Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
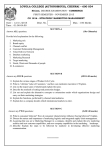
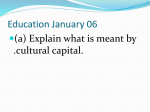
SAQ practice MH week 2 – orthopaedics and trauma 1. A 19 year old man has presented to your rural ED after falling on to his out-stretched hand while playing basketball. He is complaining of wrist pain. There are no wounds visible. AP and lateral xrays of his wrist are given. 1. List the 2 main abnormalities shown on the xrays. (2 marks) _____________________________________________________________________ 2. List the 2 mot serious possible immediate complications of this injury (2 marks) _____________________________________________________________________ You have elected to perform a Bier’s block in your management of this injury. 3. List the steps involved in performing a Birer’s block, including drugs, doses and end-points where appropriate. ( 6 marks) 1. (trans-scaphoid) Peri-lunate dislocation, scaphoid fracture 2. Median nerve injury, vascular compromise 3. Consent – 1 mark Preparation – cardiac monitor, IV access *2 (one each arm – below fracture) Cuff – inflate to 100mmHg above systolic BP LA – prilocaine 2.5mg/kg (Manipulate fracture and plaster) – not essential in this question Cuff to stay up at least 30min (CRITICAL ERROR) – 1 mark Deflate cuff and observe 15 min for toxicity Q3 – ó mark for concept, extra ó mark for specifics Pass Q3 – 3/6 Total pass – 7/10 2. A 56 year old man has been brought to your tertiary ED after a motorcycle accident. His pelvic xray is given. 1. Classify his pelvic injury based on the Xray provided. (2 marks) _________________________________________________________________ 2. List 4 possible methods of arresting the blood loss from his pelvic injury. (4 marks) CT scans have revealed active arterial haemorrhage related to his pelvic injury, but no other obvious injuries. His vital signs are: GCS 14 E4 V4 M6 Pulse 135 /min BP 70/40 mmHg O2 saturation 98% 6L O2 via mask Temp 36.5 degrees 3. In point form, list your principles of his fluid resuscitation while he is awaiting definitive management of his pelvic injury. (5 marks) __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ 1. Grade 3 antero-posterior compression fracture of the pelvis (right side) Pass 1 2. Pelvic binder, interventional radiology, pelvic packing in OT, ORIF in OT Pass any 3 out of 4 3. Minimal volume resuscitation Targets: systolic BP 80mmHg, radial pulse, mentation Use blood products, minimal crystalloid Initially O neg then Xmatched Initiate massive transfusion protocol early Aim packed cells:FFP:platelets 1:1:1 ratio (targeted to ROTEM acceptable) Each point 1 mark but has to show clinical reasoning Pass 3/5 Total pass 7/11 corrects to 6/10 SAQ 3 A 29 year old man has been brought to your hospital after being hit to the head by a baseball bat. He has no prior medical history. His vital signs on arrival to the ED are: GCS 11 E2 V2 M5 Pulse 110 /min BP 110/65 mmHg O2 sats 99% 6L O2 via mask A CT scan of his head has been performed. 1. List 5 abnormalities on the CT slice. (5 marks) ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ 2. List your treatment priorities in the ED. Where appropriate, give end-points. (9 marks) ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ Large extradural haematoma – high density bi convex lesion left temporal region Hyperacute extradural with “swirl sign” mixed density Large scalp haematoma left temporal region Parietal cerebral contusion left Significant midline shift to right Loss of sulci and gyri consistent with raised intracranial pressure Pass 3 of 5 2. Immediate neurosurgical referral for surgical drainage of haematoma Intubation for airway control and management of CO2 Maintain MAP >80 (accept approx.) mmHg with IV N/S +/- noradrenaline infusion Maintain oxygenation sats >95% Ventilate for low normal CO2 (35 – 40) Other neuroprotective measures (max 4 marks) Well sedated, paralysed Slightly head-up position Loosen ties / restriction to venous return Na high normal range Normothermia normoglycaemia pass 5 of 9 total pass 8 of 14 corrects to 5.5/10 SAQ 4 A 45 year old man has been brought to your ED by ambulance after being stabbed once in the right side of the chest. On arrival, his vital signs are: GCS 15 E4 V4 M6 Pulse 120 /min BP 85/40 mmHg O2 sats 94% 15L O2 via non-rebreather mask A chest Xray has been performed. 