Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
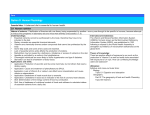
FV 4 2008 prelom.xp:FV 2 2007 prelom zadnji.xp 10/10/08 3:35 PM Page 167 Can supplementation with vitamin E or C and omega-3 or -6 fatty acids improve ... Can supplementation with vitamin E or C and omega-3 or -6 fatty acids improve the outcome of schizophrenia? Ali lahko vitaminom E ali C in omega-3 ali -6 maøœobne kisline izboljøajo izide zdravljenja shizofrenije? Marija Boøkoviå, Tomaæ Vovk Abstract: Background: Schizophrenia is a major mental disorder associated with high morbidity and economic cost. It is important to develop alternative or supplementary treatment strategies that could augment antipsychotic actions and reduce side effects. Increasing evidence indicate that oxidative damage is present in patients with schizophrenia. Oxidative mediated damage is suggested by an increase in lipid peroxidation products in cerebrospinal fluid and plasma, and a reduced concentration of membrane polyunsaturated fatty acids in neurons. Lipid peroxidation can be prevented by antioxidant supplementation and on the other hand the process of phospholipids regeneration can be increased by supplementation with essentially fatty acids. Objective: To review available data on the clinical effects of vitamin E or C and omega-3 or -6 fatty acids for supplementary treatment of patients with schizophrenia. Main results: Trials on a limited number of subjects with an uncertain quality of randomisation indicate that vitamin E protects against deterioration of tardive dyskinesia but there is no evidence that vitamin E supplementation improves symptoms of tardive dyskinesia. As concerns vitamin C, there is not enough data for evaluation. Until now, the results show that oral supplementation with vitamin C restore ascorbic acid levels, reduce oxidative stress, and improve Brief Psychiatric Rating Scale score. The results of supplementation therapy with polyunsaturated fatty acids remain inconclusive. Omega-3 fatty acids have the greatest potential of all fatty acids to reduce movement disorder outcomes as expressed by the Abnormal Involuntary Syndrome Scale score. Combined therapy with antioxidants and polyunsaturated fatty acids is the most promising approach to prevent oxidative damage and enable regeneration of phospholipids in neurons, but its potential has to be confirmed in future clinical studies. Conclusion: The use of antioxidants and omega3 polyunsaturated fatty acids in adjuvant treatment of schizophrenia still remains hypothetical and there is a need for large, well designed and reported studies. Potentially it could be an effective, low cost, supplementary treatment with few side effects. Therefore, such therapy would be a significant advance in schizophrenia. Key words: schizophrenia, oxidative stress, vitamin E, vitamin C, omega-3 and -6 fatty acids Povzetek: Uvod: Shizofrenija je pomembna duøevna bolezen povezana z velikim deleæem obolevnosti in ekonomskimi stroøki. Prav zato je potrebno razviti alternativne ali adjuvantne terapije, ki bi sedanjo antipsihotiœno terapijo izboljøale predvsem pa omilile njene neæelene uœinke. Øtevilni dokazi potrjujejo oksidativne poøkodbe pri bolnikih s shizofrenijo. To so poveœane koncentracije produktov lipidne peroksidacije v cerebrospinalni tekoœini in plazmi ter zniæane koncentracije polinenasiœenih maøœobnih kislin v membranah nevronov. Lipidno peroksidacijo lahko prepreœimo s terapijo z antioksidanti, medtem ko lahko procese regeneracije fosfolipidov pospeøimo z uvedbo terapije z esencialnimi maøœobnimi kislinami. Namen: Pregled rezultatov kliniœnih øtudij, kjer so bolniki s shizofrenijo prejemali adjuvantno terapijo z vitamino E ali C in omega3 ali -6 maøœobnimi kislinami. Rezultati: Øtudije z majhnim øtevilom bolnikov s shizofrenijo in z dvomljivo randomizacijo so pokazale, da vitamin E prepreœuje napredovanje tardivne diskinezije, vendar pa ne omogoœa tudi izboljøanje njenih simptomov. Øtudij z adjuvantno terapijo z vitaminom C je premalo. Dosedanji rezultati kaæejo, da peroralna aplikacija vitamina C poveœa zniæane koncentracije vitamina C, zmanjøa oksidativni stres in izboljøa psihiatriœno stanje ovrednoteno po kratki psihiatriœni ocenjevalni lestvici. Rezultati adjuvantne terapije s polinenasiœenimi maøœobnimi kislinami ostajajo nejasni. Omega-3 maøœobne kisline so najbolj obetajoœe maøœobne kisline, ki lahko izboljøajo motnje