Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
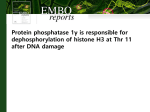
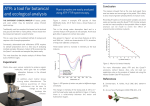
Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Clinical Cancer Research Review Achieving Precision Death with Cell-Cycle Inhibitors that Target DNA Replication and Repair Aimee Bence Lin1, Samuel C. McNeely2, and Richard P. Beckmann3 Abstract All cancers are characterized by defects in the systems that ensure strict control of the cell cycle in normal tissues. The consequent excess tissue growth can be countered by drugs that halt cell division, and, indeed, the majority of chemotherapeutics developed during the last century work by disrupting processes essential for the cell cycle, particularly DNA synthesis, DNA replication, and chromatid segregation. In certain contexts, the efficacy of these classes of drugs can be impressive, but because they indiscriminately block the cell cycle of all actively dividing cells, their side effects severely constrain the dose and duration with which they can be administered, allowing both normal and malignant cells to escape complete growth arrest. Recent progress in understanding how cancers lose control of the cell cycle, coupled with comprehensive genomic profiling of human tumor biopsies, has shown that many cancers have mutations affecting various regulators and checkpoints that impinge on the core cell-cycle machinery. These defects introduce unique vulnerabilities that can be exploited by a next generation of drugs that promise improved therapeutic windows in patients whose tumors bear particular genomic aberrations, permitting increased dose intensity and efficacy. These developments, coupled with the success of new drugs targeting cell-cycle regulators, have led to a resurgence of interest in cellcycle inhibitors. This review in particular focuses on the newer strategies that may facilitate better therapeutic targeting of drugs that inhibit the various components that safeguard the fidelity of the fundamental processes of DNA replication and repair. Clin Cancer Res; 23(13); 1–9. 2017 AACR. Introduction defective. This shift in focus was vindicated by success of oncogene-targeting drugs such as trastuzumab, imatinib, erlotinib, vemurafenib, and crizotinib (1). During this same period, next-generation sequencing ushered in efforts to comprehensively catalog all genomic aberrations that can drive cancer growth (2). Interestingly, these studies identified key cell-cycle checkpoint genes that are commonly mutated in cancer. In particular, checkpoints at three stages are targeted by mutations in established cancer genes: (i) G1 phase checkpoints, including the restriction point; (ii) S-phase checkpoints, including DNA damage and origin firing checkpoints; and (iii) M-phase, particularly the spindle assembly checkpoint. Recent years have seen the introduction of inhibitors that specifically target kinases that facilitate DNA replication and repair such as inhibitors of ataxia telangiectasia mutated kinase (ATM), ataxia telangiectasia and Rad3-related kinase (ATR), WEE1, checkpoint kinase 1 (CHK1), and checkpoint kinase 2 (CHK2), collectively referred to herein as checkpoint kinase inhibitors. Because their mechanisms of action inhibit crucial components of DNA damage checkpoints, the initial interest in this class of inhibitors was their use in combination with standard cytotoxic (genotoxic) therapies as chemopotentiators. However, preclinical investigations led to a next-generation strategy that relies on the identification of underlying genetic or expression alterations that can potentially enhance the susceptibly of cancer cells to checkpoint kinase inhibitor monotherapy or to combination therapy with targeted drugs that do not induce generalized DNA damage. Consequently, this article reviews the underlying genetic drivers in tumors that facilitate better selective targeting of these agents, with a focus on checkpoint kinase inhibitors that are currently in development (Table 1). Tissue growth and homeostasis in multicellular organisms necessitate a variety of systems to regulate and coordinate cell division. When these systems fail, unabated and uncoordinated growth can lead to cancer. The core cell-cycle machinery required for chromosome duplication, chromosome segregation, and cytokinesis can be distinguished from cell-cycle regulators that restrain the core engine via cell-cycle checkpoints. Many traditional cancer therapies act on the core machinery, either at S-phase, preventing nucleotide synthesis and DNA replication (antimetabolites, DNA-damaging agents, and radiotherapy) or at mitosis (microtubule inhibitors). As they act on processes essential for all dividing cells, these classical therapies also affect normal proliferating tissues, and toxicities seemed inevitable for cell-cycle inhibitors. Hence, in the 1990s, cancer drug discovery shifted focus from cell-cycle targets to mitogenic and oncogenic signaling pathways. Targeting somatic mutations in genes encoding members of these signaling pathways offered a better therapeutic window in the cancers where they were 1 Early Phase Medical-Oncology, Eli Lilly and Company, Lilly Corporate Center, Indianapolis, Indiana. 2Oncology Business Unit-Patient Tailoring, Eli Lilly and Company, Lilly Corporate Center, Indianapolis, Indiana. 3Oncology Translational Research, Eli Lilly and Company, Lilly Corporate Center, Indianapolis, Indiana. Corresponding Author: Richard P. Beckmann, Eli Lilly and Company, Lilly Corporate Center, Drop Code 0438, Indianapolis, IN 46285. Phone: 317-2764285; Fax: 317-651-6346; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-16-0083 2017 American Association for Cancer Research. www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. OF1 Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Lin et al. Table 1. Cell-cycle kinase inhibitors currently in development Target Agent Phase Context WEE1 AZD1775, MK1775 II Monotherapy Chemotherapy combinations: cisplatin, carboplatin, docetaxel, gemcitabine, irinotecan, nab-paclitaxel, paclitaxel, peglyated liposomal doxorubicin, pemetrexed Targeted therapy combinations: olaparib, belinostat Radiation/chemoradiation combinations: monotherapy, cisplatin, gemcitabine, temozolomide Immunotherapy combinations: durvalumab CHK1 Prexasertib, LY2606368 II Monotherapy Chemotherapy combinations: cisplatin, 5-FU, pemetrexed Targeted therapy combinations: cetuximab, LY3023414 (PI3K/mTOR inhibitor), ralimetinib (p38 MAPK inhibitor), olaparib Chemoradiation combinations: cetuximab, cisplatin LY2880070, ESP-01 I CCT245737, PNT-737 I Monotherapy Chemotherapy combinations: gemcitabine Monotherapy Chemotherapy