Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
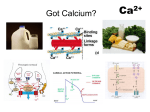
At the end of this lecture, students should be able to: • • • • • • Describe the role of calcium in the body Enumerate the hormones affecting plasma calcium Describe the actions of parathyroid hormone Know the source and actions of calcitonin Describe the role of calcitriol Describe Pathophysiology of hypoparathyroidism & hyperparathyroidism • Calcium in plasma or serum exists in three forms: 1) Protein-bound calcium accounts for approximately onethird of the total serum calcium concentration. Proteinbound calcium cannot diffuse through membranes and thus is not usable by tissues. 2) Ionized or free calcium is the physiologically active form that accounts for 50%–60% of total calcium concentration. 3) Complexed or chelated calcium is bound to phosphate, bicarbonate, sulfate, citrate, and lactate and accounts for ~10% of the total calcium concentration. Total Body Ca++ Body fluids (1%) ECF (0.1%) Free form (50%) Skeleton & teeth (99%) ICF in soft tissues (0.9%) Bound (50%) Functions of calcium: 1) The calcium ion is an essential structural component of the skeleton 2) It plays a key role in muscle Contraction, blood Coagulation, Enzyme activity, neural Excitability, secondary Messengers, hormone release, and Membrane permeability. Plasma calcium level: • Normally kept constant within a range of 9 to 11 mg/100 ml. • 50 % exists as free calcium. * The principal regulatory hormones: A- Parathyroid hormone (PTH). B- Calcitriol or (1, 25-(OH)2- cholecalciferol). C- Calcitonin. • Others: Adrenal corticosteroids, estrogens, thyroxine, and somatotropin may also contribute to the maintenance of calcium homeostasis. • Parathyroid glands are essential for life. They secrete Parathyrin or Parathyroid hormone (PTH) (84 a.a.) by chief cells. • Four rice grain-sized glands located on the back surface of the thyroid gland, one in each corner. • Ca2+ sensors in cells of the parathyroid glands regulate PTH synthesis and secretion in response to changes in the plasma concentration of ionized Ca2+ . • More PTH is secreted into the blood stream whenever Ca2+ concentration falls below normal (hypocalcemia). • Inversely, PTH secretion decreases when Ca2+ level rises. • The primary function of PTH is to normalize the decreased Ca2+ conc. in the blood. It is a Ca2+ increasing hormone. • It is essential for life. Complete absence of PTH ensues death within few days. • PTH essentially acts to increase the concentration of calcium in the blood by acting upon the parathyroid hormone 1 receptor, which is present at high levels in bone and kidney, and the parathyroid hormone 2 receptor, which is present at high levels in the central nervous system, pancreas, testis, and placenta. Calcium regulation: • Maintenance of plasma Ca++ level at 10 mg %, and also phosphate level to keep solubility product = [Ca++] X [PO4-3] = constant. A) On bone: • PTH raises plasma Ca2+ by withdrawing Ca2+ from the bone bank. • induces a fast Ca2+ efflux into the plasma from the small labile pool of Ca2+ in the bone fluid. • Second, by stimulating bone dissolution, it promotes a slow transfer into the plasma of both Ca2+ & PO43- from the stable pool of bone minerals in bone itself. • Bone resorption is the normal destruction of bone by osteoclasts, which are indirectly stimulated by PTH. • Osteoclasts do not have receptors for PTH. • PTH binds to osteoblasts to increase their expression of RANKL and inhibits their expression of OPG. • The binding of RANKL to RANK stimulates these osteoclast precursors to fuse, forming new osteoclasts, which ultimately enhances bone resorption. PTH Calcitriol Estrogen Calcitonin • reabsorption of Calcium in DCT & CD of nephrons plasma Ca++ level. • reabsorption of Phosphate in PCT of nephrons plasma Phosphate level. • When the (calcium : phosphate ratio) increases, more calcium is free in the circulation. • PTH accelerates the final step of calcitriol synthesis in the kidney, resulting in increased absorption of Ca++ from the GIT. • It enhances the absorption of calcium in the intestine by increasing the production of activated vitamin D. • PTH increases the activity of 1-α-hydroxylase enzyme, which converts 25-hydroxycholecalciferol, the major circulating form of inactive vitamin D, into 1,25dihydroxycholecalciferol (Calcitriol), the active form of vitamin D, in the