gibanja ocenjene z lestvico abnormalnih nehotnih gibov. Potencialno najuspeønejøo adjuvantno terapijo za prepreœevanje oksidativnih poøkodb in regeneracijo fosfolipidov v neuronih predstavlja kombinacija maøœobnih kislin in antioksidantov, vendar je tudi to potrebno øe potrditi v kliniœnih raziskavah. Zakljuœek: Uporaba antioksidantov in omega-3 polinenasiœenih maøœobnih kislin za adjuvantno zdravljenje shizofrenije ostaja øe vedno na raziskovalni ravni, zato je potrebno izvesti velike, dobro naœrtovane in dokumentirane øtudije. Ta kombinacija adjuvantne terapije bi lahko bila uspeøna, z malo neæelenimi uœinki in nizko ceno zato lahko predstavlja pomemben napredek pri zdravljenju shizofrenije. Kljuœne besede: shizofrenija, oksidativen stres, vitamin E, vitamin C, omega-3 in -6 maøœobne kisline Marija Boøkoviå, M. Pharm., Faculty of Pharmacy, The Chair of Biopharmaceutics and Pharmacokinetics, Aøkerœeva 7, 1000 Ljubljana, Slovenia dr. Tomaæ Vovk, M. Pharm., Faculty of Pharmacy, The Chair of Biopharmaceutics and Pharmacokinetics, Aøkerœeva 7, 1000 Ljubljana, Slovenia farm vestn 2008; 59 167 FV 4 2008 prelom.xp:FV 2 2007 prelom zadnji.xp 10/10/08 3:35 PM Page 168 Pregledni znanstveni œlanki - Review Scientific Articles Introduction Schizophrenia is a major mental disorder associated with high morbidity and economic cost. The illness has a poor outcome in spite of the best currently available treatment. It is the most common cause of chronic psychosis and affects approximately 1 % of the world's population. Its cardinal signs include active psychosis, such as delusions and hallucinations, the disturbance of logical thought processes, and deterioration of social and occupational functions. Two terms are commonly used to categorize the symptoms of schizophrenia. Positive symptoms refer to new mental phenomena, which unaffected people normally do not experience, such as hallucinations and delusions. Negative symptoms refer to a loss of normal mental functions leading for example to amotivation and social withdrawal. More recently, impaired cognition has been identified as a third domain of abnormality in schizophrenia (1). Schizophrenia is associated with a broad range of neurodevelopmental, structural and behavioral abnormalities that often progress with or without treatment. Evidence indicates that such neurodevelopmental abnormalities may result from defective genes and/or non-genetic factors such as prenatal and neonatal infections, birth complications, famines, maternal malnutrition, drug and alcohol abuse, season of birth, sex, birth order and life style (2, 3). According to the classical dopamine (DA) hypothesis, schizophrenia is associated with increased dopaminergic activity in the specific brain structures. Increased dopaminergic activity is supported by increased number and sensitivity of dopaminergic D2 receptors and overproduction or reduced destruction of dopamine (4). The scope of this article is to review major mechanisms of oxidative stress development in patients with schizophrenia and in particular to review potential therapeutic strategies using supplementation with vitamin E and C and omega-3 and -6 polyunsaturated fatty acids to prevent oxidative injuries and improve clinical outcome of schizophrenia. Oxidative stress Increasing evidence indicates that oxidative damage exists in schizophrenia. Although this may not be the main cause, oxidative damage has been suggested to contribute to its pathophysiology and may account for the deteriorating course and poor outcome in schizophrenia (9, 10). Under physiological conditions, dopamine (DA) which has a dihydroquinone structure, is non-enzymatically oxidized by molecular oxygen to form hydrogen peroxide (H2O2) and the corresponding oquinone. Subsequently, o-quinone undergoes an intramolecular cyclization which is immediately followed by a cascade of oxidative reactions resulting in the final formation of a black, insoluble polymeric pigment known as neuromelanin. During the oxidation of dopamine and its precursor L-DOPA, the superoxide radical (O2•-) and H2O2 can be produced. For these compounds, the rate of oxidation is accelerated by the presence of transition-metal ions such as iron and copper. In the presence of such metals, in addition to O2•-, H2O2, semiquinones, and quinones, the hydroxyl radical (OH•) is produced during oxidation. The molecular mechanism generally accepted for OH• production