Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
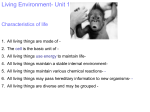
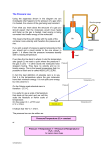
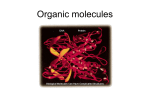
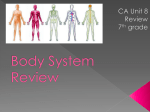
649 Decreased Expression of z Molecules by T Lymphocytes Is Correlated with Disease Progression in Human Immunodeficiency Virus–Infected Persons Minke F. Geertsma, Annelies van Wengen-Stevenhagen, Ellen M. van Dam, Karianne Risberg, Frank P. Kroon, Paul H. P. Groeneveld, and Peter H. Nibbering Department of Infectious Diseases, Leiden University Medical Center, Leiden, The Netherlands In human immunodeficiency virus type 1 (HIV-1) infection, functional activities of T lymphocytes are impaired. Analogous to tumor-infiltrating T lymphocytes from cancer patients, in whom poor proliferative responses are associated with fewer z molecules, this study compared expression of CD3z molecules by T lymphocytes from HIV-infected persons and healthy controls. Flow cytometry and immunoblotting revealed significantly diminished z expression by CD3, CD4, and CD8 T lymphocytes from AIDS patients but not from persons without AIDS. z-mRNA levels were also decreased in cells from AIDS patients. CD3z expression correlated significantly with CD4 cell counts and HIV-1 RNA levels; impaired expression of CD3z molecules appeared to be reversible upon virus load reduction following highly active antiretroviral treatment (HAART). Thus, reduced expression of CD3z molecules by T lymphocytes from HIV-infected persons correlates with disease status. Investigations into CD3z expression by subpopulations of peripheral T lymphocytes and by T lymphocytes in lymphoid tissues will contribute to the understanding of immune reconstitution of HIV-infected patients following HAART. Clinically, human immunodeficiency virus (HIV) infection varies from an asymptomatic phase to full-blown AIDS, characterized by opportunistic infections related to severe defects in cellular immunity. Prior to a profound decrease in the number of peripheral CD4 T lymphocytes, T lymphocytes display impaired proliferative capacity and interleukin-2 (IL-2) production early in HIV infection. Initially, T lymphocyte responses to recall antigens and CD3 cross-linking are diminished, and then their responses to alloantigens and phytohemagglutinin (PHA) are diminished [1–5]. Incubation of T lymphocytes with HIV gene products, such as gp120 and gp41, results in altered cellular functions and in perturbations in lymphocyte signaling [6–8]. This indicates that altered signaling may underlie the impaired functional activities of T lymphocytes from HIV-infected persons. One of the earliest events upon ligation of the T cell receptor complex (TCR) is activation of receptor-associated protein tyrosine kinases (PTKs) p56lck and p59fyn, which then phosphorylate multiple protein substrates, including CD3z molecules [9, Received 28 December 1998; revised 19 April 1999; electronically published 3 August 1999. Presented in part: Eijkman Centennial on Infections in the 21st Century, The Hague, December 1998 (abstract O2). Patients gave informed consent before study participation. The study was approved by the Leiden University Medical Center Medical Ethical Committee. Reprints or correspondence: Dr. M. F. Geertsma, Dept. of Infectious Diseases, Leiden University Medical Center, P.O. Box 9600, 2300 RC Leiden, The Netherlands ([email protected]). The Journal of Infectious Diseases 1999; 180:649–58 q 1999 by the Infectious Diseases Society of America. All rights reserved. 0022-1899/1999/18003-0011$02.00 10]. These molecules contain 3 potential tyrosine phosphorylation motifs [11], which, after phosphorylation, serve as docking sites for SH2 domain–containing signaling proteins, such as the PTK z-associated protein-70 (ZAP-70) [12–14]. Upon binding to z molecules, ZAP-70 is tyrosine phosphorylated and thereby activated [13, 14]. This TCR-associated PTK network up-regulates the activity of several signaling pathways, particularly that mediated by phospholipase Cg1 (PLCg1) [15–17]. Tyrosine phosphorylation of PLCg1 results in increased PLC catalytic activity and activation of the inositol phosphatidyl pathway, yielding the release of diacylglycerol and inositol1,4,5-trisphosphate [18]. These second messengers activate protein kinase C and induce Ca11 mobilization, requirements for the activation of transcription factors for the IL-2 gene promotor, resulting in IL-2 secretion and effector functions [19, 20]. Impairment of the CD3-mediated proliferative response of T lymphocytes from persons with early HIV infection is associated with altered early protein tyrosine phosphorylation, lower levels of p56lck [21, 22], and constitutively higher levels [21] or higher specific activity of p59fyn [22] than in T lymphocytes of healthy controls. Analogous to tumor-infiltrating T lymphocytes from cancer patients, in which poor proliferative responses are associated with lower levels of both p56lck and z molecules [23–25], the present study focused on whether expression of CD3z molecules by T lymphocytes from HIV-infected persons is lower than in healthy controls. Materials and Methods Antibodies. Murine IgG1 monoclonal antibodies (MAbs) TIA2 [26] and 6B10.2 directed against intracellular epitopes of z mol- 650 Geertsma et al. ecules were obtained from Coulter (Hialeah, FL) and Santa Cruz Biotechnology (Santa Cruz, CA), respectively. The hybridoma cell line, producing the negative control