combinations: gemcitabine, cisplatin Monotherapy Chemotherapy combinations: gemcitabine Monotherapy Chemotherapy combinations: cisplatin, carboplatin, gemcitabine, etoposide, irinotecan, topotecan Targeted combinations: veliparib Chemoradiation combinations: monotherapy, cisplatin Monotherapy Chemotherapy combinations: carboplatin, paclitaxel Targeted combinations: olaparib Radiation Immunotherapy combinations: durvalumab GDC-0575, ARRY-575 I ATR ATM VX970 II AZD6738 I VX803 I AZD0156 I Monotherapy Chemotherapy combinations: gemcitabine, carboplatin, cisplatin Monotherapy Chemotherapy combinations: irinotecan, olaparib Populations being evaluated in all clinical contexts Cervical, CRC, gastric/GEJ, glioblastoma, gliomas, HNSCC, NSCLC, myeloid malignancies, ovarian, pancreatic, pediatric tumors, SCLC, squamous NSCLC, TNBC Biomarker focused: Basket trial: molecular profiling–based assignment Bladder: mutations in genes associated with cell-cycle regulation (RB1, CDKN2A, CCNE1 or MYC amp) CRC: KRAS/NRAS/BRAF mutations Gastric/GEJ: TP53 mutations NSCLC: biomarker-directed basket trial Ovarian: BRCA1 mutations, BRCA2 mutations, TP53 mutations, window trial Pediatric: basket trial stratifying based on molecular anomalies AML/high-risk MDS, CRC, HSNCC, NSCLC, ovarian, pediatric, prostate, SCC of anus, squamous NSCLC, SCLC, TNBC Biomarker focused: Basket trial: replication stress or homologous repair deficiency (e.g., MYC or CCNE1 amp, Rb loss, FBXW7 mutation, BRCA1, BRCA2, PALB2, RAD51C, RAD51D, ATR, ATM, CHK2, the Fanconi anemia pathway genes) Breast: BRCA1 mutations, BRCA2 mutations CRC: KRAS/BRAF mutations NSCLC: KRAS/BRAF mutations Ovarian: BRCA1 mutations, BRCA2 mutations CRC, ovarian, TNBC NSCLC, pancreatic HNSCC (HPV negative), NSCLC, ovarian, SCLC, urothelial, squamous NSCLC, TNBC B-cell malignancies, gastric/GEJ, HNSCC, NSCLC Biomarker focused: CLL: loss of chromosome 11q or ATM deficient Gastric/GEJ: low ATM expression HNSCC: window trial NSCLC: low ATM expression Ovarian NOTE: Source: www.clinicaltrials.gov. Abbreviations: AML, acute myeloid leukemia; amp, amplification; CLL, chronic lymphocytic leukemia; CRC, colorectal cancer; GEJ, gastroesophageal junction; HPV, human papillomavirus; HNSCC, squamous cell head and neck cancer; MDS, myelodysplastic syndrome; NSCLC, non–small cell lung cancer; SCC, squamous cell cancer; SCLC, small-cell lung cancer; TNBC, triple-negative breast cancer. ATM, ATR, WEE1, CHK1, and CHK2 are crucial components of DNA damage response (DDR) signaling networks responsible for contributing either to the detection and repair of damage or for coordinating DNA replication (3–6). These DDR checkpoint kinases function collectively to maintain genomic integrity by providing cells time to repair any DNA damage prior to replication or mitosis, and to initiate an apoptotic response if the damage is beyond repair. ATR and ATM act as sensors of single-strand and double-strand breaks (SSB and DSB), respectively, which activate CHK1 and CHK2 by phosphorylation (Fig. 1). CHK1 and CHK2 suppress cell-cycle progression through downregulation of the CDC25A and CDC25C phosphatases, which promote progression by removing inhibitory phosphates on CDK2 and CDK1, OF2 Clin Cancer Res; 23(13) July 1, 2017 respectively (7). WEE1 also prevents cell-cycle progression via inhibitory phosphorylation of CDK1 and CDK2 (8–11). The ATR–CHK1 response is also initiated in response to ssDNA generated by replication fork stalling (12, 13). Strategies for Clinical Development: Past and Present The initial preclinical studies evaluating these inhibitors clearly demonstrated that the chemical inhibition of checkpoint kinases enhances the activity of cytotoxic therapies that damage DNA through diverse mechanisms. Good reviews have been published recently describing this biology, and, therefore, it will not be Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Selective Targeting of Checkpoint Kinase Inhibitors Endogenous or exogenous events DSB SSB ATM ATR CHK2 CHK1 P P P P (Sequestration) (Proteolysis) WEE1 P WEE1 P CDC25A CDC25C P P P P CDK2 CDK2 CDK1 CDK1 Cyclin E Cyclin E Cyclin A/B Cyclin A/B P p53 p21 G1 S G2 M © 2017 American Association for Cancer Research Figure 1. ATR, ATM, CHK1, CHK2, and WEE1 inhibit cell-cycle progression into S-phase and mitosis following DNA damage. This regulation occurs ultimately through the control of the cyclin-dependent kinases (CDK) that facilitate entry into the S- and M-phases of the cell cycle, namely CDK2 and CDK1, respectively. The activity of CDK1 and CDK2 are controlled by phosphorylation as well as by the partnership of these kinases with their regulatory cyclin subunits, whereby activation of CDK2 requires association with cyclin E and CDK1 activation requires association with either cyclin A or B. Phosphorylation of either CDK1 or CDK2 is regulated in part by the opposing actions of the WEE1 kinase and the CDC25A/CDC25C phosphatases. ATR and ATM are sensors of SSBs and DSBs, respectively, which activate CHK1 and CHK2, respectively, by phosphorylation. The inhibition of cell-cycle progression by activated (phosphorylated) CHK1 and CHK2 results from the inhibition of CDK1 and CDK2, which is mediated by preventing the removal of inhibitory phosphates placed on CDK1 and CDK2, by WEE1. CHK1 and CHK2 prevent the removal of these phosphates by suppressing the CDC25A and CDC25C phosphatases through phosphorylation, whereby this phosphorylation facilitates proteolytic degradation of CDC25A and the sequestration of CDC25C by 14-3-3. p53 is activated upon DNA damage by phosphorylation by ATM and CHK2 and serves as an additional pathway to inhibit cell-cycle progression by promoting transcription of p21, which in turn inhibits the kinase activity of the cyclinE–CDK2 complex. summarized here (7, 10, 12–16). As a result of these data, clinical trials with early CHK1 inhibitors focused on the chemopotentiation of cytotoxic drugs. Although phase I trials demonstrated proof of concept that CHK1 inhibitors could be safely combined with chemotherapy (17–25), phase II studies failed to meet their primary endpoints (26, 27). Early CHK1 inhibitors were not successful for a variety of reasons, including pharmacokinetic properties, unacceptable toxicities, and business considerations. However, newer inhibitors, which are more diverse and include not only CHK1 inhibitors but also WEE1, ATR, and ATM inhibitors, continue to test this hypothesis with a variety of genotoxic agents and as monotherapies (Table 1). Although no phase II studies have been published with checkpoint inhibitors as monotherapy, evidence of efficacy has been observed in phase I. A phase I evaluation of AZD1775 