Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
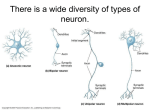
Motor Neuron Diseases Introductory article Article Contents Michael Donaghy, University of Oxford, Oxford, UK . Introduction Motor neuron disease is an umbrella term referring to a group of diseases in which there is death of the lower motor neurons and/or the upper motor neurons. Some of these diseases are genetic, but most occur sporadically, that is unpredictably without any identified environmental or genetic cause. . Pathophysiology of ALS . Frequency and Clinical Importance of ALS . Major Clinical Features and Complications of ALS . Prognosis and Management of ALS . Pure Lower Motor Neuron Syndromes Introduction . Pure Upper Motor Neuron Disorders . Summary Although many use the term ‘motor neuron disease’ to refer to amyotrophic lateral sclerosis (ALS), the most common and serious of these disorders occurring in adults, there are a wide variety of different motor neuron diseases, of varying severity, affecting all ages from infancy onwards (Table 1). This death of motor neurons is a form of neurodegenerative disease and results in paralysis of the limb and swallowing muscles. This degenerative process causes various disabilities, such as inability to walk, use the arms, swallow or speak, and it may lead to death when the breathing muscles become involved. Table 1 Classification of the motor neuron diseases Combined upper and lower motor neuron involvement Amyotrophic lateral sclerosis Sporadic (A, E) Familial adult onset (A) [ad] Familial juvenile onset (c) [ar] Pure lower motor neuron involvement Proximal hereditary motor neuronopathy Acute infantile form (Werdnig–Hoffmann; I) [ar] Chronic childhood form (Kugelberg–Welander; I, C) [ar] Adult onset forms (A) [ar] [ad] Hereditary bulbar palsy With deafness (Brown–Violetta–Van Laere; C, A) [?] Without deafness (Fazio–Londe; C) [ar] X-linked bulbospinal neuronopathy (A, E) [slr] Hexosaminidase deficiency (C, A) [ar] Multifocal motor neuropathies (A, E) Postpolio syndrome (E) Postirradiation syndrome (A, E) Monomelic, focal or segmental spinal muscular atrophy (A) Pure upper motor neuron involvement Primary lateral sclerosis (A, E) Hereditary spastic paraplegia (A, E) [ar] Lathyrism (A) Konzo (A) There are two types of motor neurons, the lower and the upper (Figure 1). Lower motor neuron cell bodies are located in the anterior horn of the spinal cord and in the brainstem. Their axons branch to innervate a group of muscle fibres within the limbs, trunk, throat or face. The group of muscle fibres innervated by a single lower motor neuron is known as a motor unit. When a motor unit is diseased, as in a motor neuron disease, it sometimes fires spontaneously without any voluntary or reflex stimulus, and all the muscle fibres of its motor unit contract simultaneously. This causes a visible flickering in the muscle belly known as a fasciculation, which can also be detected by electromyographic recording from the muscle. When a lower motor neuron degenerates, the muscle fibres of its motor unit atrophy due to loss of activity and trophic influences. With loss of many of the motor neurons innervating any particular muscle, the muscle will visibly waste. Thus, the clinical features of lower motor neuron loss are weakness, wasting and fasciculations. The upper motor neuron cell bodies are located in the cerebral cortex of the brain, principally in the primary motor cortex. Their axons descend through the brainstem and spinal cord in the pyramidal tracts. Many terminate on neuronal circuits which influence how lower motor neurons control movement. Some upper motor neurons, known as Betz cells, synapse directly with the lower motor neurons and are particularly responsible for controlling complex short latency movements such as individual finger movements. In addition to paralysis, upper motor neuron damage causes spastic stiffness of limb muscles, brisk tendon reflexes, and a characteristic extension of the great toe on stroking the sole of the foot, the so-called Babinski response. ALS causes degeneration both of the lower motor neurons in the spinal cord and brainstem, which directly control voluntary (striated) muscles, and of the upper motor neurons in the motor areas of the cerebral cortex, which direct and integrate the activity of these lower motor neurons. By contrast the other forms of motor neuron disease affect either the lower motor neurons or the upper motor neurons but not both. This article focuses on ALS, also known as Lou Gehrig disease. ENCYCLOPEDIA OF LIFE SCIENCES © 2002, John Wiley & Sons, Ltd. www.els.net 1 Motor Neuron Diseases Upper motor neurons Cerebral cortex Thalamus Mesencephalon Internal capsule Pons Cranial nerve motor nuclei Medulla oblongata Medullary pyramid The cause of sporadic ALS is unknown but nerve terminals from affected regions show defective uptake of the potentially toxic excitatory amino acid neurotransmitter, glutamate. This observation led to the development of the antiglutamate agent, riluzole, the first treatment shown to slow the progression of ALS. Twenty to 40% of hereditary amyotrophic lateral sclerosis cases are associated with mutations in the gene for Cu/Zn superoxide dismutase 1 on chromosome 21, which catalyses conversion of toxic superoxide anion free radicals to hydrogen peroxide. The mechanism whereby this enzyme abnormality causes motor neuron disease is unknown; various proposals include loss of the normal ability to detoxify free radicals allowing them to accumulate intracellularly, the possibility that the mutated enzyme protein agglomerates intracellularly in deposits which damage the motor neuron or that it affects the mitochondria, which are energy sources within cells. Introduction of this mutant enzyme transgenically