murine IgG1 MAb 63D3 directed against CD14, was obtained from the American Type Culture Collection (Rockville, MD). We purchased fluorescein isothiocyanate (FITC)–conjugated F(ab0)2 goat anti-mouse immunoglobulin (GAMFITC, Southern Biotechnology Associates [SBA], Birmingham, AL), peroxidase-conjugated goat anti-mouse immunoglobulin (GAMPO, SBA), and phycoerythrin (PE)conjugated murine IgG1 directed against human CD3 (Leu-4, antiCD3PE), CD4 (Leu-3a, anti-CD4PE), and CD8 (Leu-2a, antiCD8PE) (Becton Dickinson, Mountain View, CA). FITC-conjugated murine IgG1 directed against human CD69 (antiCD69FITC) was obtained from PharMingen (San Diego). Subjects. From March 1996 to October 1996, we enrolled 18 men and 3 women in this study (median age, 42 years; range, 27–65 years). All were patients of the Leiden University Medical Center Infectious Diseases outpatient clinic. By the 1987 Centers for Disease Control (CDC) case definition system [27], 10 patients were categorized as group IV-C1 on the basis of >1 previous opportunistic infection (cytomegalovirus [CMV] retinitis, Candida esophagitis, Pneumocystis carinii pneumonia, cryptococcal meningitis, Mycobacterium avium sepsis, or Cryptosporidium enteritis) or as group IV-D if the subject had Kaposi’s sarcoma. Hereafter, these patients together with 1 patient with severe wasting (IV-A) will be referred to as AIDS patients. The other 10 patients were asymptomatic (CDC group II, n 5 7 ) or mildly symptomatic (CDC group IV-C2, n 5 3) and will be referred to as HIV-positive patients. Numbers of CD4 cells (mean 5 SD) for the AIDS and HIV-positive subjects, respectively, were 32 5 64 cells/mL (range, 1–208) and 270 5 150 cells/mL (range, 86–598). All AIDS patients and 3 HIVpositive patients were on antiretroviral combination treatment consisting of zidovudine/lamivudine, zidovudine/zalcitabine, or lamivudine/zalcitabine. At that time, none was being treated with HIV protease inhibitors. One patient was on maintenance therapy for Mycobacterium tuberculosis infection. In addition to the antiretroviral combination therapy, 12 patients received prophylaxis drugs for P. carinii. In addition, 2 subjects received fluconazol prophylaxis because of recurrent oral candidiasis, 2 had maintenance treatment for CMV retinitis, and 2 received fluconazol prophylaxis and maintenance treatment for both CMV retinitis and disseminated M. avium infection. Controls were 15 healthy volunteers from the hospital staff (14 men, 1 woman; median age, 30 years; range, 21–50 years) without risk factors for HIV; CD41 T lymphocyte counts were not determined in this group. CD41 cells and virus load. CD41 T lymphocytes in HIV-infected patients were measured at the Central Laboratory of the Netherlands Red Cross Blood Transfusion Service (Amsterdam) or at the Central Clinical Haematological Laboratory, Leiden University Medical Centre (LUMC). HIV-1 RNA copies/mL plasma (detection limit ∼400 copies/mL) were determined by Amplicor HIV-1 Monitor test kit (Roche Diagnostic Systems, Branchburg, NJ) at the LUMC Department of Virology. Cell isolation. Forty milliliters of peripheral blood was collected by venipuncture, then heparinized, and subjected to ficollhypaque density gradient centrifugation. Peripheral blood mononuclear cells (PBMC) collected from the interphase were washed with PBS containing 0.5 U/mL heparin and then resuspended to JID 1999;180 (September) a concentration of 1 3 10 6 –2 3 10 6 cells/mL PBS. This suspension contained ∼50%–60% T lymphocytes; the remaining cells were monocytes (20%–25%), NK cells (12%–15%), and B lymphocytes (∼5%). Cell viability was 195% (determined by trypan blue exclusion). z molecule expression assessed by fluorescence-activated cell sorter. PBMC were fixed with 0.5% formaldehyde for 20 min at 47C, washed in ice-cold PBS, and stored overnight at 47C. Expression of z molecules by T lymphocytes was measured by an indirect immunofluorescence assay and fluorescence-activated cell sorter (FACS) analysis, as described elsewhere [26] with minor modifications. In short, PBMC were resuspended at a concentration of 5 3 10 6 cells/mL PBS containing 1% bovine serum albumin (PBS-BSA) and 20 mg/mL digitonin (Sigma Chemical, St. Louis) and were incubated on ice for 10–15 min. After this treatment, 195% of the cells were permeable, as determined by trypan blue uptake. Next, the cells were incubated in 1% (vol/vol) normal goat serum for 5 min to block nonspecific binding sites, washed, and incubated with either MAb TIA-2, 6B10.2, or 63D3, an isotypematched irrelevant MAb. After 30 min of incubation on ice and 3 washes, the cells were incubated with GAMFITC in PBS containing 0.05% Tween 20 for 30 min on ice. Excess GAMFITC was removed by washing. Free F(ab0)2 sites of cell-bound GAMFITC were blocked by using 1% (vol/vol) normal mouse serum. Then the cells were stained for 30 min with anti-CD3PE, -CD4PE, or CD8PE. After a wash, the cells were subjected to flow cytometry (FACScan; Becton Dickinson). The lymphocyte population was gated by forward-sideward scatter characteristics. The relative expression of z molecules by CD31, CD41, and CD81 cells was calculated as a ratio of the median fluorescence intensity (MFI) of cells incubated with the TIA-2 or 6B10.2 MAb to that of cells incubated with the isotype-matched irrelevant antibody. Biochemical analysis of z molecule expression. After removal of the monocytes from the PBMC suspension by adhesion to plastic, the nonadherent