as a monotherapy enrolled 24 patients, nine of whom had BRCA1 or BRCA2 mutations. Two patients with a BRCA1 mutation [squamous cell cancer (SCC) of the base of the www.aacrjournals.org tongue and papillary serous ovarian cancer] had partial responses (28). Prexasertib, a CHK1 inhibitor, demonstrated objective responses in patients with SCC of the anus and head and neck cancer in a phase I study with multiple expansion cohorts (29). These preliminary results suggest that the newer inhibitors may be more successful than initial CHK1 inhibitors, which were only developed as chemopotentiators. In addition, these data suggest the optimal use of these inhibitors may require the identification of contexts where tumorspecific vulnerabilities are leveraged to achieve selective cytotoxicity in cancer cells. p53 is a critical mediator of the DDR, which is activated through phosphorylation by CHK2 and ATM, and participates in a parallel pathway to ATR, CHK1, and WEE1 (Fig. 1; ref. 7). For this reason, cancer cells that have lost either p53 function or ATM may show greater reliance on ATR, CHK1, and WEE1 for efficient repair and, hence, greater sensitivity to treatments that inhibit these kinases (30–35). This hypothesis has Clin Cancer Res; 23(13) July 1, 2017 Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. OF3 Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Lin et al. been tested in a phase II trial where patients with TP53-mutated ovarian cancer who were refractory or resistant (<3 months) to first-line therapy received AZD1775 in combination with carboplatin. The combination demonstrated manageable toxicity, and in 21 evaluable patients, the objective response rate was 43%. Median progression-free and overall survival times were 5.3 months and 12.6 months, respectively. In addition to TP53 mutations, patients with an objective response had alterations in BRCA1, KRAS, MYC, or CCNE (cyclin E; ref. 36). Similarly, in a randomized, phase II trial in platinum-sensitive, TP53-mutant ovarian cancer, the WEE1 inhibitor AZD1775 combined with paclitaxel and carboplatin met the primary and secondary endpoints and significantly prolonged progression-free survival compared with the combination of paclitaxel and carboplatin (37). In a phase I, multi-arm combination study assessing AZD1775 with either gemcitabine, cisplatin, or carboplatin, 176 patients were evaluable for response. Responses were observed in patients with ovarian cancer (n ¼ 7), melanoma (n ¼ 3), breast cancer (n ¼ 2), head and neck cancer (n ¼ 3), colorectal cancer (n ¼ 1), and SCC of the skin (n ¼ 1). Patients with TP53 mutations (4/19, 23%) had a partial response compared with 4/33 (12%) of patients with TP53 wild-type tumors (38). Ongoing studies with AZD1775 continue to evaluate this hypothesis in TP53-mutated gastric cancer (with paclitaxel, NCT02448329), TP53- or KRAS-mutated solid tumors (with olaparib, NCT02576444), and TP53-mutated (with either MYC amplification or CDKN2A mutation) relapsed small-cell lung cancer (SCLC; monotherapy, NCT02688907). Similarly, the ATR inhibitor AZD6738 has an ongoing clinical study (NCT02264678) in ATM-low/deficient NSCLC (with carboplatin) or gastric cancer (with olaparib). These studies will further characterize the impact of TP53 mutations and ATM deficiency not only in the context of cytotoxic chemotherapy but also with targeted agents and monotherapy. The emerging clinical data with TP53 mutations are one example of potential synthetic lethality (SL), where functional alterations in one pathway lead to enhanced sensitivity to inhibition of another pathway. This is the strategy guiding the use of PARP inhibitors as therapies for BRCA1- or BRCA2-deficient breast or ovarian cancers (39–42). Leveraging SL for checkpoint kinase inhibitors requires knowledge about functional alterations in cancer cells that make them more vulnerable to the inhibition of these kinases than normal cells. Although TP53 mutations are the most well-characterized example of SL with the checkpoint inhibitors, the concept of replication stress (RS) is emerging as a potential SL mechanism (43, 44). RS can arise in any situation that leads to inappropriate replication origin licensing or firing (45). This results in stalled replication forks and DNA breaks if the stalled forks are not adequately resolved (46–48). In cancer cells, oncogene-driven events can contribute to higher degrees of RS by promoting growth to a point that strains the replicative capacity of the cell (45, 49). As a result, inhibitors of checkpoint kinases may induce SL with tumors that have high RS, as all of these kinases contribute to sensing and reducing RS (Fig. 2). In particular, WEE1 and CHK1 play complementary roles in restricting the initiation of replication origins by inhibiting CDK2, which when activated, promotes replication (6, 50, 51). Thus, treatment with an inhibitor of CHK1 or WEE1 augments ongoing RS by effectively neutralizing one of the mechanisms available for suppressing replication origin firing, resulting in more stalling and DNA breaks. As both CHK1 and WEE1 are important OF4 Clin Cancer Res; 23(13) July 1, 2017 signaling components in the response to DNA damage, damage that results from the additional RS is potentially exacerbated because it cannot be repaired effectively. Likewise, ATR plays an important role as a sensor for RS as it is recruited to regions of ssDNA that become exposed by replication fork stalling. Subsequently, ATR is responsible for activating CHK1, which in turn suppresses replication, as indicated above (15). An ongoing challenge is to identify tumors that have reached near-critical levels of RS and are likely the most susceptible to treatment with checkpoint kinase inhibitors. Validation of therapeutic strategies to exploit RS has recently emerged from several studies (52–63). For example, an SL relationship was described between oncogene-induced RS by MYC activation and ATR loss in lymphomas (49). Specifically in the context of ATR-deficient cells, MYC expression induced higher RS and apoptosis and contributed to greater sensitivity to ATR and CHK1 inhibitors. Analogous observations were derived from studies in neuroblastoma models wherein sensitivity to CHK1 inhibition was correlated with MYCN expression (52). Studies in other model systems for hematologic malignancies such as MYCdriven diffuse large B-cell lymphoma, cyclin D1–driven mantle cell lymphomas, T-cell acute lymphoblastic leukemia, and acute myeloid leukemia suggest that oncogene-induced RS in these cancers may make them particularly vulnerable to treatment with checkpoint kinase inhibitors (53–55, 58, 61, 63). The hypothesis that MYC may drive RS