into mice causes motor neuron degeneration, thereby providing the first good animal model of motor neuron disease. Pyramidal decussation Spinal cord Pyramidal tract Lower motor neurons Figure 1 Schematic representation showing the course of the pyramidal tract, the homuncular organization of the motor cortex in the precentral gyrus, the concentration of the motor output within the internal capsule, and the decussation of the pyramidal tract in the medulla oblongata. (From Donaghy M (1997) Neurology, Oxford University Press.) Pathophysiology of ALS Pathological examination of the spinal cord and brain of those who have died from amyotrophic lateral sclerosis shows extensive loss of lower (alpha) motor neurons, and also of the upper motor neurons from the motor cerebral cortex. Many of the surviving motor neurons show abnormalities indicating that they are in the earlier stages of degeneration, particularly spheroids (round particles) composed of disorganized elements of the normal intracellular cytoskeletal proteins in the proximal axon. Although 90% of ALS cases occur sporadically, 10% are inherited, usually on an autosomal dominant basis, that is with a one in two chance of directly inheriting the disease from an affected parent. 2 Frequency and Clinical Importance of ALS ALS occurs worldwide with an incidence of up to 2 cases per 100 000 of the population; men are twice as frequently affected as women. Particular geographical foci of an increased incidence of ALS have been noted, such as the Pacific island of Guam, where it is thought that dietary factors are responsible. Although relatively uncommon, ALS is a widely dreaded disease because of its relentless progression which eventually makes patients with normal mental function prisoners within bodies that no longer move, and ultimately leads to an undignified death. Caring for patients with ALS causes great distress to relatives, usually the spouse, and places a considerable burden upon disability healthcare services. Major Clinical Features and Complications of ALS The first symptom of ALS is usually either weakness of one limb, difficulty with swallowing, or an alteration in the quality of the voice. As the months go by, weakness and wasting spread to other parts of the body, and progressively worsen. Many patients experience muscle cramping, and inspection of the limb muscles shows involuntary flickering movements of the muscles called fasciculations. Clinical neurophysiological studies, undertaken for the purposes of diagnosis, show that these fasciculations are Motor Neuron Diseases due to simultaneous contraction of the group of muscle fibres within the motor unit innervated by a diseased motor neuron. In most patients, that muscle region which was first affected usually continues to be the worst affected. Depending upon which muscle region is predominantly weakened, patients ultimately become unable to walk, or to use their arms and hands, or to swallow, or to speak. Intellectual function remains normal, and there is no involvement of skin sensation, or of the control of the bladder or bowel. Interestingly, the striated muscles which control eye movements are not affected. Patients with advanced forms of ALS may become breathless because of failure of breathing muscles, or may experience potentially fatal choking attacks because the throat weakness allows food and liquid to be inhaled rather than swallowed. Apart from these respiratory complications of ALS, malnutrition due to impaired swallowing is the other major complication affecting general health. Prognosis and Management of ALS Of those with onset in the swallowing muscles, only 5% survive 5 years. Survival is rather better for those with limb muscle onset, of whom 15% survive 5 years. Death usually results from respiratory failure, often with associated pneumonia or choking, and general malnutrition may contribute. Malnutrition due to swallowing muscle failure can be circumvented by placing percutaneous feeding gastrostomy tubes through the abdominal wall directly into the stomach, thereby bypassing the throat. Walking aids, wheelchairs and devices to improve hand function in those with weak arms can be of assistance to affected individuals. Some patients with distressing breathlessness due to breathing muscle failure may be helped by continuous positive airways pressure at night, in which a slightly positive air pressure is delivered via a face mask. More definitive treatment of respiratory failure with tracheostomy and formal endotracheal ventilation is rarely advised because it will simply prolong the patient’s life whilst their limb, swallowing and speaking muscles fail relentlessly. The pastoral care of patients with ALS is all important, both in the manner in which one tells the patient about the diagnosis early on, and in advising him or her humanely about the best management in the later stages. Trials of drug therapy have aimed to slow the downhill progress of the disease or improve survival. The antiglutamate drug riluzole improves survival at 18 months by 35%, although there seems to be no significant benefit in terms of muscle function. This drug represents an important advance in that it is the first effective intervention in the natural history of ALS. There is much activity devoted to finding effective treatments to slow or halt motor neuron degeneration, but thus far with little success. Pure Lower Motor Neuron Syndromes There are a wide range of pure lower motor neuron syndromes, often known by the alternative name of spinal muscular atrophy, which occur at all ages of life. The commonest and most severe form is inherited, occurs in infants and is known as Werdnig–Hoffmann disease or spinal muscular atrophy (SMA) type 1. This disorder is the second most common fatal autosomal