Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
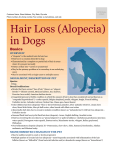
Hair and Nail Disorders Digital Lecture Series : Chapter 24 Col. Manas Chatterjee Senior Adviser, Professor and Head Maj. Shekhar Neema Graded Specialist and Asst Professor Department of Dermatology, Command Hospital (EC), Kolkata CONTENTS HAIR Structure Function Alopecia Excessive hair growth Hair pigmentation Hair cosmetics NAIL Structure Function Nail changes in systemic diseases Nail changes due to drugs Common diseases of nail Basic procedures MCQs Photoquiz Structure of hair Types of hair : Lanugo (seen in utero) Vellus Terminal Hair is a keratinized product of hair follicle. It is present all over skin except on vermillion of lips, palms, soles and skin of nail folds. Functions of hair Concerned with sexual and social communication Protective role eg. nasal and eyelash hair Sensory function: touch sensation Hair Cycle Hair follicles undergo a repetitive sequence of growth and rest called the hair cycle. Anagen is period of active hair growth. Duration of this phase decides the length of hair. In humans, it is maximum on scalp. Catagen is the regressive phase in which the follicular activity declines and ceases. Telogen is the resting phase in which hair stays till the beginning of next anagen phase. Disorders of hair Disorders of hair can either be due to : Loss of hair from hair bearing areas (alopecia) Excessive hair • Androgen dependent hair patterns of typically terminal hair (hirsutism) • Patterns of increased hair growth other than in androgenic distribution (hypertrichosis) Alopecia Classification: Non-cicatricial: preservation of follicles on clinical and histologic examination. Common causes are alopecia areata, androgenetic alopecia, female patterned hair loss and telogen effluvium. Cicatricial (scarring): destruction of follicles due to conditions eg: trauma, infections, cutaneous lupus erythematosus, lichen planus. It is irreversible. There can be either diffuse or localised (patterned / non-patterned ) hair loss. Alopecia areata Chronic inflammatory disease probably due to a T-cell mediated response in genetically predisposed individuals. Environmental factors may trigger the condition. Affects any hair bearing area; can be localized, extensive or diffuse. The involvement of all scalp hair is alopecia totalis and all body hair is alopecia universalis. May be associated with atopy, Down’s syndrome, vitiligo, pernicious anemia, myxoedema, diabetes or hypertension in the family. Alopecia Areata The affected area shows total hair loss without any inflammation; sometimes with short, easily extractable ‘exclamation-mark’ hair at margin. Grey hair spared (going white overnight). Regrowth either spontaneous or following treatment; at first fine and unpigmented but later resumes normal colour and calibre. Nail pitting, onycholysis may be associated. Alopecia Areata Localised Non Scarring Alopecia : Alopecia Areata Differential diagnosis Tinea capitis Trichotillomania Secondary syphilis Androgenetic alopecia Treatment Majority of cases have spontaneous regrowth of hair without any treatment. Steroids (usually topical or intralesional) Topical minoxidil Topical anthralin, phenol Topical immunotherapy: Dinitrochlorobenzene (DNCB), squaric acid dibutyl ester (SADBE), diphencyprone (DPCP) Immunomodulators : Cyclosporin Photochemotherapy Prognosis Majority will get complete regrowth sometimes without treatment in 1 year. A small percentage end up with severe chronic form. Poor prognostic indicators : Onset in childhood, atopy, positive family history, extensive involvement , nail dystrophy, other auto-immune conditions. Androgenetic alopecia (AGA) Most common cause of hair loss. Male patterned baldness(MPB) : 50% men affected by the age of 50 years. Female patterned hair loss(FPHL): 20-50% women affected by age of 50 years. Most likely inherited as autosomal dominant/ polygenic trait from either parent; more from father. Pathogenesis Hormonal factors - 5 alfa reductase changes testosterone to dihydrotestosterone (5-DHT). 