and increase sensitivity to checkpoint kinase inhibitors is being tested in several ongoing clinical trials, including a biomarker-directed study with AZD1775 and durvalumab in muscle-invasive bladder cancer. To be eligible, patients must have mutations in CDKN2A or RB1 genes and/or amplification of CCNE1, MYC, MYCL, or MYCN genes, all of which presumably contribute to heightened RS (Fig. 2). Other agents are focusing on SCLC, a tumor associated with RS and MYC amplifications: AZD1775 (NCT02593019) and prexasertib (NCT02735980) are being assessed as monotherapy, whereas VX970 is being evaluated with topotecan (NCT02487095). Another opportunity for SL may be inhibition of ATR in the context of ATM deficiency. In preclinical models of hematologic malignancies, cells that lack ATM (e.g., due to 11q deletions) or have defects in p53 signaling were particularly vulnerable to the ATR inhibitor AZD6738. Treatment with AZD6738 increased replication initiation and fork stalling, resulting in RS and DNA damage that likely contributed to selective cytotoxicity in cells with p53 and/or ATM defects (64). In parallel, in a phase I trial with the ATR inhibitor VX970 and carboplatin, a patient with colorectal cancer and ATM loss achieved a complete response (65). This hypothesis is being further tested in a trial of AZD6738 in patients with relapsed/refractory B-cell malignancies with prospectively identified 11q-deleted or ATM-deficient relapsed/ refractory CLL (NCT01955668). In addition to neuroblastomas, as mentioned above, other pediatric cancers, particularly sarcomas, may represent another opportunity for exploiting oncogenic drivers of RS, as demonstrated by recent studies in models for Ewing sarcoma (ES) wherein the oncogenic drivers were fusion proteins unique to this tumor (EWS/FLI1 or EWS/ERG; ref. 59). In these studies, ES cell lines were more sensitive to inhibition of ATR compared with sarcoma cell lines that lacked the EWS fusions, and ATR inhibitor monotherapy resulted in near-complete to complete growth inhibition of human ES xenografts. Related studies with the CHK1 inhibitor prexasertib (56) showed that monotherapy resulted in Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Selective Targeting of Checkpoint Kinase Inhibitors Cyclin E P P P CDK2 CDC25A CHK1 WEE1 Cyclin E CDK2 RPA RPA TopBP1 ATRIP DNA lesion ATR RPA “Activation” P RPA Replication stress • Oncogenes • Enhanced cyclin E or CDK2 expression/activity • Loss of regulation of G1 → S progression • Loss of function of ATR, CHK1, or WEE1 Fork collapse → DSBs Homologous recombination repair © 2017 American Association for Cancer Research Figure 2. The ATR–CHK1 pathway reduces RS. The kinase function of CDK2 requires activation by association with cyclin E. When activated by cyclin E, CDK2 facilitates the progression of cells from G1 into S-phase and subsequently promotes replication origin firing. ATR and CHK1 suppress replication origin firing in part by suppressing the activity of CDK2 through regulation of downstream effectors that coordinate the phosphorylation of CDK2. Specifically, the presence of long stretches of single-stranded DNA, which can occur in situations where the DNA polymerases lag behind the unwinding activity of the helicases, trigger ATR, which is recruited by a complex of proteins including replication protein A (RPA), topoisomerase-binding protein 1 (TopBP1), and ATR-interacting protein (ATRIP). ATR then activates CHK1 (through phosphorylation), which subsequently through phosphorylation of the CDC25A phosphatase, negatively regulates CDK2 by preventing the removal of inhibitory phosphates by this phosphatase. The actions of CDC25A are also opposed by WEE1, which contributes to the inhibition of CDK2 by catalyzing the inhibitory phosphates that are removed by CDC25A. As shown at the bottom half of the figure, RS can result from endogenous or exogenous DNA damage as well as through the action of growth-promoting oncogenes, such as MYC, which serve to drive progression into S-phase. In addition, RS can also arise through other alterations that disrupt control at the G1–S interface, such as changes that lead to enhanced expression of cyclin E or loss of inhibition of CDK2. Alterations that may enhance cyclin E expression or CDK2 activity possibly include (i) losses in FBXW7, which facilitates proteasomal degradation of cyclin E or (ii) alterations that disrupt regulation of the primary restriction point controlling progression from G1 into S including activation of CDK4, CDK6, and D-type cyclins or loss of RB1 that serves to activate E2F, thereby promoting the transcription of the genes that encode cyclin E and CDK2 as well as other gene products that promote DNA replication. Notably, as indicated by the red Xs, the inhibition or loss of function of ATR, CHK1, or WEE1 can elevate ongoing RS by effectively removing the control over CDK2. The result of this inhibition or loss is replication fork collapse, with eventual DNA DSBs leading to the activation of DNA damage and repair responses such as homologous recombination repair. complete regressions in xenograft models for desmoplastic small round cell tumor, which also expresses an oncogenic EWS fusion protein known as EWS–WT1, or alveolar rhabdomyosarcoma, a malignancy driven by another unique oncogenic fusion protein (66, 67). These nonclinical studies with prexasertib have led to an interest in exploring prexasertib in pediatric solid tumors (NCT02808650). In addition, WEE1 was identified as a target in medulloblastoma, the most common pediatric malignant brain tumor (68). AZD1775 induced DNA damage and suppressed the growth of medulloblastoma cells both in vitro and in vivo (68), potentially by exploiting MYC-induced RS (69). AZD1775 has also demonstrated in vitro activity in rhabdomyosarcoma as monotherapy and in combination with conventional therapies (70) and improved the efficacy of radiation in mouse models of www.aacrjournals.org pediatric high-grade glioma (71). A phase I study of AZD1775 and radiation in children with diffuse intrinsic pontine gliomas is ongoing (NCT01922076). AZD1775 is also being assessed in the European Proof-of-Concept Therapeutic Stratification Trial of Molecular Anomalies in Relapsed or Refractory Tumors (ESMART). In this basket study, molecular profiling of pediatric tumors is used to direct patients to individual treatment arms, including a combination of AZD1775 and carboplatin (NCT02813135). Strategies exploiting RS also include combining inhibitors targeting different checkpoint kinases. Accordingly, RNA interference (RNAi) studies exploring SL with the CHK1 inhibitor PF-00477736 identified WEE1 as the most significant hit (72). In addition, synergistic growth inhibition was observed with Clin Cancer Res; 23(13) July 1, 2017 Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. OF5 Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Lin et al. PF-00477736 and AZD1775 in cell lines and in a xenograft model for ovarian cancer (72). Synergy was also observed with AZD1775 and the CHK1 inhibitor MK-8776 (73). Analogous studies showed that treatment of cancer cells in culture with the CHK1 inhibitor AZD7762 and the ATR inhibitor VE-821 elevated RS, leading to replication catastrophe and death by apoptosis. The combination was associated with a significant inhibition of tumor growth and an increase in overall survival in mice bearing human NCI-H460 NSCLC xenografts when compared with the monotherapy treatments (74). In addition to RS, deficiencies in homologous recombination repair (HRR) may also contribute to greater sensitivity to checkpoint kinase inhibition, as homologous recombination deficiencies (HRD) reduce the efficiency of repair of DSBs that result from RS generated by these inhibitors (Fig. 2). Deficiencies in the Fanconi anemia (FA) genes (FANC), such as defects in BRCA1 or BRCA2, also disrupt HRR (75), and studies with the CHK1 inhibitor G€ o6976 showed that FA-deficient cell lines were highly sensitive to G€ o6976 and to RNAi silencing of CHK1 mRNA expression when compared with isogenic lines that were FA proficient (76). An RNAi-based screen that targeted 230 DNA repair genes identified many FANC genes as SL with G€ o6976 treatment, including FANCA, FANCC, FANCD1, FANCD2, FANCE, FANCF, and FANCG. A similar approach using siRNA to target 240 DNA replication and repair genes explored SL with ATR inhibitors (57). These studies uncovered that loss of expression of ATR pathway genes had the strongest association for SL including losses of ATR itself, ATRIP, RPA, and CHK1. As the ATR pathway is crucial for responding to RS, the observations from this study as well as others provide support regarding the therapeutic benefits that may be derived from the combined inhibition of targets within this pathway to elevate RS further (62, 72–74). In addition, the results confirm the benefit that may be attained through monotherapy by selective targeting of tumors with preexisting mutations in this pathway. Of note, these studies demonstrated that loss of excision repair cross-complementation group 1 protein (ERCC1), which functions in the repair of bulky DNA adducts, DSBs, and interstrand cross-links (77), was a significant SL interaction with ATR and CHK1 inhibition. Similar SL interactions were observed between ATR inhibition and loss of another repair gene known as XRCC1, which plays a role base excision repair (78) and with ATM deficiency (34). These studies suggest that therapeutic strategies aimed at disrupting HRR may facilitate SL with checkpoint kinase inhibitors. In this regard, CHK1, in addition to its role in limiting RS, is required for HRR by facilitating the essential recruitment of RAD51 to sites of repair (79). Thus, CHK1 inhibition would be expected to promote further deficiencies in HRR in addition to exacerbating RS. In support of this concept, augmented growth inhibition by the PARP inhibitor olaparib was observed upon the RNAi silencing of genes encoding CHK1, CHK2, ATR, ATM, and RPA1 as well as genes encoding proteins that contribute to HRR such as RAD51, NBS1, FANCA, FANCD2, and FANCC (40). In addition, studies in breast carcinoma cell lines showed that the combination of PARP inhibitors (olaparib, veliparib, NU1025, or rucaparib) with CHK1 inhibitors (UCN-01, AZD7762, or LY2603618) increased DNA damage and cytotoxicity, as compared with the single-agent treatments (80). More recent studies have shown in BRCA1- or BRCA2-mutated high-grade serous ovarian cancer (HGSOC) models that combination therapy with OF6 Clin Cancer Res; 23(13) July 1, 2017 olaparib and either MK-8776 (CHK1) or AZD6738 (ATR) acted synergistically to decrease survival and colony formation in vitro and inhibit tumor xenograft growth in vivo (81). Clinical trials evaluating PARP inhibition with AZD1775 (NCT02511795), AZD0156 (NCT02588105), VX970 (NCT02723864), or AZD6738 (NCT02264678) are ongoing. In addition, a study with AZD1775 and olaparib (OLAPCO) is a molecularly directed trial that requires mutations in TP53 or KRAS (NCT02576444). As outlined above, the optimal context for a checkpoint kinase inhibitor might be tumors that have both high RS and HRD. Of notable interest are ovarian cancers, particularly HGSOCs, as approximately half harbor mutations in genes that modulate HRR, including mutations that impact BRCA1 and BRCA2 (39, 82). In addition, nearly all HGSOCs have mutations in TP53 (83). Mutations in ATM and ATR have been observed in 2% of HGSOCs, and 5% have mutations in genes of the FA DNA repair pathway (39). Mutually exclusive with mutations in BRCA1 and BRCA2, CCNE1 is amplified in 15% to 20% of HGSOCs (82, 84). RB1 loss is also observed in about 15% of these cancers (83). As cyclin E is required for activation of CDK2, its overexpression induces RS and DNA damage that activates HRR and may increase sensitivity to single-agent CHK1, ATR1, and/or WEE1 inhibition (85). Likewise loss of RB1 can contribute to RS by promoting the progression of cells into S-phase. Therefore, HGSOCs present a provocative context for therapy with the checkpoint kinase inhibitors by providing an opportunity to leverage the dual presence of higher RS and HRD (28, 86). Accordingly, AZD1775, prexasertib, LY2880070, VX970, VX803, and AZD0156 are being assessed in a variety of subsets of ovarian cancer (Table 1), and it may be notable that AZD1775 has demonstrated clinical activity in both platinum-sensitive and platinum-resistant ovarian cancer (36, 37). As our understanding of SL interactions and the underlying mechanisms of the checkpoint kinase inhibitors grows, the optimal context may shift from a focus on a particular histology such as ovarian cancer, to the genetic attributes of the tumor regardless of histology. This approach is already being implemented in multiple clinical trials. In a prexasertib basket trial (NCT02873975), patients whose tumors show alterations consistent with RS (MYC amplification, CCNE1 amplification, Rb loss, or FBXW7 mutation) or HRD (BRCA1, BRCA2, PALB2, RAD51C, RAD51D, ATR, ATM, CHK2, or the FA pathway genes) are eligible. Similarly, AZD1775 is being assessed in the Molecular Profiling–Based Targeted Therapy (MPACT) trial, which assigns patients with solid tumors to a treatment regimen based on their mutation/amplification category. One of these arms assesses AZD1775 in combination with carboplatin (NCT01827384). One obvious goal from these types of studies, besides improved efficacy, is to identify tumor-specific biomarkers that can be used to predict response to monotherapy or combination therapy with one or more checkpoint kinase inhibitors. Preclinical studies indicate that alterations inducing RS or HRD contribute to greater sensitivity to these inhibitors. However, the crucial challenge from a clinical perspective is going beyond just identifying which of these alterations indicate the presence of RS or HRD to identifying situations where tumors are at near-unstainable levels of RS or HRD and, therefore, are most susceptible to interventions that further augment RS or compromise HRR. The identification of expression or genetic alterations in a small subset of stand-alone biomarkers for predicting response is Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Selective Targeting of Checkpoint Kinase Inhibitors certainly desirable and may be achievable in certain cancers, but for other cancers, additional methodologies may be required to adequately measure the extent to which RS and HRD are near catastrophic. However, these challenges should not dampen our enthusiasm for the ongoing clinical trials with the various checkpoint kinase inhibitors, as some of these trials may provide patient data that will allow us to validate and refine our biomarker hypotheses. The preclinical studies have provided a solid foundation leading to the concept of leveraging RS and HRD to achieve SL in human tumors. The clinical data will allow us to return to the bench to explore additional concepts that will further enhance the therapeutic benefit of the checkpoint kinase inhibitors. Disclosure of Potential Conflicts of Interest A.B. Lin, S.C. McNeely, and R.P. Beckmann hold ownership interest in Eli Lilly and Company. No other potential conflicts of interest were disclosed. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Received October 17, 2016; revised November 29, 2016; accepted March 15, 2017; published OnlineFirst March 22, 2017. References 1. Chin L, Andersen JN, Futreal PA. Cancer genomics: from discovery science to personalized medicine. Nat Med 2011;17:297–303. 2. Stratton MR, Campbell PJ, Futreal PA. The cancer genome. Nature 2009;458:719–24. 3. Ciccia A, Elledge SJ. The DNA damage response: making it safe to play with knives. Mol Cell 2010;40:179–204. 4. Harper JW, Elledge SJ. The DNA damage response: ten years after. Mol Cell 2007;28:739–45. 5. Sorensen CS, Syljuasen RG. Safeguarding genome integrity: the checkpoint kinases ATR, CHK1 and WEE1 restrain CDK activity during normal DNA replication. Nucleic Acids Res 2012;40:477–86. 6. Jones RM, Petermann E. Replication fork dynamics and the DNA damage response. Biochem J 2012;443:13–26. 7. McNeely S, Beckmann R, Bence Lin AK. CHEK again: revisiting the development of CHK1 inhibitors for cancer therapy. Pharmacol Ther 2014; 142:1–10. 8. Parker LL, Piwnica-Worms H. Inactivation of the p34cdc2-cyclin B complex by the human WEE1 tyrosine kinase. Science 1992;257:1955–7. 9. Watanabe N, Broome M, Hunter T. Regulation of the human WEE1Hu CDK tyrosine 15-kinase during the cell cycle. EMBO J 1995;14:1878–91. 10. Do K, Doroshow JH, Kummar S. Wee1 kinase as a target for cancer therapy. Cell Cycle 2013;12:3159–64. 11. Matheson CJ, Backos DS, Reigan P. Targeting WEE1 kinase in cancer. Trends Pharmacol Sci 2016;37:872–81. 12. Fokas E, Prevo R, Hammond EM, Brunner TB, McKenna WG, Muschel RJ. Targeting ATR in DNA damage response and cancer therapeutics. Cancer Treat Rev 2014;40:109–17. 13. Weber AM, Ryan AJ. ATM and ATR as therapeutic targets in cancer. Pharmacol Ther 2015;149:124–38. 14. Ma CX, Janetka JW, Piwnica-Worms H. Death by releasing the breaks: CHK1 inhibitors as cancer therapeutics. Trends Mol Med 2011;17:88–96. 15. Toledo LI, Murga M, Fernandez-Capetillo O. Targeting ATR and Chk1 kinases for cancer treatment: a new model for new (and old) drugs. Mol Oncol 2011;5:368–73. 16. Thompson R, Eastman A. The cancer therapeutic potential of Chk1 inhibitors: how mechanistic studies impact on clinical trial design. Br J Clin Pharmacol 2013;76:358–69. 17. Calvo E, Braiteh F, Von Hoff D, McWilliams R, Becerra C, Galsky MD, et al. Phase I study of CHK1 inhibitor LY2603618 in combination with gemcitabine in patients with solid tumors. Oncology 2016;91:251–60. 18. Calvo E, Chen VJ, Marshall M, Ohnmacht U, Hynes SM, Kumm E, et al. Preclinical analyses and phase I evaluation of LY2603618 administered in combination with pemetrexed and cisplatin in patients with advanced cancer. Invest New Drugs 2014;32:955–68. 19. Daud AI, Ashworth MT, Strosberg J, Goldman JW, Mendelson D, Springett G, et al. Phase I dose-escalation trial of checkpoint kinase 1 inhibitor MK8776 as monotherapy and in combination with gemcitabine in patients with advanced solid tumors. J Clin Oncol 2015;33:1060–6. 20. Doi T, Yoshino T, Shitara K, Matsubara N, Fuse N, Naito Y, et al. Phase I study of LY2603618, a CHK1 inhibitor, in combination with gemcitabine in Japanese patients with solid tumors. Anticancer Drugs 2015;26: 1043–53. www.aacrjournals.org 21. Infante JR, Hollebecque A, Postel-Vinay S, Bauer TM, Blackwood E, Evangelista M, et al. Phase I study of GDC-0425, a checkpoint kinase 1 inhibitor, in combination with gemcitabine in patients with refractory solid tumors [abstract]. In: Proceedings of the 106th Annual Meeting of the American Association for Cancer Research; 2015 Apr 18–22; Philadelphia, PA. Philadelphia (PA): AACR; 2015. Abstract nr CT139. 22. Karp JE, Thomas BM, Greer JM, Sorge C, Gore SD, Pratz KW, et al. Phase I and pharmacologic trial of cytosine arabinoside with the selective checkpoint 1 inhibitor Sch 900776 in refractory acute leukemias. Clin Cancer Res 2012;18:6723–31. 23. Sausville E, Lorusso P, Carducci M, Carter J, Quinn MF, Malburg L, et al. Phase I dose-escalation study of AZD7762, a checkpoint kinase inhibitor, in combination with gemcitabine in US patients with advanced solid tumors. Cancer Chemother Pharmacol 2014;73:539–49. 24. Seto T, Esaki T, Hirai F, Arita S, Nosaki K, Makiyama A, et al. Phase I, doseescalation study of AZD7762 alone and in combination with gemcitabine in Japanese patients with advanced solid tumours. Cancer Chemother Pharmacol 2013;72:619–27. 25. Weiss GJ, Donehower RC, Iyengar T, Ramanathan RK, Lewandowski K, Westin E, et al. Phase I dose-escalation study to examine the safety and tolerability of LY2603618, a checkpoint 1 kinase inhibitor, administered 1 day after pemetrexed 500 mg/m(2) every 21 days in patients with cancer. Invest New Drugs 2013;31:136–44. 