during DA autoxidation is the following: Antipsychotics have been used to treat schizophrenia for over 50 years. Classical antipsychotic agents such as haloperidol, fluphenazine, levomepromazine, promazine and others are potent antagonists of dopamine receptors, mainly D2. Atypical antipsychotics like clozapine, risperidone, olanzapine, quetiapine and others have a higher affinity for other receptors, such as serotonin receptors (5-HTA2). It also seems that they have therapeutic effects against negative symptoms and cognitive deficits that are considered to be difficult to treat (1). Classical and atypical antipsychotics differ in their neurotransmitter receptor affinity profiles but also in their efficacy and side effects in patients with schizophrenia. Classical antipsychotics have extrapyramidal side effects such as tardive dyskinesia which is a movement disorder and is characterised by abnormal, repetitive and involuntary movements. It has also been found that they increase oxidative cellular stress more than atypical antipsychotics. According to literature data, administration of classical antypsychotics induces oxidative stress and provokes attenuation of antioxidant enzymes and cell oxidative damage. Few authors have conducted experiments with classical and atypical antipsychotics. They came to unique conclusion, that after a classical antipsychotic administration concentration of antioxidant enzymes is lower and concentration of lipid peroxidation marker, malondialdehyde, is significantly higher. Therefore, it has been proposed, that oxidative damage is one of the mechanisms of classical antipsyhotics toxicity. Furthermore, it has been suggested, that neuronal cell damage caused by reactive species (RS) is a pathophysiological explanation for formation of neuroleptic induced tardive dyskinesia. (5, 6, 7, 8). 168 farm vestn 2008; 59 which involves an initial production of the O2•-, from which H2O2 is formed, to finally give OH• through the Fenton reaction. Additionally, this process involves the formation of o-quinone from the corresponding semiquinone radical (11, 12, 13). FV 4 2008 prelom.xp:FV 2 2007 prelom zadnji.xp 10/10/08 3:35 PM Page 169 Can supplementation with vitamin E or C and omega-3 or -6 fatty acids improve ... Oxidative deamination of dopamine by monoamine oxidase (MAO) can lead to formation of H2O2 and 3,4-dihydroxyphenylacetaldehyde. The latter compound is then oxidized by aldehyde dehydrogenase to give 3,4-dihydroxyphenylacetic acid, which subsequently is methylated by catechol-O-methyltransferase to form homovanillic acid (14, 15). Therefore, both the autoxidation and the MAO-mediated metabolism of DA involve the formation of H2O2, a compound that can easily be reduced in the presence of ferrous ion to form, through the Fenton reaction, the OH• radical, which is considered the most damaging free radical for living cells. Important iron-containing proteins in the brain include cytochromes, ferritin, aconitases, mitochondrial nonhaem-iron proteins, cytochromes P450 and the tyrosine and tryptophan hydroxylase enzymes, which catalyse the first steps in the synthesis of dopamine and serotonin. In the dopaminergic neurons neuromelanine is also present, which has a reported ability to accumulate iron and consequently may act by promoting the Fenton reaction (16, 17, 18). As iron content in the brain is high, dopamine autoxidation is accelerated and therefore probably responsible for the majority of ROS production (12). Schizophrenia is characterised by increased amounts of DA. Both untreated and treated patients have an increased possibility of oxidative cell damage, but in patients treated with classical antipsychotics oxidative damage is more expressed. Since classical antipsyhotics block DA receptors, DA remains unbound in the synapses. Therefore, large amounts of DA are available for processes of biotransformation. Consequently, it has been proposed that haloperidol-induced oxidative stress arises from the increased production of hydrogen peroxide caused by the catecholamine metabolism with monoamine oxidase and autooxidation of dopamine. Again, we can speculate that iron accelerates dopamine autooxidation which therefore mainly contributes to RS production. Another possible source of reactive species in haloperidol toxicity is the electron transport chain of mitochondria which is blocked by haloperidol (17). Consequences of oxidative