cells were collected and resuspended to a concentration of 2 3 10 7 cells/mL buffer containing 1% Nonidet P-40, 0.01 M triethanolamine-HCl at pH 7.8, 0.15 M NaCl, 5 mM EDTA, 0.02 mg/mL soybean trypsin inhibitor, 1 mM phenylmethylsulfonyl fluoride, 0.02 mg/mL leupeptin, 20 mM iodoacetamide, and 0.1 U/mL aprotinine, and were maintained for 30 min at 47C. Next, nuclear debris were removed by centrifugation of the lysates for 30 min at 10,000 g. The proteins in the supernatants were separated by SDS-PAGE on a 12% gel under reducing conditions and were transferred to a 0.2-mm protran nitrocellulose membrane (Schleicher & Schuell, Dassel, Germany). The membrane was soaked in 5% low-fat milk to block nonspecific binding sites, and then incubated with 0.1 mg/mL MAb 6B10.2 directed against z molecules. MAb 6B10.2 was used in these experiments because of its suitability for immunoblotting, as stated by the manufacturer. Proteins were visualized with GAMPO and enhanced chemiluminescence (Amersham International, Amersham, UK). Band densities were measured with Image Quant software (Molecular Dynamics, Sunnyvale, CA). Assessment of z mRNA expression. After removal of the monocytes from the PBMC suspension by adhesion to plastic, total cellular RNA was isolated from the lymphocytes by use of Trizol B (Campro Scientific, Veenendaal, The Netherlands), followed by chloroform extraction, isopropanol precipitation, and resuspension JID 1999;180 (September) CD3z Expression Correlates with HIV Status 651 NaHCO3, 2 mM L-glutamine, 100 U/mL penicillin G, and 100 mg/ mL streptomycin for 20 h at 377C. Next, the cells were harvested, washed twice in PBS-BSA, and stained with anti-CD69FITC and anti-CD3PE for 30 min. After removal of excess antibodies by washing, the cells were fixed in 1% formaldehyde and subjected to flow cytometry. The relative expression of CD69 by CD31 cells was calculated as a ratio of the MFI of cells cultured with and without PHA. Statistical analysis. Results are presented as individual values or as mean 5 SD. The significance of differences in expression of z molecules and CD69 expression among cells from healthy controls, HIV-positive subjects, and AIDS patients was calculated by the Mann-Whitney U test; correlations between CD3z expression and peripheral CD41 T cell numbers, virus load, and CD69 expression were determined by Pearson’s correlation test. Results Expression of z molecules by T lymphocytes. The expression of z molecules by CD31 lymphocytes from AIDS patients was Figure 1. Expression of CD3z molecules by T lymphocytes from AIDS patients, human immunodeficiency virus (HIV)–positive asymptomatic or mildly symptomatic patients, and healthy controls. z expression was determined in permeabilized cells by use of monoclonal antibody (MAb) TIA-2, CD3PE counterstaining, and flow cytometry and was expressed as the ratio of median fluorescence intensity of cells incubated with TIA-2 MAb to that of cells incubated with isotypematched irrelevant MAb. of total cellular RNA in water. An initial round of reverse transcription by use of M-MLV reverse transcriptase (Gibco BRL, Breda, The Netherlands) provided cDNA targets for subsequent 27-cycle polymerase chain reaction (PCR) amplification. Pilot experiments demonstrated that these cycle numbers were within the logarithmic phase for CD3z (sense, 50-CCTCAGCCTCTGCCTCCCAGC-30; antisense, 50-CTCACTGTAGGCCTCCGCCA-30) [28] and GAPDH primers (sense, 50-CATCACCATCTTCCAGGAGC-30; antisense, 50-GGATGATGTTCTGGAGAGCC-30) [29] (Pharmacia Biotech, Roosendaal, The Netherlands). GAPDH was the housekeeping gene used as a control. PCR was done in duplicate. Amplification conditions included denaturation at 957C for 1 min, primer annealing at 557C for 1 min, and primer extension at 727C for 1 min in an automated thermal cycler by use of the DNA polymerase Taq (Perkin Elmer-Cetus, Emeryville, CA). PCR reaction mixtures were visualized on 2% agarose gels containing ethidium bromide. After densitometric analysis of the bands with Image Quant software, results were expressed relative to the GAPDH signal. To confirm the identity of the PCR products, after electrophoresis PCR reaction mixtures were transferred onto a Hybond-N nylon membrane (Amersham), hybridized with probes (z, 50-GCTCCTGCTGAACTTCACTCTC-30; GAPDH, 50-TCTCCATGGTGGTGAAGACG-30), and labeled by a 30-end-labeling technique with [32P]dATP (data not shown). Analysis of CD69 expression by cultured lymphocytes. PBMC were cultured in the presence or absence of 1 mg/mL PHA (Murex Diagnostics, Dartford, UK) at a concentration of 106 cells/mL Dulbecco’s MEM (Gibco BRL, Paisley, UK), supplemented with 10% heat-inactivated human serum, 3.5 mg/mL glucose, 3.7 mg/mL Figure 2. Correlation between expression of CD3z molecules and plasma human immunodeficiency virus type 1 (HIV-1) RNA levels (A) and CD41 lymphocyte counts (B). z expression was determined in permeabilized cells by use of monoclonal antibody (MAb) TIA-2, CD3PE counterstaining, and flow cytometry and expressed as the ratio of median fluorescence intensity of cells incubated with TIA-2 MAb to that of cells incubated with isotype-matched irrelevant MAb. 652 Geertsma et al. JID 1999;180 (September) from T lymphocytes were measured. Gel electrophoresis and immunoblotting revealed that z molecules were almost absent in T lymphocytes from 1 AIDS patient who had relatively high HIV-1 RNA levels and low CD41 T cell counts (figure 3). T lymphocytes from the second patient, who