90 0s 1.E‐03 400 ms 0s 1.E‐03 Terfenadine APD60 is Unchanged APD90 Prolonged APD 90 is ETPC 1.E‐02 ETPC -40 Cav1.2 IC50 400 ms 800 ms Verapamil True Positive Ratee (sensitivity) Ion Chann nel IC50 (μM) Ion Chan nnel IC50 (μM) 0 Contingency Table 40 1.E+01 Nav1.5 IC50 Model Based on Multiple Ion Channel Effects Is More Predictive of TdP 1.0 30 Cav1.2 IC50 1.E+00 4.) Verapamil Blocks hERG and Cav1.2 Verapamil Blocks hERG and Cav1.2 and has Mixed Effects on SC‐HCM AP and has Mixed Effects on SC‐HCM AP 1.E+02 Nav1.5 IC50 1.E+01 0.8 0.7 Model 1 0.6 0.5 0.4 No Discrimination; AUC = 0.5 0.3 Model 2; AUC = 0.88 0.2 0.1 Model 2 0.0 Many torsadogenic drugs potently and selectively inhibit hERG ion channel current. current However, However hERG blockers that have effects on multiple ion channels, are not always torsadogenic. Verapamil, which is used to treat high blood pressure and angina, is a multiple ion channel blocker that inhibits hERG very potently (IC50 = 143 nM). Verapamil inhibits the two major depolarizing currents ICaL and INa offsetting the hERG block and avoiding delayed repolarization. There are no reported incidents of TdP since it has been on the market. Compounds that have multiple ion channel effects should be identified as early as possible during drug development. +TdP and –TdP Drugs Characterized by Their Ion Channel g y IC50/ETPC Profiles 3.)) Torsadogenic Compounds 1000000 100000 100000 10000 10000 Vanoxerine Risperidone Ranolazine Quetiapine Propranolol Propafenone Phenytoin Pentobarbital Nitrendipine Nifedipine Mibefradil Mexiletine Methadona Diltiazem Diazepan Desipramine 0.001 Cibemzoline 0.01 Amitriptyline Ziprasidone Thioridazine Terfenadine Tedisamil Sotalol Sertindole Sematilide Quinidine Prenilamine Pimozide Moxifloxacin Ibutilide Haloperidol Defetilide Cisapride Bepridil 0.1 Astemizole 0.001 0.4 0.6 0.8 False Positive Rate (1‐specificity) False Positive Rate 1.0 We created two predictive logistic regression models: The first model was developed with hERG IC50/ETPC data and the second with hERG IC50/ETPC + Nav1.5 IC50/ETPC + Cav1.2 IC50/ETPC data. Cross validation of each model was performed to classify drugs as being +TdP or ‐TdP. The first logistic regression model using only hERG data poorly classified the drugs, displaying an overlapping of the +TdP and –TdP groups, 11 false positives and 1 false negative. In contrast, the second model effectively separated the +TdP and –TdP groups and resulted in only 3 false positives and 2 false negatives. negatives 1 Imipramine 0.1 0.01 0.2 Conclusions: 10 Fluvoxamine 1 TdP‐ 3 False Positives 18 True Negatives 100 Diphenhydramine 30 fold greater than ETPC IC50/ETPC 10 TdP+ 18 True Positives 2 False Negatives 30 fold greater 30 f ld t than ETPC 1000 100 Verapamil 1000 TdP‐ 11 False Positives 10 True Negatives Receiver Operator Characteristic (ROC) for Model 1 (green circles) and Model 2 (blue circles) were constructed by plotting the false positive rate (false positives )/(false positives + true negatives)) and true positive rate (true positives)/(true positives +false negatives)) at each cross‐validated probability (shown in the box plots above). The solid line is the theoretical result for a test that does not discriminate between the two groups (the area under the curve (AUC) = 0.5). The logistic regression model derived from hERG IC50/ETPC alone is not a good TdP predictor since a 90% True Positive Rate is associated with a 52% False Positive Rate (AUC = 0.74). Encouragingly, the inclusion of Nav1.5 and Cav1.2 parameters results in a significant increase in predictivity by reducing the False Positive Rate to 14% while maintaining a True Positive Rate of 90% (AUC = 0.88). Non‐Torsadogenic Compounds 1000000 TdP+ 19 True Positives 1 False Negative Model 1; AUC = 0.74 0.0 Amiodarone The challenge is to identify drugs early in development that may cause torsade de pointes (TdP), a serious polymorphic ventricular y that can lead to sudden death. The frequency q y of TdP mayy tachycardia be <10‐6 for non‐cardiac drugs cannot be reliably detected in clinical trials. The risk of sudden death may become apparent only during marketing surveillance. QT prolongation has been chosen as a surrogate marker for TdP because TdP is always associated with a prolonged QT interval but the QT‐TdP linkage is incomplete and the predictivity is weak. Impaired predictivity remains even under the minimal safety strategy laid out in the ICH S7B industry guidance. This guidance for evaluating delayed repolarization emphasizes testing for inhibition of the hERG potassium channel and QT prolongation in an in vivo assay. assay However, However the S7B preclinical