stress Oxidative stress is defined as a disturbance in the prooxidantantioxidant balance in favour of the former, leading to potential damage. This means that diminished antioxidants and/or increased production of reactive species will result in oxidative damage. Oxidative damage is the biomolecular damage caused by attack of reactive species upon the constituents of living organisms (11). Reactive species can damage lipids, proteins, enzymes, carbohydrates and DNA in cells, resulting in membrane damage, fragmentation or random cross-linking of molecules like DNA, enzymes and structural proteins, and even lead to cell death induced by DNA fragmentation and lipid peroxidation. In the neuronal cells and glia the consequences are increased lipid peroxidation, oxidative damage to DNA, damage to proteins and induction of apoptosis and necrosis (11). Since many studies have confirmed increased lipid peroxidation in patients with schizophrenia, lipids probably represent the main target among cell macromolecules for oxidative damage. Phospholipids, cholesterols, saturated fatty acids and monounsaturated fatty acids can be synthesized de novo within the human body. Because mammals cannot introduce a double bond beyond the delta-9 position in the fatty acid chain, omega-6 and omega-3 must be regained through the diet. Polyunsaturated fatty acids are major components of membrane phospholipids and are highly susceptible to reaction with free radicals, with the resultant formation of peroxy radicals and lipid peroxides. These products in the cell membrane result in an unstable membrane structure, and altered membrane fluidity and permeability. Many investigators reported decreased levels of essential fatty acids (EFA) in both the peripheral and central membranes of patients with schizophrenia (5, 19). For a long time, altered membrane phospholipid metabolism has been considered as the pathophysiological basis of schizophrenia. Several studies have reported variable changes in the levels of membrane phospholipids in erythrocytes and cultured skin fibroblasts. Alternation of the phospholipid metabolism is also reflected in the decrease of phosphomonoesters, indicating reduced synthesis, and the increase of phosphodiesters, indicating increased breakdown. Recent attention has been focused on abnormal essential polyunsaturated fatty acid metabolism. This seems quite appropriate since the dietary availability of essential fatty acids and their utilization in synthesis of phospholipids determines the quantity and quality of membrane phospholipids, particularly in the brain, since brain phospholipids are highly enriched in essential fatty acids, primarily arachidonic acid, an omega-6 series, and docosahexaenoic acid, an omega-3 series. Reduced membrane levels of EFA have been consistently reported in red blood cells, brain and skin fibroblasts from chronically medicated patients with schizophrenia, as well as drug naive patients (20). Therapeutic strategies for the prevention of oxidative damage ROS damage can be ameliorated by at least two mechanisms; inactivation of ROS by dietary antioxidants (e.g., vitamin C, vitamin E), and replacement of lost membrane EFA by dietary supplementation with essential fatty acids. Vitamin E is a lipid soluble antioxidant with the potential to prevent oxidative damage. However, vitamin E cannot prevent oxidative damage to cytosolic proteins, mitochondria, and nuclei, where most of the ROS are generated. Therefore, it may be important to use vitamin E in combination with vitamin C, a water soluble antioxidant. The supplementary use of vitamin C in schizophrenia requires caution since a high dietary intake of iron will result in vitamin C having a prooxidant rather than an antioxidant action. The addition of essential polyunsaturated fatty acids could promote recovery of previously damaged membrane structures. It is proposed that ongoing oxidative cell damage must be stopped and that structural membrane damage farm vestn 2008; 59 169 FV 4 2008 prelom.xp:FV 2 2007 prelom zadnji.xp 10/10/08 3:35 PM Page 170 Pregledni znanstveni œlanki - Review Scientific Articles must be reversed. Since antioxidants alone may stop ongoing oxidative damage and EFA have the potential to restore the cellular structure their combined use may be necessary for optimal treatment of oxidative cell damage (21). The results of studies available in the literature in which