Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Onchocerciasis
DR JOSHUA NDOM GIYAN (FWACP)
MEDICAL DIRECTOR/CHIEF EXECUTIVE
FEDERAL MEDICAL CENTER, KEFFI.
OUTLINE
•
•
•
•
•
•
•
•
Introduction/brief history
Epidemiology
Lifecycle
Clinical features
Diagnosis/differential diagnosis
Treatment
Prevention and Control
Conclusion /references
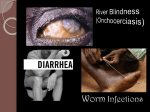
Onchocerciasis
(River Blindness or Robles disease )
• River Blindness, is a parasitic disease.
• It is the second leading infectious cause
of blindness after trachoma
.
• one of the neglected tropical diseases.
River blindness is caused by Nematode of order
Filariidae
Onchocerca volvulus
-
• River blindness is transmitted to humans by blackfly
of the Simulium spp.
• These blackflies breed in fast-flowing rivers and
streams.
• Onchocerciasis is a vectorborne disease, where
human beings are the only natural vertebrate host.
A Short History
1893: Rudolf
Leuckhart
describes
morphology of
adult worms in
subcutaneous
nodules
1875: John
O’Neill first
reports the
presence of
microfilaria in
Onchocerciasis
patients in
Ghana
1917: Rodolfo
Robles publishes
findings on a “new
disease” which
includes
subcutaneous
nodules, anterior
ocular lesions,
dermatitis, and
microfilariae
1975: Fungus that
produces chemical
toxic to parasitic
worms discovered
in Japanese soil
sample, from
which scientists
develop
avermectins
2009: First
evidence that
Onchocerciasis
can be eliminated
with Ivermectin
published in the
journal Neglected
Tropical Diseases
1995: WHO establishes
The African Program for
Onchocerciasis Control
(APOC)
1987: Merck & Co
agrees to donate
Ivermectin to all
countries where
River Blindness is
endemic
Epidemiology
• Global Onchocerciasis prevalence is about 18
million(WHO).
• About 270,000 individuals develop blindness
• Another 500,000 have severe visual
impairment.
• 6.5million suffer severe itching or dermatitis.
• 99% of cases occur in 31 African countries
• The remainder is in Yemen and six countries in
the American continent.
Epidemiology 2
• In July 2016, Guatemala became the fourth
country in the world to be verified free of
onchocerciasis .
• after Colombia (2013)
• Ecuador (2014)
• Mexico (2015)
• after successfully implementing elimination
activities for decades.
Epidemiology {Nigeria}
• Onchocerciasis in Nigeria accounts for 40% of
the global disease burden.
• Approximately 40million are at risk of the
disease
• 7-10 million people infected with Onchocerca
Volvulus.
• 7 endemic states in Nigeria are;
• Abia, Anambra, Delta, Ebonyi, Edo, Enugu,
Imo.
Epidemiology {Nigeria} 2
A study by Uttah et al in Calabar revealed;
• 37% of those examined were positive for
Onchocerca volvulus microfilariae
• (39.2% of males and 34.9% of females).
River Blindness primarily affects the tropics of
Africa and the Americas
LIFE CYCLE
An infected female blackfly
takes a blood meal from a host.
The hosts skin is stretched by
the fly’s apical teeth and cut by
its mandible.
Onchocerciasis is linked with
fast flowing rivers where
Simulium blackflies breed.
OVERVIEW OF LIFE CYCLE
LIFE CYCLE
Microfilariae also can travel to
the eye, causing blindness.
Some microfilariae die causing
skin rashes, lesions, intense
itching, or skin depigmentation.
Clinical Features
• The intensity of human infection is related to the
number of infectious bites endured by an
individual.
• Blindness is almost always in persons with
intense infection.
• Incubation Period : 9 – 24 months.
• Adult worms remain in subcutaneous nodules
• Microfilariae induce intense inflammatory
responses, especially upon their death
Clinical Features 2
• An individual may be asymptomatic.
• Those with symptoms usually experience
-Subcutanoeus nodules
- Skin rashes
- Eye lesions; which can progress to blindness.
• Symptoms appear after the L3 larvae mature
into adult worm.
Skin Manifestation
• Diffuse papular dermatitis, often with intense
pruritis
• Subcutaneous nodules (onchocercomata)
- Firm, mobile and non-tender
- Commonly over bony prominences
- Trunk and hips(Africa)
- Head and shoulders(Americas)
• Peripheral lymphadenopathy
Skin Manifestation 2
• Chronic infection leading to
Papular rashes – onchodermatitis
"leopard skin" appearance ; bilateral,
symmetric ,patchy depigmentation of the
shins.
"cigarette-paper" appearance or
"hanging groin“ as a result of skin
elasticity and atrophy.
Leopard skin
Hanging groin
Eye Manifestation
• Early symptoms;
- itchy eyes, redness, or photophobia.
- Snow-flake opacities from punctate keratitis.
- Inflammation of the optic nerve resulting in
-vision loss, particularly peripheral vision.
- eventually blindness.
Eye Manifestation
• Chronic eye manifestation.
• initially reversible lesions on the cornea .
• Without treatment can progress to;
- Sclerosing keratitis and iridiocyclitis.
- Glaucoma and choroiditis often resulting in
blindness.
Diagnosis
• Definitive :
Skin snip biopsy:
- demonstrate microfilariae. 100% specificity in
experienced hands
- but 20-50% sensitivity in early stages.
Excisional biopsy of nodules.
Slit lamp examination of eyes.