had relatively low HIV-1 RNA levels, expressed z molecules but in significantly Figure 3. Expression of CD3z molecules by T lymphocytes from AIDS patients detected by gel electrophoresis and immunoblotting. Peripheral blood lymphocytes from 2 AIDS patients and 2 healthy controls were lysed in parallel by use of Nonidet P-40. Proteins in lysates (3 3 105 cell equivalents) were separated by 12% SDS-PAGE under reducing conditions, transferred to nitrocellulose membranes, and immunoblotted with monoclonal antibody 6B10.2. Band densities were measured with Image Quant software (Molecular Dynamics, Sunnyvale, CA). AU, arbitrary units; ND, not determined. significantly decreased, compared with that by cells from HIVpositive patients and healthy donors (figure 1). Similar reductions (35% 5 12% and 42% 5 15%, respectively, n 5 5) were found in the expression of z molecules by T lymphocytes from AIDS patients by use of the MAb 6B10.2 that was generated against a peptide stretch localized outside the phosphorylation sites of z instead of MAb TIA-2, which has a lower reactivity to phosphorylated z molecules (P. J. Anderson, personal communication) [30]. Thus, we excluded the possibility that decreased amounts of CD3z molecules were detected by TIA-2 in cells from AIDS patients because of the phosphorylation status of the molecules. Comparison of the expression of CD3z molecules by T lymphocytes from HIV-infected patients with virus loads and CD41 cell counts revealed that z expression decreased with increasing HIV-1 RNA levels (figure 2A) and with decreasing numbers of peripheral CD41 T lymphocytes (figure 2B). Expression of CD3e did not differ between cells from healthy controls and patients; the MFIs were 1735 5 487, 2087 5 479, and 1714 5 454 arbitrary units for healthy donors, HIV-positive subjects, and AIDS patients, respectively. Together, these data show that expression of CD3z molecules, but not of CD3e, by T lymphocytes is decreased according to disease progression. Enhanced resistance to permeabilization by digitonin could account for the reduction in the level of z molecules detected with FACS analysis in cells from AIDS patients. To investigate this possibility, total amounts of z molecules in lysates prepared Figure 4. Expression of CD3z molecules by CD41 and CD81 cells from AIDS patients, compared with cells from human immunodeficiency virus (HIV)–positive asymptomatic or mildly symptomatic patients and healthy controls. z expression was determined in permeabilized cells by use of monoclonal antibody (MAb) TIA-2 counterstained with CD4PE and CD8PE, analyzed by flow cytometry, and expressed as the ratio of median fluorescence intensity of cells incubated with TIA-2 MAb to that of cells incubated with isotypematched irrelevant MAb. JID 1999;180 (September) CD3z Expression Correlates with HIV Status 653 Figure 5. Expression of z-specific mRNA in T lymphocytes from human immunodeficiency virus (HIV)–infected patients (p1–p5) and healthy controls (c1–c6). cDNA was reverse transcribed from mRNA and analyzed in duplicate for presence of CD3z and GAPDH message. After 27 polymerase chain reaction (PCR) cycles, reaction mixtures were electrophoresed on 2% agarose gel containing ethidium bromide. Band densities were measured with Image Quant software (Molecular Dynamics, Sunnyvale, CA) and results were expressed relative to GAPDH signal. Identity of PCR products was confirmed by Southern blotting (data not shown). Expression of CD3z protein was measured by flow cytometry (see figure 1 legend) and expressed as median fluorescence intensity (MFI) in arbitrary units. lower amounts than in cells from the healthy donor (figure 3). Thus, both FACS and Western blot analysis showed reduced expression of z molecules by cells from AIDS patients. T lymphocyte activation by specific antigens results in a decrease in the cellular content of CD3z molecules [31]. Decreased expression of CD3z molecules by T lymphocytes from AIDS patients, therefore, could result from antigenic stimulation due to previous opportunistic infections. To investigate this possibility, we assessed CD3z expression by T lymphocytes from HIV-negative persons with opportunistic infections frequently seen in AIDS patients. One person had a history of disseminated M. avium infection; the other was a kidney transplantation recipient with CMV infection. CD3z expression by T lymphocytes from both patients was comparable with that of cells from control donors (83%–90% of control levels). These results indicate that HIV itself, rather than the opportunistic infections resulting from HIV infection, most likely causes reduced expression of z molecules by T lymphocytes from AIDS patients. Expression of z molecules by CD41 and CD81 T cells. Detailed analysis of the expression of z molecules by the various subpopulations of T lymphocytes revealed a significant decreased expression of z molecules by CD41 lymphocytes from AIDS patients compared with cells from HIV-positive patients and healthy donors (figure 4A). Expression of z molecules by CD81 cells from AIDS patients was significantly lower than that from cells from healthy controls and lower, although not significantly (P 5 .06), than that from cells from HIV-positive patients (figure 4B). Overall, expression of z molecules was decreased in both CD41 and CD81 cells from AIDS patients. PCR analysis of z chain–specific mRNA. To learn whether the decreased expression of z molecules by T lymphocytes from