these therapeutic strategies were used are presented in Table 1 and Table 2. Vitamin E and vitamin C are well known antioxidants that are postulated to protect against damage to biological membranes by their ability to scavenge free radicals. Accordingly, several studies have examined the efficacy of vitamin E or vitamin C in the treatment of schizophrenia (Table 1). According to statistical analysis of the results of ten clinical studies, there is no evidence that vitamin E reduces the symptoms of tardive dyskinesia. The studies were designed as controlled trials involving patients with antipsychotic-induced tardive dyskinesia and schizophrenia, or other chronic mental illness, who were randomly allocated to either vitamin E or to a placebo or no intervention. The overall results for clinically relevant improvement showed no benefit of vitamin E against placebo (6 trials, 256 people). Small scale trials with an uncertain quality of randomisation indicate that vitamin E protects against deterioration of tardive dyskinesia but there is no evidence that vitamin E improves symptoms of this disease (22). As concerns vitamin C, there is a lack of available data. In the first study that we identified the aim was to examine the effect of peroral application of vitamin C with atypical antipsychotics on serum malondialdehyde, plasma ascorbic acid levels, and Brief Psychiatric Rating Scale (BPRS) score in patients with schizophrenia. The patients with schizophrenia had increased serum malondialdehyde levels and decreased plasma ascorbic acid levels, which proves increased oxidative stress. These levels were significantly reversed after treatment with vitamin C along with atypical antipsychotics compared to placebo with atypical antipsychotics. BPRS scores improved significantly with addition of vitamin C as compared to Table 1: Effect of supplemental treatment (vitamin E and C) on patients with schizophrenia in double blind randomised studies. Reports for vitamin E were included according to data from the Cochrane library data base (22). Preglednica 1: Uœinek adjuvantne terapije (vitamin E in C) pri bolnikih s shizofrenijo v dvojno slepih randomiziranih øtudijah. Podatki za adjuvantno terapijo z vitaminom E so v skladu s podatkovno bazo “Cochrane library data base” (22). Vitamin E studies Study duration, number of patients Intervention Outcome Adler 1993 36 weeks, N=40 Vitamin E 1600 IU/day Significant reduction of AIMS score in favour of vitamin E Adler 1999 1 year, N=158 Vitamin E 1600 IU/day No significant reduction of AIMS and BPRS Akhtar 1993 4 weeks, N=32 Vitamin E 1200 IU/day Significant reduction of TDRS Dabiri 1994 12 weeks, N=12 Vitamin E 1200 IU/day Significant reduction of AIMS Egan 1992 6 weeks, N=21 Vitamin E 1600 IU/day No significant reduction of AIMS Elkashef 1990 4 weeks, N=10 Vitamin E 1200 IU/day Significant reduction of AIMS Lam 1994 6 weeks, N=16 Vitamin E 1200 IU/day No significant reduction of AIMS Lohr 1996 8 weeks, N=55 Vitamin E 1600 IU/day Significant reduction of AIMS and not of BPRS Sajjad 1998 7 months, N=20 Vitamin E 600 IU/day Significant reduction of AIMS score Schmidt 1991 2 weeks, N=23 Vitamin E 1200 IU/day No significant reduction of AIMS Vitamin C studies Study duration, number of patients Intervention Outcome Nikolaus 2002 * (23) 2 years , N=6 Vitamin C 200 mg/day and vitamin E 1.8 mg/day Significant reduction in dyskinetic movements total score Vitamin C 500 mg/day Significant reduction in MDA and BPRS Dakhale 2005 (24) 8 weeks , N=40 * prospective open study (AIMS- Abnormal Involuntary Movement Syndrome Scale, BPRS- Brief Psychiatric Rating Scale, PANSS- Positive and Negative Syndrome Scale, M-ADRSMontgomery-Asberg Depression Rating Scale, S-ARS- Simpson-Angus Rating Scale, TDRS- Tardive Dyskinesia Rating Scale, CGI- Clinical Global Impression Scale, QOL- Henrich’s Quality of Life scale, EPA- Eicosapentaenoic acid, E-EPA- Ethyl eicosapentaenoic acid, DHA- Docosahexaenoic acid, MDA- Malondialdehyde). (AIMS- Lestvica abnormalnih nehotnih gibov, BPRS- Kratka psihiatriœna ocenjevalna lestvica, PANSS- Lestvica za ocenjevanje pozitivnega in negativnega sindroma, M-ADRS- Montogmery-Asberg ocenjevalna lestvica depresije, S-ARS- Simpson-Angus ocenjevalna lestvica, TDRS- Ocenjevalna lestvica tardivne diskinezije, CGI- Lestvica sploønega kliniœnega vtiska, QOL- Henrihova lestvica ocenjevanja kakovosti æivljenja, EPA- Eikozapentaenojska kislina, E-EPA- Etil eikozapentaenojska kislina, DHA- Dokozaheksaenojska kislina, MDA- Malondialdehid). 