Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Surround optical-fiber immunoassay wikipedia , lookup
Schistosomiasis wikipedia , lookup
Inflammatory bowel disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
Infection control wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Ulcerative colitis wikipedia , lookup
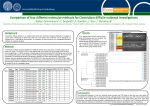
AJCP / Editorial PCR vs “PCAren’t” Limitations of PCR-Based Assays Performed on Formalin-Fixed, Paraffin-Embedded Mucosal Biopsy Specimens Laura Lamps, MD DOI: 10.1309/AJCPWFN9D0EGDEUK Clostridium difficile remains the most common nosocomial cause of diarrhea and is becoming an increasingly important community-acquired infection.1,2 Antibiotic resistance, as well as the recently identified BI/NAP1/027 strain, is responsible for more cases of severe C difficile–associated diarrhea worldwide.3 The diagnosis of C difficile infection is usually based on a combination of history of antibiotic use, the presence of pseudomembranes on colonoscopy, appropriate histology on biopsy, and confirmatory laboratory stool tests for either the C difficile toxin or bacterial toxin genes. Most clinical laboratories employ a C difficile–associated toxin enzyme immunoassay (EIA). These assays are technically easy to perform and have a rapid turnaround time. Although they have specificities ranging from 65% to 100%, the sensitivities are limited, ranging from 31% to 99%.4 Recently, US Food and Drug Administration–approved, polymerase chain reaction (PCR)–based molecular assays performed on stool lysates have been increasingly recognized as the most sensitive and specific methods of diagnosing C difficile. These assays target C difficile toxin genes rather than the toxins themselves, with a sensitivity from 77% to 100% and a specificity from 93% to 99%.5-7 The tissue diagnosis of C difficile in a gastrointestinal mucosal biopsy specimen is generally straightforward, although some infections (eg, enterohemorrhagic Escherichia coli, Shigella, and toxin-producing Clostridium perfringens) may produce similar features both macroscopically and morphologically. Ischemia is frequently in the histologic differential diagnosis as well, and the distinction between the two is extremely important because the treatments are different. In their article in this issue of the American Journal of Clinical Pathology, Wiland and colleagues8 examine the degree of interobserver agreement in the histologic diagnosis © American Society for Clinical Pathology Lamps_2013040207.indd 705 of C difficile colitis and correlate the histologic findings with clinical data. They also evaluate the utility of a PCR-based assay for C difficile when applied to formalin-fixed, paraffinembedded mucosal biopsy specimens. To our knowledge and that of the authors, this article is the first to evaluate the feasibility and usefulness of PCR in detecting C difficile in fixed, processed mucosal biopsy specimens. The authors analyzed 20 mucosal biopsy specimens from patients who had C difficile colitis, with the diagnosis based on histology plus a positive EIA or PCR test, and/or were clinically suspected of having C difficile colitis or responded to treatment for C difficile. Twenty biopsy specimens from patients with ischemic colitis were evaluated in comparison. Punch biopsy specimens from the paraffin blocks of most cases were subjected to DNA extraction and PCR, although a few lacked enough residual tissue for further testing. Wiland et al8 demonstrated overall excellent interobserver agreement in distinguishing between ischemic colitis and C difficile colitis, and there was also good correlation between the consensus histologic interpretation and the clinical impression. The results of the PCR assay performed on the fixed, paraffin-embedded tissue, however, were underwhelming. Only 3 of the 15 cases categorized as C difficile colitis were positive by PCR performed on the tissue block. This study nicely confirms the reliability and reproducibility of the histologic diagnosis of C difficile colitis and emphasizes the good correlation between histologic diagnosis and clinical impression in most cases. It also highlights many of the challenges in using PCR-based assays on fixed, processed biopsy specimens. Analysis of fixed, paraffin-embedded tissue samples with PCR assays is fraught with difficulty, particularly when applied to small biopsy specimens. Wiland 705 Am J Clin Pathol 2013;139:705-707 DOI: 10.1309/AJCPWFN9D0EGDEUK 705 705 5/6/13 10:28 AM Lamps / PCR vs PCAren’t et al8 do not state the size of the target DNA in the commercial assay that they used, but typically the target DNA must be less than 500 base pairs due to DNA fragmentation caused by fixation. Fixatives other than formalin (such as mercuric or picric acid–based fixatives) may limit DNA yield even more. Commercial assays are usually designed for use on fresh or frozen specimens, and the extraction and detection kits may not be designed to handle the tiny quantities of DNA present in many mucosal biopsy specimens. The authors emphasize this technical limitation themselves—the average DNA concentration (ng/L) for their tested formalin-fixed, paraffin-embedded biopsy cases was 70.05 ng/L, yet the average DNA concentration for a comparison group of 10 random stool lysates was significantly greater at 277.70 ng/L and was 105.94 ng/L when excluding 1 outlier control. Finally, lesional tissue in the block may simply be exhausted by the time it is subjected to molecular analysis, and thus sampling error may cause a negative result even when the patient truly has an infection.9 This study also emphasizes the critical importance of correlating molecular data with all available histologic, laboratory, and clinical information. Wiland et al8 give an excellent example of this when they describe one of their cases that was histologically categorized as C difficile colitis, yet the patient tested negative by PCR-based stool assay. Upon clinical review, the patient had multiple convincing risk factors for ischemic colitis. One must bear in mind that the PCR-based stool assays detect C difficile toxin genes but do not necessarily indicate viability of the bacteria and toxin production. A PCR assay also cannot gauge the severity of disease in the same way that a colonoscopy or a biopsy can. Moreover, molecular