1. Give the main abnormality on the chest Xray, with supporting evidence. (3 marks) ______________________________________________________________________________ ______________________________________________________________________________ ____________________________________________________________________________ 2. List the steps involved in inserting an intercostal catheter in this patient. (9 marks) _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________ ____________________________________________________________________________ Right sided tension haemothorax (CRITICAL) - Veiled opacity to right hemi-thorax - Significant rim of fluid around lateral lung edge - Mediastinal shift to left 1 mark for haemothorax, ó marks for – tension, 3 other bits pass 2 of 3 2. Verbal consent / explanation (sedation optional) (Gown / gloves / mask / goggles) Clean chest with anti-septic (appreciate this is a time critical procedure) Local anaesthesia – lignocaine 1% with adrenaline 20mL Location - 5th interspace mid-axillary line Incision with scalpel Blunt dissection to pleural space / finger sweep Insertion ICC 28-32 Fr Connection to underwater seal Suture and dressing Pass 7 of 9 Total pass 9/12 corrects to 7.5/10 Question 5 A 25 year-old male involved in a motorbike accident was brought to the ED at a tertiary level centre. A trauma series was performed with a normal CXR and C-spine Xray. The following radiological imaging was undertaken. Vital signs are: RR 20 sat 99% on room air HR 115 BP 80/50 GCS 15 1. List the abnormalities on this Xray (2 marks) pubic symphysis diastasis – APC or VS injury contrast leakage consistent with urethral rupture 2. What clinical signs are associated with this injury on examination (1 mark) high riding or boggy prostate blood at the urethral meatus perineal or scrotal haematoma 3. Give the 4 most likely causes of hypotension in this patient (2 marks) pelvic venous or arterial haemorrhage intra- abdominal heamorrhage spinal shock/ injury long bone fracture NB need all 4 to score 2 marks, 2-3 scores 1 mark, 0-1 scores 0 4. List the five most important treatment and disposition priorities, as the team leader, in treating this patient’s hypotension. Give details (5 marks) pelvic immobilisation – external binder/ sheet, minimal pelvic movements resuscitation - massive transfusion protocol – blood/ platelets/ FFP 1:1:1, cryoprecipitate, tranexamic acid FAST scan – angiography and laparotomy if positive; angiography if –ve and readily available urgently notify theatres/ interventional radiology/ orthopaedic surgeon/ trauma surgeon/ anaesthetist/ blood bank/ prepare staff and equipment for transfer – monitors, IV access, drugs for intubation/ analgesia maintain normothermia – warm fluids, external radiant heater SAQ 6 A 42 year old man fell off his bicycle when travelling at 20km/h. He complained of left forearm pain. He had the following X-rays taken. 1. What are the abnormalities on the X-ray? (2 marks) transverse fracture through the mid shaft of the left radius, which is associated wit h 100% dorsal displacement and shortening of 1.5cm distal radius is angulated 15 degrees in the palmar direction distal ulnar-carpal joint is dislocated with dorsal displacement of the ulnar head 2. List the 2 most likely nerve injuries (2 marks) ulnar nerve interosseous branch of median nerve 3. Your registrar decides to perform procedural sedation. Outline your checklist with details of each of the major area. (6 marks) consent assessment of patient – fasting status, allergies,meds, MP, ASA check airway equipment – CO2, airway, mask, ETT, laryngoscope, suction iv with fluids running medications labelled monitoring – sats, BP, ECG, CO2 SAQ 7 A 5 year old boy has been brought to your emergency department after a road traffic accident. He has had a blood transfusion commenced by the retrieval service for haemorrhagic shock. The second unit has already been commenced. 1. What is the definition of massive transfusion in this child? (2 marks) Transfusion of more than 40 mls/kg (blood volume of children older than a neonate is approximately 80 mls/kg. 2. List eight potential complications of massive transfusion for this child (4 marks) hyperkalaemia hypocalcaemia Acid base derangement and lactic acidosis Dilutional thrombocytopenia disseminated intravascular coagulation Systemic hypothermia Transfusion reactions TRALI: transfusion related acute lung injury 3. If he was to have a cardiac arrest. What are the 4 likely causes (4 marks) Hypoxia Tension pneumothorax Tamponade Hypovolaemia from blood loss Question 8 A 20yo male attends with a grossly swollen painful hand from a punching injury at 36 hours. There is broken skin over the 3rd MCP joint. (a) What complications may arise from this injury? (20%) (b) Outline your examination (20%) (c) Given the appearance of the hand shown, what investigations would you request, assuming no comorbidities and that this is an isolated injury? (20%) (d) What are the indications for admission? (20%) Answers: 1a. Joint penetration Septic arthritis Metacarpal fracture Extensor tendon laceration Extensor tendon sheath infection Extensor tendon rupture Marking. 