5 DHT facilitates miniaturization of hair. Aromatase in contrast inhibits process of miniaturization. Androgen receptors may be increased or may be hyper-responsive in areas affected by AGA. Clinical features Pigmented terminal hairs are progressively replaced by finer, short and virtually non-pigmented hairs. MPHL: pattern of progression is uniform; starts as frontoparietal recession and involves the entire scalp sparing the occipital fringe; graded into 8 stages by Hamilton. FPHL : widened central parting earliest sign; progresses through 3 stages of Ludwig. Male Pattern Alopecia Female Pattern Alopecia Androgenetic Alopecia Patterned Non scarring alopecia : Androgenetic Alopecia Female Pattern Hair Loss Patterned Non scarring alopecia Treatment Medical : • Topical Minoxidil (2 to 10%) • Oral Finasteride (1 mg or less) Surgical : • Follicular unit transplant/extraction • Scalp reduction Cosmetic cover : • Wigs, hair bonding, hair weaving Telogen effluvium (TE) Sudden significant hair loss 2-3 months after an offending insult where hair follicles are pushed prematurely from anagen to telogen phase. Offending insults : fever, post partum, crash dieting, hypoproteinemia, iron deficiency, major surgeries, prolonged anaesthesia, hypo and hyperthyroidism, major internal disease, acute psychologic stress and medication. Trichotillomania Psychiatric disorder in which there is a compulsive habit of pulling out the hair. Bizarre pattern of hair loss in which hair is twisted and broken at various distances from clinically normal scalp Management : may vary from identification of stressful episode with accompanying support, parent education, support of psychologist and psychiatrist, drug therapy (antidepressants etc.) Trichotillomania Alopecia due to tinea capitis Seen essentially in pre-pubertal age group It is patchy, incomplete and is due to breakage of hair shaft invaded by dermatophytes. It is fully reversible except in cases of inflammatory involvement due to species of dermatophytes derived from animals/soil or if inflammatory process destroys the hair follicles Cicatricial alopecia Seen as an area of thin, shiny, dry and depressed skin with telangiectasia; absence of follicular openings. Could be developmental / hereditary, traumatic, secondary to tinea capitis, discoid lupus erythematosus, herpes zoster, bacterial infections, neoplastic disorders, cicatricial pemphigoid, pseudopelade of Brocq Treatment: Excision and primary closure for small patches, autografting and scalp expansion, cosmetic camouflage for large patches. Scarring Alopecia Excessive hair Growth of hair that in any given site is coarser, longer or more profuse than is normal for the age, sex and race. Hirsutism : androgen dependent hair patterns of typically terminal hair. Hypertrichosis : patterns of increased hair growth involving nonandrogen dependent follicles. Hirsutism Growth in females of coarse terminal hair in adult male pattern of distribution i.e. face, chest, upper back. Androgen dependent. Idiopathic or due to hyperplasia / tumors involving ovaries, adrenal cortex or pituitary. May be due to drugs, reduced plasma sex hormone binding globulin, increased androgen receptor or 5 alfa reductase activity in skin. Other causes : HAIR-AN and SAHA syndromes. Approach to a hirsute patient Enquire about the pattern of hirsutism, alopecia, features of virilisation. Probe into the menstrual history, family history and intake of drugs such as glucocorticoids, anabolic steroids. Systemic examination: Deepening of voice, muscle bulk, loss of body contours, hypertension, striae distensae and clitoromegaly. Cutaneous examination: Associated acne, acanthosis nigricans, androgenetic alopecia. Investigate to rule out hormonal aberrations like polycystic ovarian disease or androgen secreting tumors. Treatment Cosmetic : depilatory creams, plucking, bleaching, electrolysis, eflornithine. Lasers : Long pulse Nd:YAG, intense pulse light, diode, alexandrite. Hormonal correction : any tumors have to be removed. Drugs : cyproterone acetate, finasteride, flutamide, spironolactone, leuprolide, ketoconazole, medroxyprogesterone acetate. Hair pigmentation and cosmetics Canities : greying of hair with age. Premature canities : onset of greying before 20 years in Caucasians and 30 years in Africans. Poliosis : localised patch of grey hair; congenital and acquired. Hair cosmetics : shampoos, conditioners, hair dyes and bleaches. Nails Functions of nails Help