170 farm vestn 2008; 59 FV 4 2008 prelom.xp:FV 2 2007 prelom zadnji.xp 10/10/08 3:35 PM Page 171 Can supplementation with vitamin E or C and omega-3 or -6 fatty acids improve ... Table 2: Effect of supplemental treatment (polyunsaturated fatty acids or a combination of antioxidants and polyunsaturated fatty acids) on patients with schizophrenia in double blind randomised studies. Reports for fatty acid supplemental therapy were included according to data from the Cochrane library data base (25). Preglednica 2: Uœinek adjuvantne terapije (polinenasiœene maøœobne kisline ali kombinacija antioksidanta in polinenasiœenih maøœobnih kislin) pri bolnikih s shizofrenijo v dvojno slepih randomiziranih øtudijah. Podatki za adjuvantno terapijo s polinenasiœenimi maøœobnimi kislinami so v skladu s podatkovno bazo “Cochrane library data base” (25). Fatty acids studies Method Intervention Outcome Emsley 2002 12 weeks, N=40 E-EPA 3g/day Significant reduction in PANSS scores Fenton 2001 16 weeks, N=90 E-EPA 500 mg/day and vitamin E No significant change in PANSS, M-ADRS, AIMS, S-ARS, CGI Peet 2001 12 weeks, N=55 EPA 2g, DHA 2g Comparative study Significant reduction in PANSS scores. EPA is superior to DHA Peet 2002 12 weeks, N=55 EPA 1g/day, EPA 2g/day, EPA 3g/day, EPA 4g/day. Comparative study Significant reduction in PANSS scores, the bigest for those who had EPA 2g/day Wolkin 1986 12 weeks, N=55 Gama-linoleic acid 600 mg/day No significant reduction in AIMS Mellor 1995 6 weeks, N=20 EPA, 10 g MaxEPA fish oil Significant reduction in PANSS scores and AIMS Vitamins E and C and fatty acids Method Intervention Outcome EPA/DHA 180:120 mg Vitamin E/C 400 IU/ 500mg Significant reduction of PANSS and BPRS and increase of QOL Arvindakshan 2003 (21) 4 months, N=33* * prospective open study (AIMS- Abnormal Involuntary Movement Syndrome Scale, BPRS- Brief Psychiatric Rating Scale, PANSS- Positive and Negative Syndrome Scale, M-ADRS- Montgomery-Asberg Depression Rating Scale, S-ARS- Simpson-Angus Rating Scale, TDRS- Tardive Dyskinesia Rating Scale, CGI- Clinical Global Impression scale, QOL- Henrich’s Quality of Life scale, EPA- Eicosapentaenoic acid, E-EPA- Ethyl eicosapentaenoic acid, DHA- Docosahexaenoic acid, MDA- Malondyaldehide). (AIMS- Lestvica abnormalnih nehotnih gibov, BPRS- Kratka psihiatriœna ocenjevalna lestvica, PANSS- Lestvica za ocenjevanje pozitivnega in negativnega sindroma, M-ADRS- Montogmery-Asberg ocenjevalna lestvica depresije, S-ARS- Simpson-Angus ocenjevalna lestvica, TDRS- Ocenjevalna lestvica tardivne diskinezije, CGI- Lestvica sploønega kliniœnega vtiska, QOL- Henrihova lestvica ocenjevanja kakovosti æivljenja, EPA- Eikozapentaenojska kislina, E-EPA- Etil eikozapentaenojska kislina, DHA- Dokozaheksaenojska kislina, MDA- Malondialdehid). placebo after 8 weeks of treatment. It can be concluded that oral supplementation of vitamin C with atypical antipsychotics restore ascorbic acid levels, reduces oxidative stress, and improves the BPRS score (24). In the second study when a combination of both antioxidants (vitamin E and vitamin C) was used, the results showed that the dyskinetic movements total score was significantly reduced. Results of the vitamin combination are promising and further studies on this combination therapy are suggested (23). It is difficult to make a direct comparison between vitamin C and vitamin E effects in schizophrenia according to available clinical studies. Class of antipsychotic treatment, duration of disease and duration of treatment should be standardised. Moreover, there are only two vitamin C studies, and one of them is conducted on six patients. Furthermore, to compare antioxidant effects, we would need to evaluate markers of oxidative stress and oxidative damage. In the light of presented data, additional randomised clinical study with vitamin C, vitamin E and placebo group would be needed. Patients should be treated with same group of antipsychotics (suggested is typical antipsychotic) and markers of oxidative stress and oxidative damage should be quantified. To review the effects of EFA supplementation of antipsychotic treatment for schizophrenia-like illnesses we present the most recent data (Table 2). When the use of omega-3 is compared to placebo, small scale short trials suggest that the need for antipsychotics appears