20% of the total for question 1 pass =4/6 =10% of total for question 1, add 5% for each additional correct item up to a total of 20% 1b. Anatomic assessment of skin wound (position, depth, and visible involvement of underlying structures. Signs of infection: Local and spread (lymphangitis, nodes, and temperature) Functional assessment: nerve, extensor tendon, joint, bone and vascular Survey for other injuries Question 9 Whist restraining a 47yo male with a convulsive seizure a nurse was kneed in the cheek, including the orbit and nose. She experienced immediate epistaxis, facial pain and visual blurring. (photo) (a) Assuming that this is an isolated facial injury without loss of consciousness, list six potential immediate ocular complications that you would exclude. (25%) (b) What non-occular complications would you seek to exclude? (25%) (c) Describe your management of a probable acutely fractured nose. (25%) (d) What are the clinical signs of orbital compartment syndrome? What is the immediate management? (25%) 7a. Globe rupture, hyphaema, retinal tear and detachment, vitreous haemorrhage and detachment, choroidal tear/rupture, iris injury, traumatic iritis, lens detachment, corneal abrasion, commotion retinae, orbital fracture, orbital compartment syndrome, orbital content entrapment in the fractured orbital floor. 7b. Inferior orbital nerve injury (sensory loss), nasal septal haematoma (fractured nose), depressed fractured maxilla), orbital floor fracture and entrapment of orbital fat (enophthalmos) and inferior rectus (diplopia). Pass = 4 complications 7c. Analgesia, control epistaxis, exclude/drain septal haematoma, only image in the context of surveying for facial fractures, exclude orbital injury and inferior orbital nerve injury, no evidence for antibiotics but argued for and given by many on risk of severe infection (divided debate), Pass must be reasonable and include exclude/drain septal haematoma, no imaging unless excluding facial fractures SAQ 1 (Acute agitation) A 38 year old man walks up to the triage desk. He is agitated, shouting and uncooperative with simple instructions He is poorly kempt, clammy and tremulous. 1. List five differential diagnostic categories you would consider when trying to assess this man? Give two examples from each category. 2. Briefly describe two different strategies for gaining the cooperation of this man? 3. List the legal principles that guide your management? Answers Q 1. Category Trauma Toxidrome Acute withdrawal Electrolyte disorder Environmental Psychiatric Endocrine Sepsis Post-ictal 1. 2. 1. 2. 1. 2. 1. 2. 1. 2. 1. 2. 1. 2. 1. 2. 1. 2. Q2. Example Major visceral injury with blood loss Head injury (bleed, concussion) Amphetamines, opiates, cannabis, usual antipsychotic medication e.g. Lithium Alcohol, serotonin syndrome Alcohol, cannabis Opioids Hypo/hyperglycemia Hyponatremia, hypercalcemia Snake bite Red back spider bite Schizophrenia Acute mania Hyperthyroidism Adrenal crisis CNS Infective endocarditis Known epilepsy, related to causes above Withdrawal seizure Physical versus chemical Q3. Five person physical restraint Chemical restraint: benzodiazepine, butyrophenone, phenothiazine Autonomy vs duty of care Competence Informed consent SAQ 2 (Chest CT post MVC) A 28 year old male presents to ED after being involved in a high speed MVC. He was the driver, restrained, deployed airbag, required extrication. On arrival he is short of breath and complaining of right sided chest pain His SaO2 P BP 95 105 110/70 % on 5l/min by Hudson mask sinus tachycardia afebrile He has no significant past history and is on no medication. A CT chest is performed as part of his workup. A single axial slice is given (SAQ 2 contd…) 1. Give an interpretation of the image providing Five positive findings Two negative findings 2. List three potential complications of these changes. 3. List three options for the treatment of the changes shown. Answers Q1. Positive findings Extensive right and left chest wall surgical emphysema Epidural air Pneumo-mediastinum Right sided pneumothorax Small emphysematous bleb posteriorly No tension No chest tube No haemothorax Tension pneumothorax Air embolism; stroke Airway compromise from tracking to larynx/pharynx Pneumopericardium progressing to cardiac tamponade Negative findings Q2. Q3. Conservative: repeat CXR in 24 hours specifically looking for increase in pneumothorax size with view to ICC Small lumen right sided catheter inserted using Seldinger technique for drainage of pneumothorax Small bore ICC inserted using Seldinger technique Small bore ICC inserted using incision/surgical technique Large bore ICC specifically to treat pneumothorax and possible haemothorax. Catheters on Heimlich valve/UWSD +/- suction 17. A 10 year old girl has fallen off a wall and presents with a “sore arm”. X-ray is shown below. a. Give 3 features which are required to “clear the neck”. (3 marks) Pt fully conscious No evidence of intoxication No neck pain/ midline tenderness No neurological deficit No distracting injury ROM >45o in all directions Age < 65 b. Describe the x-ray. (1 mark) Fracture distal shaft of humerus with posterior displacement c. What is the diagnosis? (1 mark) Supracondyla fracture humerus d. What are 2 potential neurological complications of this injury and how