cardiac safety strategy may give internally discordant results and imperfect clinical predictivity making it difficult to determine a compound’s TdP risk. Discordances may be resolved and TdP predictivity increased by following an improved thorough cardiac safety testing strategy that determines effects on multiple cardiac ion channel currents. In this study we demonstrate that characterizing the effects of drugs on Nav1.5 and Cav1.2, in addition to hERG, better predicts whether a drug is torsadogenic. Terfenadine Selectively Blocks hERG Terfenadine Selectively Blocks and Prolongs SC‐HCM AP hERG and Prolongs SC‐HCM AP 1.E+02 Ajmaline Introduction: Ion Channels IC50/ETPC Abstract Drug‐induced inhibition of the cardiac hERG potassium channel is assumed to predict delayed cardiac repolarization (DR). The consequent QTc prolongation is a surrogate marker of torsade de pointes (TdP), a potentially lethal iatrogenic outcome. Drugs with effective therapeutic plasma concentrations (ETPC) within 30‐fold of their hERG IC50s are thought to be dangerous despite the fact that multiple ion channel effects (MICE) can mitigate DR. Here we demonstrate that a logistic regression model, which integrates MICE, predicts TdP with much greater certainty than the hERG safety ratio (hERG IC50/ETPC) alone. Safety ratios were calculated for 41 drugs (20 +TdP and 21 ‐TdP) TdP) from multiple classes by dividing their hERG, Nav1.5 and Cav1.2 IC50 values by each drug’s ETPC. Two logistic regression models were constructed; one using the hERG IC50/ETPC ratio alone (Model 1), the other integrating hERG IC50/ETPC + Nav1.5 IC50/ETPC + Cav1.2 IC50/ETPC data (Model 2). The predictive power of each model was evaluated by performing leave‐one‐out cross validations. Each model’s accuracy for discriminating +TdP and ‐TdP drugs was determined by comparing their receiver–operator characteristics (ROC, true vs. false positive rates). Model 1 had a 52% False Positive Rate associated with a 90% True Positive Rate and a ROC area under the curve (AUC) of 0.74. Model 2 significantly improved accuracy showing a 14% False Positive Rate associated with a 90% True Positive Rate and a ROC AUC of 0.88. We propose that models that incorporate quantitative drug effects on multiple cardiac ion channels will be robust nonclinical predictors of cardiac risk. 1) Some hERG blockers (IC50/ETPC values lower than 30) are safe drugs when they also block calcium and/or sodium currents. 2) Logistic regression models that include multiple ion channels are better predictors of cardiac risk than models including hERG block alone. 1.) The ECG and Cardiac Action Potential are Formed by Many Different Ion Channel Currents. Cardiac Channel Panel™ Nav1.5 (INa) Phase 1 Cav1.2/β2, α2δ, (L‐type) 0 Cav3.2 (T‐type) Phase 2 Kv4.3 (ITO1) ‐30 30 Phase 0 Membrane P Potential (mV) 30 Phase 3 ‐60 Phase 4 ‐90 0 s 100 ms 200 ms 300 ms Time 400 ms 500 ms AP Phase 0, 2 2 1 1 KvLQT1/minK (I Kv QT /minK (IKs) 2 ‐ 3 hERG (IKr) 2 ‐ 3 Kv1.5 (IKur) 2 ‐ 3 Kir2.1 (IK1) 4 HCN2 (pacemaker, If) 4 HCN4 (pacemaker, If) 4 Kir3.1/3.4 (IK,ACh) 4 Kir6.2/SUR2A (IK,ATP) 4 NCX1 (Na‐Ca exchange) 2 Ion channel (hERG, Cav1.2 and Nav1.5) IC50 values for 41 drugs were collected from the literature and ChanTest’s internal database. The average Effective Therapeutic Plasma Concentrations (ETPC) were collected from the literature or calculated from Cmax and % protein binding values. In the logarithmic plots above, the hERG IC50/ETPC value is the vertex of each line segment, the Nav1.5 IC50/ETPC value is the point at the end of each blue line segment and the Cav1.2 IC50/ETPC is the point at the end of each orange segment. Drugs were characterized as torsadogenic (left panel) or non‐ torsadogenic (right panel) according to information found in Redfern et al. (Categories 1‐3 = +TdP; C Categories i 4‐5 4 5 = ‐TdP), TdP) the h Arizona Ai CERT database d b and d reported d cases. The Th dashed d h d line li shows h Redfern’s criteria of 30 for torsadogenic drugs. One can see that not all of the torsadogenic drugs have hERG IC50 values that are less than 30 fold above the ETPC and some non‐torsadogenic drugs have hERG IC50/ETPC ratios that are less than 30. The plots above reveal that with very few exceptions, the +TdP and –TdP drugs can be qualitatively distinguished from each other by their multi ion channel IC50/ETPC profiles. In general safe drugs have IC50/ETPC values for the depolarizing currents close (within one order of magnitude) to hERG IC50/ETPC values. 3) Drug misclassification is most probably due to inadequacy of TdP classification or drug effects on other channels involved in cardiac excitability.