26. Scagliotti G, Kang JH, Smith D, Rosenberg R, Park K, Kim SW, et al. Phase II evaluation of LY2603618, a first-generation CHK1 inhibitor, in combination with pemetrexed in patients with advanced or metastatic non-small cell lung cancer. Invest New Drugs 2016;34:625–35. 27. Webster JA, Tibes R, Blackford A, Morris L, Patnaik MM, Wang L, et al. Randomized phase II trial of timed sequential cytosine arabinoside with and without the CHK1 inhibitor MK-8876 in adults with relapsed and refractory acute myelogenous leukemia. Blood 2015;126:2563. 28. Do K, Wilsker D, Ji J, Zlott J, Freshwater T, Kinders RJ, et al. Phase I study of single-agent AZD1775 (MK-1775), a Wee1 kinase inhibitor, in patients with refractory solid tumors. J Clin Oncol 2015;33:3409–15. 29. Hong D, Infante J, Janku F, Jones S, Nguyen LM, Burris H, et al. Phase I study of LY2606368, a checkpoint kinase 1 inhibitor, in patients with advanced cancer. J Clin Oncol 2016;34:1764–71. 30. Zabludoff SD, Deng C, Grondine MR, Sheehy AM, Ashwell S, Caleb BL, et al. AZD7762, a novel checkpoint kinase inhibitor, drives checkpoint abrogation and potentiates DNA-targeted therapies. Mol Cancer Ther 2008;7:2955–66. 31. Hirai H, Iwasawa Y, Okada M, Arai T, Nishibata T, Kobayashi M, et al. Small-molecule inhibition of Wee1 kinase by MK-1775 selectively sensitizes p53-deficient tumor cells to DNA-damaging agents. Mol Cancer Ther 2009;8:2992–3000. 32. King C, Diaz H, Barnard D, Barda D, Clawson D, Blosser W, et al. Characterization and preclinical development of LY2603618: a selective and potent Chk1 inhibitor. Invest New Drugs 2014;32:213–26. 33. Rajeshkumar NV, De Oliveira E, Ottenhof N, Watters J, Brooks D, Demuth T, et al. MK-1775, a potent Wee1 inhibitor, synergizes with gemcitabine to achieve tumor regressions, selectively in p53-deficient pancreatic cancer xenografts. Clin Cancer Res 2011;17:2799–806. Clin Cancer Res; 23(13) July 1, 2017 Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. OF7 Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Lin et al. 34. Reaper PM, Griffiths MR, Long JM, Charrier JD, Maccormick S, Charlton PA, et al. Selective killing of ATM- or p53-deficient cancer cells through inhibition of ATR. Nat Chem Biol 2011;7:428–30. 35. Toledo LI, Murga M, Zur R, Soria R, Rodriguez A, Martinez S, et al. A cell-based screen identifies ATR inhibitors with synthetic lethal properties for cancer-associated mutations. Nat Struct Mol Biol 2011;18: 721–7. 36. Leijen S, van Geel RM, Sonke GS, de Jong D, Rosenberg EH, Marchetti S, et al. Phase II study of WEE1 inhibitor AZD1775 plus carboplatin in patients with TP53-mutated ovarian cancer refractory or resistant to first-line therapy within 3 months. J Clin Oncol 2016;34:4354–61. 37. Oza AM, Weberpals JI, Provencher DM, Grischke E-M, Hall M, Uyar D, et al. An international, biomarker-directed, randomized, phase II trial of AZD1775 plus paclitaxel and carboplatin (P/C) for the treatment of women with platinum-sensitive, TP53-mutant ovarian cancer. J Clin Oncol 33, 2015 (suppl; abstr 5506). 38. Leijen S, van Geel RM, Pavlick AC, Tibes R, Rosen L, Razak AR, et al. Phase I study evaluating WEE1 inhibitor AZD1775 as monotherapy and in combination with gemcitabine, cisplatin, or carboplatin in patients with advanced solid tumors. J Clin Oncol 2016;34:4371–80. 39. Lord CJ, Ashworth A. BRCAness revisited. Nat Rev Cancer 2016;16: 110–20. 40. McCabe N, Turner NC, Lord CJ, Kluzek K, Bialkowska A, Swift S, et al. Deficiency in the repair of DNA damage by homologous recombination and sensitivity to poly(ADP-ribose) polymerase inhibition. Cancer Res 2006;66:8109–15. 41. Bryant HE, Schultz N, Thomas HD, Parker KM, Flower D, Lopez E, et al. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADPribose) polymerase. Nature 2005;434:913–7. 42. Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 2005;434:917–21. 43. Dobbelstein M, Sorensen CS. Exploiting replicative stress to treat cancer. Nat Rev Drug Discov 2015;14:405–23. 44. Lecona E, Fernandez-Capetillo O. Replication stress and cancer: it takes two to tango. Exp Cell Res 2014;329:26–34. 45. Hills SA, Diffley JF. DNA replication and oncogene-induced replicative stress. Curr Biol 2014;24:R435–44. 46. Gaillard H, Garcia-Muse T, Aguilera A. Replication stress and cancer. Nat Rev Cancer 2015;15:276–89. 47. Zeman MK, Cimprich KA. Causes and consequences of replication stress. Nat Cell Biol 2014;16:2–9. 48. Mazouzi A, Velimezi G, Loizou JI. DNA replication stress: causes, resolution and disease. Exp Cell Res 2014;329:85–93. 49. Murga M, Campaner S, Lopez-Contreras AJ, Toledo LI, Soria R, Montana MF, et al. Exploiting oncogene-induced replicative stress for the selective killing of Myc-driven tumors. Nat Struct Mol Biol 2011;18:1331–5. 50. Maya-Mendoza A, Petermann E, Gillespie DA, Caldecott KW, Jackson DA. Chk1 regulates the density of active replication origins during the vertebrate S phase. EMBO J 2007;26:2719–31. 51. Petermann E, Woodcock M, Helleday T. Chk1 promotes replication fork progression by controlling replication initiation. Proc Natl Acad Sci U S A 2010;107:16090–5. 52. Cole KA, Huggins J, Laquaglia M, Hulderman CE, Russell MR, Bosse K, et al. RNAi screen of the protein kinome identifies checkpoint kinase 1 (CHK1) as a therapeutic target in neuroblastoma. Proc Natl Acad Sci U S A 2011;108:3336–41. 53. David L, Fernandez-Vidal A, Bertoli S, Grgurevic S, Lepage B, Deshaies D, et al. CHK1 as a therapeutic target to bypass chemoresistance in AML. Sci Signal 2016;9:ra90. 54. Derenzini E, Agostinelli C, Imbrogno E, Iacobucci I, Casadei B, Brighenti E, et al. Constitutive activation of the DNA damage response pathway as a novel therapeutic target in diffuse large B-cell lymphoma. Oncotarget 2015;6:6553–69. 55. Ghelli Luserna Di Rora A, Iacobucci I, Imbrogno E, Papayannidis C, Derenzini E, Ferrari A, et al. Prexasertib, a Chk1/Chk2 inhibitor, increases the effectiveness of conventional therapy in B-/T- cell progenitor acute lymphoblastic leukemia. Oncotarget 2016;7:53377–91. 56. May C, Beckmann R, Blosser W, Dowless M, VanWye A, Burke T, et al. Targeting checkpoint kinase 1 (CHK1) with the small molecule inhibitor LY2606368 mesylate monohydrate in models of high-risk pediatric cancer OF8 Clin Cancer Res; 23(13) July 1, 2017 57. 58. 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. 74. 75. 76. 