to be reduced in patients treated with omega-3 supplementation due to improvement in their mental state. There are limited data comparing the effect of omega-6 to placebo. For movement disorder outcome, only one small study does not show any difference for the average short-term endpoint AIMS score. When different omega 3 fatty acids (E-EPA, EPA, DHA) are compared there is no clear difference in the outcome of Positive and Negative Syndrome Scale (PANSS) scores. Comparison of different dose levels of omega-3 with placebo revealed no difference in the measure of global and mental state. Despite all these data, there is currently no farm vestn 2008; 59 171 FV 4 2008 prelom.xp:FV 2 2007 prelom zadnji.xp 10/10/08 3:35 PM Page 172 Pregledni znanstveni œlanki - Review Scientific Articles clear evidence of the effectiveness of fatty acids. Clinicians should prescribe an omega-3 preparation as part of a well-designed randomised trial. It is important that researchers record and release all clinically relevant data. There are still too few data on the role of essential fatty acid supplementation in the treatment of patients with schizophrenia. The value of polyunsaturated fatty acids for treating schizophrenia is not yet confirmed. The intriguing theory behind their use and even the possibility of a clinical effect could create a whole new path of research. Support of a substantial study would seem warranted (25). Despite the fact that combined therapy with antioxidants and EFA is potentially more effective than monotherapy in patients with schizophrenia, we have identified only one study with an appropriate design (21). In this study morning and evening oral supplementation with antioxidants (vitamin E/C, 400 IU: 500 mg) and a mixture of EPA/DHA (180:120 mg) was used in treatment of patients with schizophrenia (N = 33) for 4 months. Post-treatment levels of red blood cell EFA were significantly higher than pre-treatment levels, as well as the levels in healthy controls, without any significant increase in plasma peroxides. Additionally, there was a significant reduction in psychopathology based on a reduction in individual total scores on the Brief Psychiatric Rating Scale (BPRS) and Positive and Negative Syndrome Scale (PANSS) and an increase in Henrich’s Quality of Life (QoL) Scale. General psychopathology-PANSS is part of the whole PANSS and its mention does not mean much if the changes on the part of positive and negative symptoms are not quoted. (21). Conclusion The use of antioxidants and omega-3 polyunsaturated fatty acids in the treatment of schizophrenia still remains to be established and there is a need for large well designed, conducted and reported studies. Future studies need to be done in placebo-controlled trials with a larger number of patients, both chronic as well as drug naive, and for a longer duration of treatment while the dietary intake is monitored. Previous studies indicated several critical issues that must be considered in designing and carrying out future studies. The age of the patients and years of the illness may be an important issue since the age has been associated with the potentially reduced antioxidant defence, and the years of illness and treatment, particularly with classical antipsychotics such as haloperidol, may lead to state of membrane pathology which is difficult to repair. Despite the fact that some of the studies gave positive results, there is currently no reason for clinicians to either encourage or discourage the use of polyunsaturated fatty acids. If a person with schizophrenia wishes to use EFA supplementation then an omega-3 preparation should be the preferred option. Finally, combined therapy with antioxidants and EFA has an improved potential in preventing oxidative damage and repairing already existing damage, but this has to be confirmed in future clinical studies. Polyunsaturated fatty acids (omega-3) together with antioxidant vitamins could be an effective, low cost, supplemental treatment with few side effects. Therefore, such therapy would be a significant advance in the treatment of schizophrenia. 172 farm vestn 2008; 59 Literature 1. Nestler EJ, Hyman SE, Malenka RC. Higher cognitive function and Psychosis. In: Molecular neuropharmacology: A foundation of Clinical Neuroscience. McGraw-Hill companies, Inc., 2001: 383-407. 