would you test for them? (4 marks) Median nerve palsy- reduced sensation over the palm, reduced thumb opposition and wrist palmar flexion Radial nerve – reduced sensation thumb, reduced wrist dorsiflexion e. Give an example of one other joint injury that can also give rise to nerve injuries. (1 mark) Shoulder dislocation- axillary nerve Neck of fibula fracture- peroneal nerve 19. A 28 year old man has been out kite surfing and was thrown into the water at high speed. He is brought in on a spinal board with C-spine protection. He is intubated and ventilated and put on a propofol infusion. His observations are: Pulse 65 /min, BP 90/60 mmHg and he is warm and well perfused. The C-spine film and tomogram are shown below. a. Describe 3 abnormalities on the x-ray. (3 marks) # body C4, loss of space C3-4, probably soft tissue swelling Burst fracture b. Describe 2 aspects of his cardiovascular status. (2 marks). Hypotensive and bradycardic/normocardic c. What is the likely diagnosis? (2 marks) Spinal shock d. What 3 signs would support this? (3 marks) priapism Pink, well perfused peripheries, flaccid paralysis below level C4, increased tendon jerk reflexes below that level (might be absent initially) loss of sensation, very weak respiratory effort, 30. A 65 year old male presents following a fall. He complains of a painful swollen left wrist. An x-ray of his wrist is shown below. a. Describe his x-ray. (2 marks) Intra-articular fracture of the distal radius with dorsal angulation 1 mark for intra-articular fracture distal radius 1 mark for dorsal angulation No marks given for Colles fracture b. List the contra-indications to performing a Bier's block. (4 marks) 1/2 mark each to maximum of 4 marks from: Refusal of procedure Uncooperative patient Compromised limb circulation Compartment syndrome of affected limb Sickle cell disease Ipsilateral # humerus LA Sensitivity / allergy Staff / area / equipment unavailable Soft tissue injury at tourniquet site Age <10 / Paediatric patient Peripheral vascular disease / Raynauds Systolic >200mmHg Severe liver disease Unstable epilepsy Unable to gain bilateral iv access Taken from Dunn Emergency Medicine Manual 5th Edition Volume 1 Chp 9 Page 159 and Cameron Textbook of Adult Emergency Medicine 3rd Edition Chpt 22.2 Pg 701 c. List the key steps in performing a Bier's block. (4 marks) 1/2 mark each for: 1. Consent - ideally written 2. Area / staff / monitoring 3. Bilateral iv access - no marks if only iv access mentioned must specify bilateral 4. Check equipment 5. Inflate cuff - ideally answer should state >100mmHg above systolic 6. Injection of local anaesthetic - prilocaine ideally but accept lignocaine (as per Dunn & Tintinalli) 7.Perform procedure - MUA wrist 8.Deflate cuff / post-procedural monitoring Taken from Dunn Emergency Medicine Manual 5th Edition Volume 1 Chp 9 Page 159 60. This 32 year old male lost control of a high pressure injector and comes in with a wound on his left lower leg. a. List three complications that are likely to occur within the next 48 hours. (3 marks) 1. Compartment syndrome 2. Tissue necrosis from local trauma 3. Wound infection b. List the management priorities for this injury. (5 marks) a. b. c. d. Elevation Tetanus Plain film to rule out other injury Surgical or orthopaedic admission +/- exploration in OT c. What factors contribute to damage? (3 marks) a. Type of liquid injected b. Location of injury c. Amount injected d. Proximity of nozzle 68. You are the director of a tertiary ED which is a level one trauma centre. Recently the directors of trauma and haematology have both written to you regarding your department’s haphazard use of blood products in the severely injured. You search your intranet and realise that you do not have a policy. a. What are 3 triggers for massive transfusion? (3 marks) Massive Haemorrhage with shock or anaemia, ie Immediate need for uncrossmatched blood due to rapid haemorrhage and anaemia Blood loss exceeding 150 mL/min Need for at least 4 RBC units in the setting of uncontrolled bleeding Replacement of 50% of total blood volume within 3 hours (24pprox.. 35mL/kg in an adult) Coagulopathy in the setting of blood transfusion b. Name 4 physiological or biochemical parameters that should be measured early and often. (2 marks) • • • • • • • • Temperature; Acid–Base Status; Ionised Calcium; Haemoglobin; Platelet Count; PT/INR; APTT; and Fibrinogen Level. c. What is the indication for Cryoprecipitate delivery? (2 marks) Cryoprecipitate is used primarily as a source of fibrinogen (but also contains FVIII, VWF and FXIII). This is found in adequate amounts in FFP, and in dilutional coagulopathy FFP alone may be adequate. Coexisting DIC may increase fibrinogen requirements. Empirical use is unnecessary. Use should be guided by fibrinogen determinations. d. What are the targets for Hb, Platelets and INR in massive transfusion? (3 marks) Hb>80g/L; Platelets >50x109/L; and PT and APTT<1.5 x control.