recessive disease of childhood and occurs once in every 20 000 births. Affected babies are weak from birth, or soon after, can only suck weakly, and normally die of respiratory failure within a year. Mutations in the survival motor neuron gene (SMN) occur in 98% of these patients but the mechanism whereby this genetic mutation causes motor neuron abnormalities is not yet known. Less severe forms of inherited spinal muscular atrophy also occur in older children, adolescents and adults and some of these too are associated with SMN gene abnormalities. A distinctive inherited sex-linked form of spinal muscular atrophy, only occurring in men, is called Xlinked bulbospinal neuronopathy or Kennedy syndrome. This occurs at various ages of adulthood, with the most serious weakness affecting the tongue and swallowing muscles. The disease is due to an expanded CAG trinucleotide repeat sequence within the androgen receptor gene on the X-chromosome. The reason why this mutation of a sex-hormone receptor causes motor neuron degeneration is not clear but may involve cellular damage induced by deposition of the aberrant receptor protein. The patients also show general evidence of inadequate testosterone influence, but this hormonal state is unlikely to be directly responsible for the motor neuron disease. Sporadic lower motor neuron syndromes also occur. A small proportion of those who have suffered paralysis due to acute poliomyelitis (polio) will develop a slowly worsening weakness of the affected limb, more than two decades later. Self-limited spinal muscular atrophies occasionally occur, particularly in young men, and often only affecting one arm. Multifocal motor neuropathy is a condition resembling spinal muscular atrophy in which diagnostic neurophysiological tests show the problem to be one of focal blocking of the passage of action potentials along motor nerve fibres, rather than true degeneration of the motor axons. This disorder often responds dramatically within a few days of intravenous infusions with high dose human immunoglobulin. Motor neuron diseases occasionally occur in association with benign or malignant tumours. Lower motor neuron syndromes are well recognized in association with proliferations of lymph node tissue, both in the form of malignant lymphomas and with the production of monoclonal immunoglobulins by benign lymphocyte proliferations. 3 Motor Neuron Diseases Pure Upper Motor Neuron Disorders These are the rarest forms of motor neuron disease. A sporadic condition known as primary lateral sclerosis causes stiffness and weakness of the limbs, voice or swallowing muscles due to degeneration of the upper motor neurons. A similar picture can occur, although usually earlier in adult life with less progressive deterioration, in an autosomal dominantly inherited condition known as hereditary spastic paraplegia. It is of interest to note that pure upper motor neuron degenerations have occurred following dietary consumption of Lathyrus sativus, the chickling pea vetch, during famine conditions, causing the disease neurolathyrism which mainly occurs in India, and following consumption of dietary cyanide derived from the flour of cassava root, during famine causing konzo in Central Africa. Summary Various sporadic and inherited degenerations affect the lower and upper motor neurons to cause paralysis of limb, swallowing and breathing muscles. This selective motor neuron degeneration appears to be a common endpoint of diverse pathophysiological processes ranging from altered glutamate handling, to abnormalities of free radical detoxifying enzymes, mutations in genes affecting neuronal survival during early development, and in the gene for the androgen receptor. Although an antiglutamate drug has been shown to improve the natural history of one form of motor neuron disease, the fatal amyotrophic lateral sclerosis of adults, it seems likely that a wider range of therapies will have to be developed specific to the different 4 abnormalities of cell biology causing these diverse motor neuron syndromes. This is an important challenge to modern pharmacological medicine given the disabling, distressing, and often fatal nature of these disorders. Further Reading Amato AA, Prior TW, Barohn RJ et al. (1993) Kennedy’s disease: a clinico-pathologic correlation with mutations in the androgen receptor gene. Neurology 43: 791–794. Dalakas MC, Elder G, Hallett M et al. (1986) A long-term follow-up study of patients with post-poliomyelitis neuromuscular symptoms. New England Journal of Medicine 314: 959–963. Donaghy M (1995) Motor neuron diseases in adults. In: Kennard C (ed.) Recent Advances in Clinical Neurology 8, pp. 73–88. Edinburgh, UK: Churchill Livingstone. Donaghy M (1999) Classification and clinical features of motor neurone diseases and motor neuropathies in adults. Journal of Neurology 246: 331–333. Gordon PH, Rowland LP, Younger DS et al. (1997) Lymphoproliferative disorders and motor neurone disease. Neurology 48: 1671–1678. Gurney ME, Pu H, Chiu AY et al. (1994) Motor neuron degeneration in mice that express a human Cn, Zn superoxide dismutase mutation. Science 164: 1772–1775. Lefebvre S, Burglen L, Frezal J et al. (1998) The role of the SMN gene in proximal spinal muscular atrophy. Human Molecular Genetics 7: 1531–1536. Pringle CE, Hudson AJ, Munoz DG et al. (1992) Primary lateral sclerosis. Clinical features, neuropathology and diagnostic criteria. Brain 115: 495–520. Rosen DR, Siddique T, Patterson D et al. (1993) Mutations in Cu/Zn superoxide dismutase gene are associated with familial amyotrophic lateral sclerosis. Nature 362: 59–62. Rothstein JD, Martin LJ and Kuncl RW (1992) Decreased glutamate transport by the brain and spinal cord in amyotrophic lateral sclerosis. New England Journal of Medicine 326: 1464–1468.