AIDS patients is regulated at the transcriptional level, we assayed z-specific mRNA in these cells by use of reverse transcription and PCR amplification. The results showed that decreased expression of z molecules by T lymphocytes from AIDS patients is associated with decreased mRNA levels for this protein (figure 5A, 5B). As a control, T lymphocytes from 2 patients expressing z molecules at a slightly reduced level had minor (figure 5C) or no reductions (figure 5D) in z mRNA levels compared with that in cells from healthy controls. Expression of CD69 by T lymphocytes on stimulation with PHA. To investigate whether decreased expression of z molecules could be involved in the impairment of functional activities of T lymphocytes from HIV-infected patients as a functional readout, we determined the expression of the early activation antigen CD69 [32] upon stimulation of these cells with PHA. Only a minority of T lymphocytes from patients and healthy controls, 7.6% 5 2.2% and 8.8% 5 5.3%, respectively, expressed CD69 when cultured in the absence of a stimulus. When cultured in the presence of PHA, 150% of the cells expressed CD69: 58.4% 5 28.4% and 68.1% 5 12.4% of cells from patients and healthy controls, respectively. The intensity of PHA-induced CD69 expression by CD3 T lymphocytes from 654 Geertsma et al. JID 1999;180 (September) HIV-infected patients was significantly lower (P 5 .003) than that from cells from healthy donors (figure 6A). We found a good correlation (r 5 0.76, P 5 .007) between CD3z expression and PHA-mediated CD69 expression (figure 6B), indicating that for CD69 expression, z expression correlates with functional activities of T lymphocytes. Expression of CD3z molecules by T lymphocytes after highly active antiretroviral therapy. Since there was a relation between CD3z expression and virus load, as a pilot study, we examined whether highly active antiretroviral therapy (HAART); a combination of 3 antiviral drugs including at least 1 protease inhibitor) was accompanied by improved expression of CD3z molecules in 3 subjects. Shortly after initiation of HAART, HIV-1 RNA copies in plasma of all patients dropped to levels near the detection limit of the assay; this was accompanied by an increase in the expression of z molecules by CD31, CD41, and CD81 lymphocytes (figure 7). In 1 patient, virus loads decreased further to undetectable levels in the next months; this was associated with a further increase in the expression of z molecules (figure 7A). In the other 2 patients, within 1 month (figure 7B) and within 5 months (figure 7C) after the start of therapy, virus loads increased, which was associated with decreased expression of z molecules by their T lymphocytes. For comparison, variability in CD3z expression by T lymphocytes from 4 healthy controls (determined 23 or 33 during the same period) was ∼10%. Together, these data suggest that effective treatment of AIDS patients with HAART results in enhanced expression of z molecules by their T lymphocytes. Discussion In this study, we found that expression of z molecules is down-regulated in T lymphocytes from HIV-infected persons, in relationship to disease progression. Expression of z molecules by T lymphocytes from AIDS patients, but not from HIVpositive persons with mild or no symptoms, was reduced by >35%, as measured by flow cytometry and immunoblotting. The reduction in CD3z molecules was specific and not a generalized reduction in the expression of the CD3 complex, since we found no decrease in the expression of CD3e molecules. We are the first to demonstrate reduced levels of mRNA for z molecules in cells from AIDS patients, thereby extending the results of 2 studies that reported decreased expression of z molecules by T lymphocytes from HIV-infected subjects [33, 34]. On the basis of these findings, we suggest that defects in or upstream of transcription of z account for the reduced expression of this protein. Furthermore, we found a significant correlation between expression of CD3z molecules and CD41 cell counts and an inverse correlation between z expression and plasma HIV-1 RNA levels. It is of interest that impaired expression of CD3z molecules appeared to be reversible in AIDS patients after HAART. Altered expression of CD3z molecules Figure 6. Phytohemagglutinin (PHA)-induced expression of CD69 (A) by T lymphocytes from human immunodeficiency virus (HIV)–infected patients and healthy controls and correlation with CD3z molecules (B). Peripheral blood mononuclear cells from patients (v) and healthy controls (V) were cultured in presence and absence of 1 mg/mL PHA for 20 h, stained with anti-CD69FITC and antiCD3PE, and subjected to flow cytometry. Results are expressed as the ratio of median fluorescence intensity (MFI) of cells cultured with and without PHA. Expression of CD3z molecules was determined in freshly isolated cells by permeabilization, staining with monoclonal antibody (MAb) TIA-2, CD3PE counterstaining, and flow cytometry and expressed as the ratio of MFI of cells incubated with TIA-2 MAb to that of cells incubated with isotype-matched irrelevant MAb. thus correlates with disease progression in persons infected with HIV and is thereby concurrent with therapy success in these patients. Whether decreased expression of CD3z molecules can explain functional defects of T lymphocytes from AIDS patients [1–5] is not clear. We found a significant correlation between expression of CD3z molecules and expression of