to grasp and manipulate objects Help in ‘pincer grip’ Protect terminal phalanx and fingertip Serve an aesthetic and cosmetic purpose Nail changes in systemic diseases Clubbing Koilonychia Beau’s lines Subungual hematoma / Splinter hemorrhages Color changes of nails Periungual / subungual tumors Clubbing 3 major categories : Idiopathic Hereditary - congenital Acquired : 80% cases associated with respiratory ailments, 10-15% with cardiovascular and the rest with various extrathoracic diseases like Inflammatory bowel disease. Koilonychia (spoon nails) 3 types : Idiopathic Hereditary Acquired : Trauma, dermatologic diseases, Raynaud’s phenomenon, iron deficiency (not the most common cause) Beau’s lines Transverse depression across nail plate. Caused by serious systemic illness, drug reaction, bullous dermatoses, severe psychologic stress, local trauma, eczemas, idiopathic. Nail changes due to systemic drugs Asymptomatic growth rate change and pigmentation abnormalities are the most common changes. Other changes: Transient shedding, photo-onycholysis, brittle nails, Beau’s lines, permanent nail deformities. Common drugs : Antibiotics like tetracycline, cephalosporins; fluoroquinolones, antimalarials, retinoids, psoralens, chemotherapeutic drugs. Common skin conditions with nail changes Psoriasis Lichen planus Fungal infections Bacterial infections Viral infections Ingrown nails (trauma induced) Eczemas Nail psoriasis Seen in up to 50% of patients with psoriasis May be the first manifestation of psoriasis Seen in several nails; both finger and toe nails may be affected Diagnostic signs include extensive irregular pitting, oil drop sign and onycholysis with erythematous borders. Other abnormalities often seen are nail thickening, subungual hyperkeratosis, nail crumbling etc. Nail psoriasis Nail Lichen planus Nail abnormalities evident in 10% cases with skin / mucosal lichen planus Also occurs in absence of skin / mucosal involvement Thinning and longitudinal ridging / fisssuring of nail plate, pterygium formation, subungual hyperkeratosis Permanent destruction may occur Lichen planus Onychomycosis Involvement of one / few nails Examination of skin may give a clue Four patterns of onychomycosis • Distal and lateral subungual onychomycosis (DLSO) • Proximal subungual onychomycosis (PSO) • White superficial onychomycosis (WSO) • Total dystrophic onychomycosis (TDO) Onychomycosis : causes Caused by dermatophytes, candida and moulds. Is known to affect >10% of population in western world. Predisposing factors : occlusive footwear, diabetes mellitus, hyperhidrosis, immunosuppression, trauma, poor peripheral circulation. Most common pathogens are Trichophyton rubrum, Trichophyton mentagrophytes and candida species. Onychomycosis : see one hand involvement Ingrown nail Common condition due to piercing of nail plate into lateral nail fold Improper trimming of nails and tight, ill-fitting footwear Great toe nail most commonly involved Causes inflammation, pain and sometimes formation of extra granulation tissue Colour changes in nails Leuconychia Nail hyperpigmentation Useful investigations KOH mount Mycologic culture Nail clipping Biopsy-nail plate/nail bed Radiologic studies Therapeutic procedures Chemical nail avulsion using 40% urea Nail avulsion : partial and total Nail splinting Nail matrix injections Chemical / surgical matricectomy Electrosurgery / radiosurgery / cryotherapy, laser ablation of growths like verrucae, myxoid cyst Surgical removal of growths like glomus tumor MCQ’s Q.1) A. B. C. D. Which phase of hair cycle has maximum duration among the following? Catagen Telogen Kenogen Anagen Q.2) Which of the following is not a poor prognostic marker in alopecia areata? A. Nail involvement B. Oophiasis pattern C. Solitary patch D. Associated Autoimmune diseases MCQ’s Q.3) A. B. C. D. Nail involvement is seen in what percentage of psoriasis patient? 10 % 50% 20% None Q.4) What is the most common pattern of nail involvement in onychomycosis? A. Distal - lateral subungal onychomycosis (DLSO) B. Proximal subungal onychomycosis (PSO) C. Total dystrophic onychomycosis (TDO) D. White superficial onychomycosis (WSO) Photo Quiz Classify the type of alopecia and enumerate few causes Photo Quiz Identify the nail disorder Thank You!