= may reveal microfilariae in the cornea and
anterior chamber.
Diagnosis 2
• Mazzoti test; 10% diethylcarbamazine(DEC)
-pruritus and pustular onchodermatitis develop after 24- 48hrs.
-It is useful in detecting infected patients in whom no microfilariae
can be detected.
• Serology : skin snip
- Ov16 card test
- ELISA
- Oncho-27 antigens
- PCR
• Ancillary tests :
- FBC: eosinophilia
- Elevated serum IgE
Differential Diagnoses
•
•
•
•
•
•
•
•
•
Delayed Hypersensitivity Reactions
Food Allergies
Leprosy
Lichen Planus
Loa loa infection
Lymphatic filariasis
Scabies
Syphilis
Vitamin A Deficiency
Management
•
-
Usually multidisciplinary involving the
Primary care physician.
Infectious disease specialist
Ophthalmologist
Dermatologist
Treatment
• Ivermectin PO 150 µg/kg every 6-12 months.
-Has microfilaricidal effect.
-Treatment of choice.
- This medication will not cure the disease but it
will slow down its progress.
• WHO recommends treating with ivermectin at
least once yearly for between 10 to 15 years.
OR
• Doxycycline 100-200mg/day for 6 weeks.
- It kills both microfilariae and adult worms.
Prevention
• Various control programs aim to stop
onchocerciasis from being a public health
problem.
Onchocerciasis Control program (OCP)
The African Programme for Onchocerciasis
Control (APOC)
The Expanded Special Project for the
Elimination of Neglected Tropical Diseases in
Africa (ESPEN)
Onchocerciasis Control Program (OCP)
• Launched by WHO in 1974
• using mainly the spraying of insecticides against
blackfly larvae (vector control) by helicopters and
airplanes.
• This was supplemented by large-scale
distribution of ivermectin since 1989.
- Relieved 40 million people from infection
- Prevented blindness in 600 000 people
- Ensured that 18 million children were born free
from the threat of the disease and blindness.
The African Programme for Onchocerciasis
Control (APOC)
• was launched in 1995
• Objective was controlling onchocerciasis in the remaining
endemic countries in Africa
• Closed at the end of 2015 after beginning the transition to
onchocerciasis elimination.
• Its main strategy has been
-the establishment of sustainable community-directed
treatment with ivermectin (CDTI)
- vector control with environmentally-safe methods where
appropriate.
• In 2015, more than 114 million people were treated in in
Africa where the strategy of CDTI was being implemented
The Expanded Special Project for the Elimination of
Neglected Tropical Diseases in Africa (ESPEN)
• was officially launched at the World Health
Assembly in May 2016.
• Its roles include;
• Focus on several priority countries to support to
(NTDs) programs.
• Create a pool of experts that can provide
technical assistance to all member countries.
• ESPEN, like OCP and APOC, is housed in the WHO
Regional Office for Africa.
The Nigerian Story
• The national health policy was introduced in 1988
• the onchocerciasis policy as a national health
intervention was put forward in 2004.
• Ultimate goal; to eliminate onchocerciasis as a
public health problem through
- strengthening of self-sustainable prevention and
control programmes in endemic communities.
-The global target for the elimination of NTDs is
2020
• The policy was to achieve and maintain
nationwide coverage.
• A minimum of 65% coverage nationwide
by the end of 2012 was envisaged.
• Nigeria was the first country to use
community-directed treatment (CDT)
with Ivermectin
• Ivermectin for treatment of
onchocerciasis was introduced in Nigeria
in 1991.
Appraisal of the Nigerian Situation
• Health education on NTDs remained very poor,
• The community had not fully realized its
responsibility for the drug distribution and NTDs
control.
• The community drug distributor (CDDs) had not
been developed as a substantial team working for
other projects.
• The goals of community-directed treatment with
ivermectin (CDTI) only have been partly met
Conclusion
• Onchocerciasis is a disease caused by
Onchocerca volvulus
• It is the second most common cause of
blindness due to infection.
• It is transmitted by blackfly which thrives in
fast flowing waters.
• Various programmes have been developed to
effectively prevent and control the disease
Conclusion 2
• The control of onchocerciasis as a public
health problem has been achieved with
significant success in the OCP countries in
West Africa
• APOC countries, covering all remaining
onchocerciasis endemic countries in Africa.
• The objective of large-scale ivermectin
treatment is changing from onchocerciasis
control to onchocerciasis elimination.
References
• World Health Organization. Onchocerciasis
and its control. Report of a WHO Expert
Committee on Onchocerciasis Control.
Geneva: World Health Organization; 2009.
• Boatin B. The Onchocerciasis Control
Programme in West Africa . Ann Trop Med
Parasitol. 2008;102(1):13–17.
• Korevaar DA, Visser BJ. Reviewing the
evidence on nodding syndrome, a mysterious
tropical disorder. Int J Infect Dis.
2013;17(3):149–52.
References 2
• Thylefors B. The Mectizan Donation Program .
Ann Trop Med Parasitol. 2008;102(1):39–44.
• Duerr HP, Raddatz G, Eichner M. Control of
onchocerciasis in Africa: threshold shifts,
breakpoints and rules for elimination. Int J
Parasitol. 2011;41(5):581–9.
• World Health Organisation: Guidelines for
stopping mass drug administration and
verifying elimination of human onchocerciasis:
criteria and procedures. World Health
Organisation; 2016.
THANK YOU FOR
LISTENING