the early activation antigen CD69 by T lymphocytes upon stimulation with mitogens. Whether decreased expression of CD3z molecules underlies other functional defects of T lymphocytes from HIVinfected patients is beyond the focus of this study. However, others have reported that defective HIV-specific cytolytic ac- Figure 7. Reversibility of impairment in expression of CD3z molecules by T lymphocytes from 3 AIDS patients after highly active antiretroviral therapy (HAART). Patient 1 (A), who had no prior antiretroviral treatment, began with stavudine, lamivudine, and indinavir; patient 2 (B) was treated with zidovudine and lamivudine and then with ritonavir; patient 3 (C), who was previously treated with zidovudine and lamivudine, received stavudine, didanosine, ritanovir, and saquinavir. Plasma human immunodeficiency virus type 1 (HIV-1) RNA levels were determined by Amplicor HIV-1 test kit (detection limit, ∼400 copies/mL). CD41 cells/mL during month 1 of HAART rose from 273 to 307, 107 to 197, and 15 to 38 for patients 1–3, respectively. Expression of z molecules was determined, as described in legends of figures 1 and 4. CD3z expression by T lymphocytes from healthy controls during same period was 7.6 5 1.5 (n 5 17). 656 Geertsma et al. tivity by T lymphocytes from HIV-infected patients correlated with reduced expression of CD3z molecules by these cells [34]. Furthermore, loss of CD3z molecules may result in suppression of antigen-specific proliferation of T lymphocytes [35]. Together, decreased expression of CD3z molecules most likely contributes at least to some functional defects in T lymphocytes from AIDS patients. We did not find decreased expression of CD3z molecules by T lymphocytes from asymptomatic or mildly symptomatic HIV-infected persons, as reported elsewhere [33, 34], even when we used an antibody with a lower affinity for phosphorylated z molecules. The reason for this discrepancy is not clear. T lymphocytes from HIV-infected subjects at early stages of disease have altered early protein tyrosine phosphorylation and PTK levels associated with impaired proliferative responses [21, 22]. Our data suggest that such alterations and not a loss of CD3z molecules account for functional defects of T lymphocytes early in infection. A second question pertains to the mechanisms underlying the reduced expression of z molecules by T lymphocytes from AIDS patients. Since antigenic stimulation of T lymphocytes results in enhanced TCR turnover and reduced levels of z molecules [31], antigenic stimulation due to previous opportunistic infections could account for the reduced expression of CD3z molecules in AIDS patients. However, our observation that T lymphocytes from HIV-negative persons who had been exposed to opportunistic agents, such as CMV and M. avium, did not have reduced expression of CD3z molecules excludes this possibility. Another possibility is that HIV-derived proteins, such as gp120, gp41, tat, and nef, which diminish functional activity of T lymphocytes and alter lymphocyte signaling [6–8, 36–40], affect expression of z molecules by T lymphocytes. Preliminary investigations into this possibility revealed no effect of HIV gp120 on expression of z molecules by T cells from healthy donors (data not shown). Alternatively, reactive oxygen intermediates produced by macrophages may induce decreased expression of z molecules in T lymphocytes, as has been reported elsewhere, for tumor-infiltrating T lymphocytes [35, 41]. Of interest, the level of glutathione, the main intracellular defense against oxidative stress, is decreased in plasma and leukocytes of HIV-infected subjects [42], indicating that reactive oxygen intermediates could also be involved in down-regulation of CD3z molecules from AIDS patients. In analogy, we found reduced expression of CD3z molecules by T lymphocytes from synovial fluid of patients with rheumatoid arthritis [43], a disease also involving oxidant stress [44]. HIV-1 infection is characterized by a chronic state of immune activation [45] and substantial shifts in the composition of T lymphocyte subsets, including a preferential loss of memory CD41 T lymphocytes [3] and a relatively increased number of T lymphocytes with a Th2 profile in the circulation [46, 47]. The major goal of antiretroviral therapy, therefore, is not only to suppress viral replication but also to achieve some degree of JID 1999;180 (September) immune reconstitution. Indeed, substantial increments in the number of memory CD41 T lymphocytes, diminished expression of T lymphocyte activation markers (e.g., HLA-DR, CD38, and CD25), and significant improvements of antigenspecific responses by peripheral blood lymphocytes following HAART have been reported elsewhere [48, 49]. We studied too few patients for definitive conclusions in regard to up-regulation of z molecules by T lymphocytes after HAART. In future studies, measurement of CD3z expression in the various subsets of T lymphocytes may contribute to the understanding of restoration of immune competence in patients during HAART. Furthermore, since lymphatic tissues harbor large depots of viral RNA and many infected cells [50], we anticipate more severely reduced levels of z molecules in cells at these sites, compared with peripheral T lymphocytes. The reduction in expression of CD3z molecules by lymphatic T lymphocytes may be reversible with significant virus load reductions in lymphatic tissues during HAART [51]. If so, redistribution of memory