2. Mahadik SP, Pillai A, Joshi S et al. Prevention of oxidative stressmediated neuropathology and improved clinical outcome by adjunctive use of a combination of antioxidants and omega-3 fatty acids in schizophrenia. Int Rev Psychiat 2006; 18: 119-131. 3. Ranjekar PK, Hinge A, Hegde MV et al. Decreased antioxidant enzymes and membrane essential polyunsaturated fatty acids in schizophrenic and bipolar mood disorder patients. Psych Res 2003; 121: 109–122. 4. Laurence DR, Bennet PN, Brown MJ. Drugs and mental disorder. In: Clinical pharmacology. Churchill Livingstone, 1997: 330. 5. Yao JK, Ravinder DR, Van Kammen DP. Oxidative damage and schizophrenia. CNS Drugs 2001; 15: 287-310. 6. Parikh V, Khan MM, Mahadik SP. Differential effects of antipsychotics on expression of antioxidant enzymes and membrane lipid peroxidation in rat brain. Journal of Psychiatric Research 2003; 37: 43–51. 7. Pillai A, Parikh V, Terry AV Jr et al. Long-term antipsychotic treatments and crossover studies in rats: Differential effects of typical and atypical agents on the expression of antioxidant enzymes and membrane lipid peroxidation in rat brain. Journal of Psychiatric Research 2007; 41: 372–386. 8. Krop S, Kern V, Lange K et al. Oxidative stress during treatment with first and second-generation antipsychotics. J Neuropsychiatry Clin Neurosci 2005; 17: 227-231. 9. Mahadik PS, Mukherjee S. Free radical pathology and antioxidant defence in schizophrenia: a review. Schizophr Res1996; 19: 1-17. 10. Mahadik PS, Evan D, Lal H. Oxidative stress and role of antioxidant and w-3 essential fatty acid supplementation in schizophrenia. Rag Nemo-Psychopharmacol & Bwl Psychiat 2001; 25: 463-493. 11. Halliwell B, Gutteridge MCJ. Antioxidant defence: sequestration of metal ions, Reactive species can be poisonous: their role in toxicity, Reactive species and disease: fact, fiction or filibuster? In: Free radicals in biology and medicine. 4th edition, Oxford university press, 2007: 133, 454-456, 576-577, 594-595. 12. Hermida-Ameijeiras A, Mendez-Alvarez E, Sanchez-Iglesias S et al. Autoxidation and MAO-mediated metabolism of dopamine as a potential cause of oxidative stress: role of ferrous and ferric ions. Neurochem Int 2004; 45: 103–116. 13. Smythies RJ. Oxidative reactions and schizophrenia: a reviewdiscussion. Schizophr Res 1997; 24: 357-364. 14. Cooper JR, Bloom EF, Roth HR. Dopamine. In: The biochemical basis of neuropharmacology. Oxford university press, 2001: 225271. 15. Kopin JI. Catecholamine metabolism: basic aspects and clinical significance. Pharmacol Rev 1985; 37: 333-364. 16. Sagara Y. Induction of reactive oxygen species in neurons by haloperidol. J Neurochem 1998; 71 (3): 1002-1012. FV 4 2008 prelom.xp:FV 2 2007 prelom zadnji.xp 10/10/08 3:35 PM Page 173 Can supplementation with vitamin E or C and omega-3 or -6 fatty acids improve ... 17. Perez-Neri I, Ramrez-Bermudez J, Montes S et al. Possible Mechanisms of Neurodegeneration in Schizophrenia. Neurochem Res 2006; 31: 1279–1294. 18. Linert W, Jameson GNL. Redox reactions of neurotransmitters possibly involved in the progression of Parkinson’s Disease. J Inorg Biochem 2000; 79: 319–326. 19. Fenton SW, Hibbeln J, Knable M. Essential fatty acids, lipid membrane abnormalities, and the diagnosis and treatment of schizophrenia. Biolo Psychiatry 2000; 47: 8-21. 20. Khan MM, Evans RD, Gunna V at al.Reduced erythrocyte membrane essential fatty acids and increased lipid peroxides in schizophrenia at the never-medicated first-episode of psychosis and after years of treatment with antipsychotics. Schizophr Res 2002; 58: 1–10. 21. Arvindakshan M, Ghate M, Ranjekar KP at al. Supplementation with a combination of w-3 fatty acids and antioxidants (vitamins 22. 23. 24. 25. E and C) improves the outcome of schizophrenia. Schizophr Res 2003; 62:195–204. Soares KVS, McGrath JJ. Vitamin E for neuroleptic-induced tardive dyskinesia (Review). Cochrane-Database-Syst-Rev 2001; 4: Art. No.: CD000209. Nikolaus M, Hildegard S, Volker A et al. Severe tardive dyskinesia in affective disorders: Treatment with vitamin E and C. Neuropsychobiology 2002; 46(suppl 1): 28–30. Dakhale GN, Khanzode SD, Khanzode S at al. Supplementation of vitamin C with atypical antipsychotics reduces oxidative stress and improves the outcome of schizophrenia. Psychopharmacology 2005;182: 494–498. Joy CB, Mumby-Croft R, Joy LA. Polyunsaturated fatty acid supplementation for schizophrenia. Cochrane-Database-SystRev 2006, Issue 3. Art. No.: CD001257. farm vestn 2008; 59 173