kidney. • This activated form of vitamin D (Calcitriol) increases the absorption of Ca2+ ions by the intestine via calbindin. • It is not under control of hypothalamus nor anterior pituitary. • It is controlled by Plasma Ca++ Level (and to a lesser extent magnesium) by – ve feedback mechanism. i.e. plasma Ca++ PTH secretion. • It is a 32-amino acid linear polypeptide hormone produced in humans primarily by parafollicular C-cells of the thyroid. • Calcitonin counteracts parathyroid hormone. Calcitonin reduces calcium levels in the blood by two main mechanisms: 1. Inhibits osteoclast activity in bones. Therefore, the inhibition of osteoclasts by calcitonin directly reduces the amount of calcium released into the blood. 2. Inhibits renal tubular cells reabsorption of Ca2+ allowing it to be excreted in the urine. • The actions of PTH and calcitonin are antagonistic on bone resorption but synergistic on decreasing the renal tubular reabsorption of phosphorus. • Calcitonin protects against calcium loss from skeleton during periods of calcium mobilization, such as pregnancy and lactation. Calcitonin prevents postprandial hypercalcemia resulting from absorption of Ca2+ . • Salmon calcitonin is used for treatment of: Postmenopausal osteoporosis, Hypercalcaemia & Paget's disease. • A steroid like compound essential for Ca++ absorption in the intestine. Activated by the addition of two (-OH) groups. • The first reaction occurs in the liver & the second in kidneys. • It is the active metabolite of vitamin D3 • PTH accelerates the final step of calcitriol synthesis in the kidney. Its release from kidney is increased by decreased plasma Ca++. Calcitriol increases blood calcium levels by: 1) increasing absorption of dietary calcium from the gastrointestinal tract 2) increasing renal tubular reabsorption of calcium, thus reducing the loss of calcium in the urine. Calcitriol also stimulates release of calcium from bone by its action on the specific type of bone cells referred to as osteoblasts, causing them to release RANKL, which in turn activates osteoclasts. The observation that calcitriol stimulates the release of calcium from bone seems contradictory, given that sufficient levels of serum calcitriol generally prevent overall loss of calcium from bone. It is believed that the increased levels of serum calcium resulting from calcitriol-stimulated intestinal uptake causes bone to take up more calcium than it loses by hormonal stimulation of osteoclasts. Only when there are conditions, such as dietary calcium deficiency or defects in intestinal transport, which result in a reduction of serum calcium does an overall loss of calcium from bone occur. • Causes: 1. Adenoma of parathyroid gland (in 80% of cases). 2. Multiple adenomas or hyperplasia (in 15% of cases). 3. Carcinoma (in less than 5% of cases). • Characterized by hypercalcemia & hypophosphatemia. • Clinical features: Bones Stones Abdominal groans Psychic moans p. 730 • Causes: 1. Accidental removal of parathyroids surgically with thyroid in cases of thyroid carcinoma. 2. Autoimmune disease. • Characterized by hyperphosphatemia. • Clinical picture: hypocalcemia & Hypocalcaemia neuromuscular hyperexcitability Tetany. • Def. ↓ ionized Ca++ in ECF → ↑ Na+ influx → ↑ Neuromuscular excitability. • Causes: 1. Hypoparathyroidiam hypocalcaemia. 2. Alkalemia as in Hyperventilation & Vomiting. 3. ↓ Absorption of Ca++ from GIT due to: Low calcium intake Lack of vitamin D. 1) Manifest tetany: Plasma Ca++ level is below 7 mg% Hypocalcaemia manifest itself by cramps of the limbs in form of: • Carpal Spasm: (Obstetrician's hand) flexion at elbow, wrist, metacarpophalangeal joints & extension at interphalangeal joints and adduction of thumb. • Pedal Spasm: Dorsiflexion of foot and planter flexion of toes. • Laryngeal spasm: Asphyxia (fatal). • Plasma Ca++ level is above 7 mg% and below 9 mg%. • Appears after exposure to stress, pregnancy, lactation & hyperventilation ... • Diagnosis of latent tetany: 1) Plasma Ca++ level. 2) Trousseau's sign: blood flow in arm with a sphygmomanometer cuff carpal spasm in less than 3 minutes (pressure must be more than systolic pressure). 3) Chvostek's sign: Sharp tap on facial nerve at angle of mandible twitch of facial muscles. • During attack: Calcium gluconate by very slow intravenous injection. • For latent tetany: Vitamin D & Oral calcium. قلعة صالح الدين األيوبى ....القاهرة