tests may detect C difficile in stools of colonized patients, but it may not be the cause of diarrheal disease.10 Unfortunately, Wiland et al8 did not provide detailed data regarding the colonoscopic appearance, risk factors for C difficile, or results of molecular assays performed on stool vs EIA for their study cases. Because previous studies10-12 have shown a troubling lack of correlation between clinical, laboratory, and histologic data, the opportunity to see such a correlation in these cases, particularly when combined with the data from the PCR assay performed on the tissue blocks, would no doubt have been interesting. Robust clinicopathologic correlation is important for many reasons in the practice of infectious disease pathology. Few (if any) laboratory assays, including PCR performed on tissue blocks, should be interpreted in a vacuum devoid of clinical and histologic information. The result of the PCR assay must be compared with the findings on the microscopic slide, as well as available clinical and laboratory data. Obviously, the negative PCR results from the tissue blocks in this study do not mean that the patients with histologic and clinical evidence of C difficile colitis were misdiagnosed. Yet, how many of us have had a hallway conversation with a clinical colleague or 706 706 Am J Clin Pathol 2013;139:705-707 medical student that started with, “How can you call it that? The PCR was negative.” This is a particular problem in infections characterized by detection of few organisms. Some cases of mycobacterial infection, for example, contain few bacilli on acid-fast bacilli–stained slides. The PCR assay is often negative in such situations due to lack of sufficient bacterial DNA.9 The PCR-based assays for C difficile detection are somewhat unusual because they are typically performed on stool rather than on tissue. The ability to perform PCR assays for bacterial DNA directly on gastrointestinal mucosal biopsy tissue blocks, however, is extremely important because patients are often placed on empiric antibiotic therapy prior to either mucosal biopsy or stool culture, thus limiting our ability to detect a specific pathogen. Although their attempt met with limited success, Wiland et al8 emphasize the importance of continuing to develop molecular assays for gastrointestinal pathogens that are suitable for use in fixed, paraffin-embedded tissue. Part of our mission as pathologists, laboratorians, and consultants is to educate our colleagues and the public as to the limitations, as well as the advantages, of laboratory technology. This education includes the technical limitations of the assays, as well as the importance of correlating all available clinical and pathologic data when rendering a diagnosis. Many of us are old enough to have witnessed the conflict between technology and tradition with the advent and widespread use of diagnostic immunohistochemistry, as well as heard our clinical colleagues claim that “those brown stains” were a miraculous tool that simply revealed the diagnosis by a color change and had nothing to do with the interpretive abilities of the pathologist. New technology is available all the time, often at a high cost to institutions and patients. Application of molecular technology, while often invaluable, must be done with the knowledge (by both pathologists and clinicians) of the limitations of the test as well as the ability to interpret the test in light of the tissue biopsy results and the clinical data. The study by Wiland et al8 serves as a reminder that even the most sophisticated technology has limitations and is best interpreted in the context of the entire clinicopathologic picture. It is also a reaffirmation of pathologists’ ability to make an accurate diagnosis of C difficile colitis. To paraphrase a quote attributed to Hans Popper, the best diagnostic tool is still a good-quality H&E slide connected to a brain. From the Department of Pathology, University of Arkansas for Medical Sciences, Little Rock. References 1. Cohen S, Gerding D, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431-455. © American Society for Clinical Pathology DOI: 10.1309/AJCPWFN9D0EGDEUK Lamps_2013040207.indd 706 5/6/13 10:28 AM AJCP / Editorial 2. Dumyati G, Stevens V, Hannett GE, et al. Communityassociated Clostridium difficile infections, Monroe County, New York, USA. Emerg Infect Dis. 2012;18:392-400. 3. Lessa FC, Gould CV, McDonald LC. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(suppl 2):S65-S70. 4. Crobach MJ, Dekkers OM, Wilcox MH, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): data review and recommendations for diagnosing Clostridium difficile-infection (CDI). Clin Microbiol Infect. 2009;15:1053-1066. 5. Viala C, Le Monnier A, Maataoui N, et al. Comparison of commercial molecular assays for toxigenic Clostridium difficile detection in stools: BD GeneOhm Cdiff, XPert C. difficile and illumigene C. difficile. J Microbiol Methods. 2012;90:8385. 6. Chapin KC, Dickenson RA, Wu F, et al. Comparison of five assays for detection of Clostridium difficile toxin. J Mol Diagn. 2011;13:395-400. 7. Curry S. Clostridium difficile. Clin Lab Med. 2010;30:329-342. © American Society for Clinical Pathology Lamps_2013040207.indd 707 8. Wiland HO, Procop GW, Goldblum JR, et al. Interobserver variability and feasibility of polymerase chain reaction–based assay in distinguishing ischemic colitis from Clostridium difficile colitis in endoscopic mucosal biopsies. Am J Clin Pathol. 2013;139:730-735. 9. Thangappah RB, Paramasivan CN, Narayanan S. Evaluating PCR, culture & histopathology in the diagnosis of female genital tuberculosis. Indian J Med Res. 2011;134:40-46. 10. Wilcox MH, Planche T, Fang FC, et al. What is the current role of algorithmic approaches for diagnosis of Clostridium difficile infection? J Clin Microbiol. 2010;48:4347-4353. 11. Guarner J, Bhatnagar J, Shane AL, et al. Correlation of the detection of Clostridium difficile toxins in stools and presence of the Clostridia in tissues of children. Hum Pathol. 2010;41:1586-1592. 12. Johal S, Hammond J, Solomon K, et al. Clostridium difficile associated diarrhoea in hospitalised patients: onset in the community and hospital and role of flexible sigmoidoscopy. Gut. 2004;53:673-677. 707 Am J Clin Pathol 2013;139:705-707 DOI: 10.1309/AJCPWFN9D0EGDEUK 707 707 5/6/13 10:28 AM