T lymphocytes previously trapped in the lymph nodes upon antiretroviral therapy [52] could result in normalization of CD3z expression by peripheral T lymphocytes. Future experiments will focus on expression of CD3z molecules by T lymphocytes in lymphoid tissues from patients before and during HAART. Acknowledgments We thank P. Anderson, Department of Tumor Immunology, Dana Farber Institute, Boston, for providing TIA-2 to start our studies; E. Suchiman for technical assistance; F. Koning and M. M. Maurice, Departments of Immunohematology and Bloodbank and of Rheumatology, respectively, LUMC, for advice on the biochemical characterization of the expression of z molecules; P. J. van den Elsen and B. C. Godthelp, Department of Immunohematology and Bloodbank, LUMC, for advice on the assessment of z mRNA; and the patients and controls for study participation. References 1. Clerici M, Stocks NL, Zajac RA, et al. Detection of three distinct patterns of T helper cell dysfunction in asymptomatic, human immunodeficiency virus–seropositive patients. J Clin Invest 1989; 84:1892–9. 2. Shearer GM, Bernstein DC, Tung KSK, et al. A model for the selective loss of major histocompatibility complex self-restricted T cell immune responses during the development of acquired immune deficiency syndrome (AIDS). J Immunol 1986; 137:2514–21. 3. Van Noesel CJM, Gruters RA, Terpstra FG, Schellekens PTA, Van Lier RAW, Miedema F. Functional and fenotypic evidence for a selective loss of memory T cells in asymptomatic human immunodeficiency virus–infected men. J Clin Invest 1990; 86:293–9. 4. Schnittman SM, Lane HC, Greenhouse J, Justement JS, Baseler M, Fauci AS. Preferential infection of CD41 memory T cells by human immunodeficiency virus type 1: evidence for a role in the selective T-cell functional defects observed in infected individuals. Proc Natl Acad Sci USA 1990; 87:6058–62. 5. Meyaard L, Otto SA, Hooibrink B, Miedema F. Quantitative analysis of JID 1999;180 (September) 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. CD3z Expression Correlates with HIV Status CD41 T cell function in the course of human immunodeficiency virus infection: gradual decline of both naive and memory alloreactive cells. J Clin Invest 1994; 94:1947–52. Cefai D, Ferrer M, Serpente N, et al. Internalization of HIV glycoprotein gp120 is associated with down-modulation of membrane CD4 and p56lck together with impairment of T cell activation. J Immunol 1992; 149: 285–94. Morio T, Chatila T, Geha RS. HIV glycoprotein gp120 inhibits TCR-CD3mediated activation of fyn and lck. Int Immunol 1997; 9:53–64. Ruegg CL, Strand M. A synthetic peptide with sequence identity to the transmembrane protein gp41 of HIV-1 inhibits distinct lymphocyte activation pathways dependent on protein kinase C and intracellular calcium influx. Cell Immunol 1991; 137:1–13. Danielian S, Alcover A, Polissard L, et al. Both T cell receptor (TcR)-CD3 complex and CD2 increase the tyrosine kinase activity of p56lck, CD2 can mediate TcR-CD3-independent CD45-dependent activation of p56lck. Eur J Immunol 1992; 22:2915–21. Tsygankov AY, Broker BM, Fargnoli J, Ledbetter JA, Bolen JB. Activation of tyrosine kinase p60fyn following T cell antigen receptor cross-linking. J Biol Chem 1992; 267:18259–62. Reth M. Antigen receptor tail clue. Nature 1989; 338:383–4. Chan AC, Irving BA, Fraser JD, Weiss A. The z chain is associated with a tyrosine kinase and upon T-cell antigen receptor stimulation associates with ZAP-70, a 70-kDa tyrosine phosphoprotein. Proc Natl Acad Sci USA 1991; 88:9166–70. Chan AC, Iwashima M, Turck CW, Weiss A. ZAP-70: a 70 kd protein tyrosine kinase that associates with the TCR z chain. Cell 1992; 71:649–62. Iwashima M, Irving BA, Van Oers NSC, Chan AC, Weiss A. Sequential interactions of the TCR with two distinct cytoplasmic tyrosine kinases. Science 1994; 263:1136–9. Weiss A, Koretzky G, Schatzman RC, Kadlecek T. Functional activation of the T cell antigen receptor induces tyrosine phosphorylation of phospholipase Cg1. Proc Natl Acad Sci USA 1991; 88:5484–8. Park DJ, Rho HW, Rhee SG. CD3 stimulation causes phosphorylation of phospholipase Cg1 on serine and tyrosine residues in a human T cell line. Proc Natl Acad Sci USA 1991; 88:5453–6. Secrist JP, Karnitz L, Abraham RT. T cell antigen receptor ligation induces tyrosine phosphorylation of phospholipase Cg1. J Biol Chem 1991; 266: 12135–9. Nishibe S, Wahl MI, Hernandez-Sotomayor SM, Tonk NK, Rhee SG, Carpenter G. Increase of the catalytic activity of phospholipase Cg1 by tyrosine phosphorylation. Science 1990; 250:1253–6. Berridge MJ, Irvine RF. Inositol trisphosphate, a novel second messenger in cellular signal transduction. Nature 1984; 312:315–21. Imboden JB, Stobo JD. Transmembrane signaling by the T cell antigen receptor: perturbation of the T3-antigen receptor complex generates inositol phosphates and releases calcium ions from intracellular stores. J Exp Med 1985; 161:446–56. Cayota A, Vuillier F, Siciliano J, Dighiero G. Defective protein tyrosine phosphorylation and altered levels of p59fyn and p56lck in CD4 T cells from HIV-1 infected patients. Int Immunol 1994; 6:611–21. Phipps DJ, Yousefi S, Branch DR. Increased enzymatic activity of the T cell antigen receptor–associated fyn protein tyrosine kinase in asymptomatic patients infected with the human immunodeficiency virus. Blood 1997; 90:3603–12. Finke JH, Zea AH, Stanley J, et al. Loss of T-cell receptor z chain in T-cells infiltrating human renal cell carcinoma. Cancer Res 1993; 53:5613–6. Nakagomi H, Petersson M, Magnusson I, et al. Decreased expression of the signal-transducing z chains in tumor-infiltrating T cells and NK cells of patients with colorectal carcinoma. Cancer Res 1993; 53:5610–2. Matsuda M, Petersson M, Lenkei R, et al. Alterations in the signaltransducing molecules of T cells and NK cells in colorectal tumor-infiltrating, gut mucosal and peripheral lymphocytes: correlation with the stage of the disease. Int J Cancer 1995; 61:765–72. 