77. yields significant antitumor effects [abstract]. In: Proceedings of the 107th Annual Meeting of the American Association for Cancer Research; 2016 Apr 16-20; New Orleans, LA. Philadelphia (PA): AACR; Cancer Res 2016;76(14 Suppl):Abstract nr 2458. Mohni KN, Kavanaugh GM, Cortez D. ATR pathway inhibition is synthetically lethal in cancer cells with ERCC1 deficiency. Cancer Res 2014;74: 2835–45. Morgado-Palacin I, Day A, Murga M, Lafarga V, Anton ME, Tubbs A, et al. Targeting the kinase activities of ATR and ATM exhibits antitumoral activity in mouse models of MLL-rearranged AML. Sci Signal 2016;9:ra91. Nieto-Soler M, Morgado-Palacin I, Lafarga V, Lecona E, Murga M, Callen E, et al. Efficacy of ATR inhibitors as single agents in Ewing sarcoma. Oncotarget 2016;7:58759–67. Pfister SX, Markkanen E, Jiang Y, Sarkar S, Woodcock M, Orlando G, et al. Inhibiting WEE1 selectively kills histone H3K36me3-deficient cancers by dNTP starvation. Cancer Cell 2015;28:557–68. Restelli V, Chila R, Lupi M, Rinaldi A, Kwee I, Bertoni F, et al. Characterization of a mantle cell lymphoma cell line resistant to the Chk1 inhibitor PF-00477736. Oncotarget 2015;6:37229–40. Saini P, Li Y, Dobbelstein M. Wee1 is required to sustain ATR/Chk1 signaling upon replicative stress. Oncotarget 2015;6:13072–87. Sarmento LM, Povoa V, Nascimento R, Real G, Antunes I, Martins LR, et al. CHK1 overexpression in T-cell acute lymphoblastic leukemia is essential for proliferation and survival by preventing excessive replication stress. Oncogene 2015;34:2978–90. Kwok M, Davies N, Agathanggelou A, Smith E, Oldreive C, Petermann E, et al. ATR inhibition induces synthetic lethality and overcomes chemoresistance in TP53- or ATM-defective chronic lymphocytic leukemia cells. Blood 2016;127:582–95. Yap TA, Luken MJdM, O'Carrigan B, Roda D, Papadatos-Pastos D, Lorente D, et al. Phase I trial of first-in-class ataxia telangiectasia-mutated and Rad3related (ATR) inhibitor VX-970 as monotherapy (mono) or in combination with carboplatin (CP) in advanced cancer patients (pts) with preliminary evidence of target modulation and antitumor activity. Mol Cancer Ther 2015;14(12 Suppl 2):PR14. Gerald WL, Haber DA. The EWS-WT1 gene fusion in desmoplastic small round cell tumor. Semin Cancer Biol 2005;15:197–205. Shern JF, Chen L, Chmielecki J, Wei JS, Patidar R, Rosenberg M, et al. Comprehensive genomic analysis of rhabdomyosarcoma reveals a landscape of alterations affecting a common genetic axis in fusion-positive and fusion-negative tumors. Cancer Discov 2014;4:216–31. Harris PS, Venkataraman S, Alimova I, Birks DK, Balakrishnan I, Cristiano B, et al. Integrated genomic analysis identifies the mitotic checkpoint kinase WEE1 as a novel therapeutic target in medulloblastoma. Mol Cancer 2014;13:72. Moreira D, Venkataraman S, Balakrishnan I, Prince E, Foreman N, Vibhakar R. MB-71 The role of wee1 in Myc-driven medulloblastoma. Neuro Oncol 2016;18(suppl_3):iii113. Kahen E, Yu D, Harrison DJ, Clark J, Hingorani P, Cubitt CL, et al. Identification of clinically achievable combination therapies in childhood rhabdomyosarcoma. Cancer Chemother Pharmacol 2016;78:313–23. Mueller S, Hashizume R, Yang X, Kolkowitz I, Olow AK, Phillips J, et al. Targeting Wee1 for the treatment of pediatric high-grade gliomas. Neuro Oncol 2014;16:352–60. Carrassa L, Chila R, Lupi M, Ricci F, Celenza C, Mazzoletti M, et al. Combined inhibition of Chk1 and Wee1: in vitro synergistic effect translates to tumor growth inhibition invivo. Cell Cycle 2012;11:2507–17. Guertin AD, Martin MM, Roberts B, Hurd M, Qu X, Miselis NR, et al. Unique functions of CHK1 and WEE1 underlie synergistic anti-tumor activity upon pharmacologic inhibition. Cancer Cell Int 2012;12:45. Sanjiv K, Hagenkort A, Calderon-Montano JM, Koolmeister T, Reaper PM, Mortusewicz O, et al. Cancer-specific synthetic lethality between ATR and CHK1 kinase activities. Cell Rep 2016;14:298–309. Kennedy RD, D'Andrea AD. The Fanconi Anemia/BRCA pathway: new faces in the crowd. Genes Dev 2005;19:2925–40. Chen CC, Kennedy RD, Sidi S, Look AT, D'Andrea A. CHK1 inhibition as a strategy for targeting Fanconi Anemia (FA) DNA repair pathway deficient tumors. Mol Cancer 2009;8:24. Olaussen KA, Dunant A, Fouret P, Brambilla E, Andre F, Haddad V, et al. DNA repair by ERCC1 in non-small-cell lung cancer and cisplatin-based adjuvant chemotherapy. N Engl J Med 2006;355:983–91. Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Selective Targeting of Checkpoint Kinase Inhibitors 78. Sultana R, Abdel-Fatah T, Perry C, Moseley P, Albarakti N, Mohan V, et al. Ataxia telangiectasia mutated and Rad3 related (ATR) protein kinase inhibition is synthetically lethal in XRCC1 deficient ovarian cancer cells. PLoS One 2013;8:e57098. 79. Sorensen CS, Hansen LT, Dziegielewski J, Syljuasen RG, Lundin C, Bartek J, et al. The cell-cycle checkpoint kinase Chk1 is required for mammalian homologous recombination repair. Nat Cell Biol 2005;7:195–201. 80. Booth L, Cruickshanks N, Ridder T, Dai Y, Grant S, Dent P. PARP and CHK inhibitors interact to cause DNA damage and cell death in mammary carcinoma cells. Cancer Biol Ther 2013;14:458–65. 81. Kim H, George E, Ragland RL, Rafail S, Zhang R, Krepler C, et al. Targeting the ATR/CHK1 axis with PARP inhibition results in tumor regression in BRCA mutant ovarian cancer models. Clin Cancer Res 2016 Dec 19. [Epub ahead of print]. 82. Konstantinopoulos PA, Ceccaldi R, Shapiro GI, D'Andrea AD. Homologous recombination deficiency: exploiting the fundamental vulnerability of ovarian cancer. Cancer Discov 2015;5:1137–54. www.aacrjournals.org 83. Bowtell DD, Bohm S, Ahmed AA, Aspuria PJ, Bast RCJr, Beral V, et al. Rethinking ovarian cancer II: reducing mortality from high-grade serous ovarian cancer. Nat Rev Cancer 2015;15: 668–79. 84. Etemadmoghadam D, Weir BA, Au-Yeung G, Alsop K, Mitchell G, George J, et al. Synthetic lethality between CCNE1 amplification and loss of BRCA1. Proc Natl Acad Sci U S A 2013;110:19489–94. 85. Jones RM, Mortusewicz O, Afzal I, Lorvellec M, Garcia P, Helleday T, et al. Increased replication initiation and conflicts with transcription underlie Cyclin E-induced replication stress. Oncogene 2013;32:3744–53. 86. Lee J-M, Karzai FH, Zimmer A, Annunziata CM, Lipkowitz S, Parker B, et al. A phase II study of the cell cycle checkpoint kinases 1 and 2 inhibitor (LY2606368; Prexasertib monomesylate monohydrate) in sporadic highgrade serous ovarian cancer (HGSOC) and germline BRCA mutationassociated ovarian cancer (gBRCAmþ OvCa). Ann Oncol 2016;27Suppl 6:855O. Clin Cancer Res; 23(13) July 1, 2017 Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research. OF9 Published OnlineFirst March 22, 2017; DOI: 10.1158/1078-0432.CCR-16-0083 Achieving Precision Death with Cell-Cycle Inhibitors that Target DNA Replication and Repair Aimee Bence Lin, Samuel C. McNeely and Richard P. Beckmann Clin Cancer Res Published OnlineFirst March 22, 2017. Updated version E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: doi:10.1158/1078-0432.CCR-16-0083 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on August 3, 2017. © 2017 American Association for Cancer Research.