657 26. Anderson P, Blue ML, O’Brien C, Schlossman SF. Monoclonal antibodies reactive with the T cell receptor z chain: production and characterization using a new method. J Immunol 1989; 143:1899–904. 27. Centers for Disease Control. Revision of the CDC surveillance case-definition for acquired immunodeficiency syndrom. MMWR Morb Mortal Wkly Rep 1987; 36 (Suppl):1S–15S. 28. Weissman AM, Hou D, Orloff DG, et al. Molecular cloning and chromosomal localization of the human T-cell receptor z chain: distinction from the molecular CD3 complex. Proc Natl Acad Sci USA 1988; 85:9709–13. 29. Allen RW, Trach KA, Hoch JA. Identification of the 37 kDa protein displaying a variable interaction with the erythroid cell membrane as glyceraldehyde-3-phosphate dehydrogenase. J Biol Chem 1987; 262:649–63. 30. Boussiotis VA, Barber DL, Lee BJ, Gribben JG, Freeman GJ, Nadler LM. Differential association of protein tyrosine kinases with the T cell receptor is linked to the induction of anergy and its prevention by B7 familymediated costimulation. J Exp Med 1996; 184:365–79. 31. Valitutti S, Müller S, Salio M, Lanzavecchia M. Degradation of T cell receptor (TCR)–CD3-z complexes after antigenic stimulation. J Exp Med 1997; 185:1859–64. 32. Testi R, D’Ambrosio D, De Maria R, Santoni A. The CD69 receptor: a multipurpose cell-surface trigger for hematopoietic cells. Immunol Today 1994; 15:479–83. 33. Štefanová I, Saville MW, Peters C, et al. HIV-infection–induced posttranslational modification of T cell signaling molecules associated with disease progression. J Clin Invest 1996; 98:1290–7. 34. Trimble LA, Lieberman J. Circulating CD4 T lymphocytes in human immunodeficiency virus–infected individuals have impaired function and downmodulate CD3z, the signaling chain of the T-cell receptor complex. Blood 1998; 91:585–94. 35. Otsuji M, Kimura Y, Aoe T, Okamoto Y, Saito T. Oxidative stress by tumorderived macrophages suppresses the expression of CD3z chain of T-cell receptor complex and antigen-specific T-cell responses. Proc Natl Acad Sci USA 1996; 93:13119–24. 36. De SK, Marsh JW. HIV-1 nef inhibits a common pathway in NIH-3T3 cells. J Biol Chem 1994; 269:6656–60. 37. Iafrate AJ, Bronson S, Skowronski J. Separable functions of nef disrupt two aspects of T cell receptor machinery: CD4 expression and CD3 signaling. EMBO J 1997; 16:673–84. 38. Chirmule N, Than S, Khan SA, Pahwa S. Human immunodeficiency virus that induces functional unresponsiveness in T cells. J Virol 1995; 69:492–8. 39. Li CJ, Friedman DJ, Wang C, Metelev V, Pardee AB. Induction of apoptosis in uninfected lymphocytes by HIV-1 tat protein. Science 1995; 268:429–31. 40. Ott M, Emiliani S, Van Lint S, et al. Immune hyperactivation of HIV-1– infected T cells mediated by tat and the CD28 pathway. Science 1997; 275:1481–5. 41. Kono K, Salazar-Onfray F, Petersson M, et al. Hydrogen peroxide secreted by tumor-derived macrophages down-modulates signal transducing zeta molecules and inhibits tumor-specific T cell– and natural killer cell–mediated cytotoxicity. Eur J Immunol 1996; 26:1308–13. 42. Staal FJT, Ela SW, Roederer M, Anderson MT, Herzenberg LA. Glutathionedeficiency and human immunodeficiency virus infection. Lancet 1992; 339: 909–12. 43. Maurice MM, Lankester AC, Bezemer AC, et al. Defective TCR-mediated signaling in synovial T cells in rheumatoid arthritis. J Immunol 1998; 159: 2973–8. 44. Maurice MM, Nakamura H, Van der Voort EAM, et al. Evidence for the role of an altered redox state in hyporesponsiveness of synovial T cells in rheumatoid arthritis. J Immunol 1997; 158:1458–65. 45. Fauci AS. Host factors and the pathogenesis of HIV-induced disease. Nature 1996; 384:529–34. 46. Clerici M, Hakim FT, Venzon DJ, et al. Changes in interleukin-2 and interleukin-4 production in asymptomatic, human immunodeficiency virus–seropositive individuals. J Clin Invest 1993; 91:759–65. 47. Meyaard L, Otto SA, Keet IPM, Van Lier RAW, Miedema F. Changes in 658 Geertsma et al. cytokine secretion patterns of CD41 T cell clones in HIV infection. Blood 1994; 84:4262–8. 48. Autran B, Carcelain G, Li TS, et al. Positive effects on CD4 1 T cell homeostasis and function in advanced HIV disease. Science 1997; 277:112–6. 49. Li TS, Tubiana R, Katlama C, et al. Long-lasting recovery in CD4 T-cell function and viral load reduction after highly active antiretroviral therapy in advanced HIV-1 disease. Lancet 1998; 351:1682–6. 50. Pantaleo G, Graziosi C, Demarest JF, et al. HIV infection is active in lym- JID 1999;180 (September) phoid tissue during the clinically latent stage of disease. Nature 1993; 362: 355–8. 51. Cavert W, Notermans DW, Staskus KA, et al. Kinetics of response in lymphoid tissues to antiretroviral therapy of HIV-1 infection. Science 1997; 276:960–4. 52. Pakker NG, Notermans DW, De Boer RJ, et al. Biphasic kinetics of peripheral blood T cells after triple combination therapy in HIV-1 infection: a composite of redistribution and proliferation. Nature Med 1998; 4: 208–14.