Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
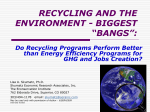
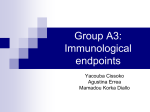
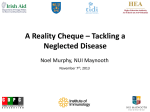
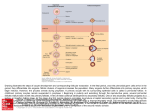
Human Reproduction, Vol.29, No.7 pp. 1380 –1386, 2014 Advanced Access publication on May 8, 2014 doi:10.1093/humrep/deu101 REVIEW Embryology Can healthy babies originate from oocytes with smooth endoplasmic reticulum aggregates? A systematic mini-review Department of Gynaecology, CHU St-Pierre, Université Libre de Bruxelles, rue Haute 322, Brussels 1000, Belgium *Correspondence address. Tel: +32-25-35-34-66; Fax: +32-25-35-34-09; E-mail: [email protected] Submitted on January 23, 2014; resubmitted on March 31, 2014; accepted on April 8, 2014 study question: Is it time to reconsider whether oocytes affected by smooth endoplasmic reticulum aggregates (SERa) should still be destroyed? summary answer: At the time of writing, the literature shows that 171 apparently healthy babies have been born from SERa+ cycles amongst which 22 were from SERa+ oocytes. what is known already: The SER dysmorphism has been associated with negative embryological, clinical and neonatal outcomes, which led to a recommendation in 2011 to avoid inseminating affected oocytes. The data in the literature are nevertheless conflicting and some centres have continued using SERa+ oocytes. study design, size, duration: A systematic mini-review of the literature to 7 November 2013 was performed with the keywords ‘Smooth Endoplasmic Reticulum’ and ‘oocyte’, limited to humans and written in English. participants/materials, setting, methods: Articles (Pubmed) and major abstracts where the effect of the SER dysmorphism was studied as an individual feature on embryological, clinical or neonatal outcomes were included in this review. main results and the role of chance: From a total of 297 publications identified, 13 were selected as being relevant to this review. One hundred eighty-three babies have been reported to be born from SERa+ cycles, 171 were healthy, 8 live births presented malformations, 3 were neonatal deaths, 1 was a stillborn and additionally 4 terminations of pregnancy occurred. limitations, reasons for caution: Data concerning SERa+ oocytes in the literature are scarce, the studies are small, heterogeneous and results are conflicting. The malformations observed could be due to over-reporting of scattered alarming results. Alternatively, an under-reporting of complications cannot be excluded. wider implications of the findings: Centres that have or that are including transfers of SERa+ embryos in their IVF procedures should publish their clinical and neonatal outcomes as well as the follow-up of children. The birth of healthy babies from SERa+ embryos is encouraging and might lead in the future to a revision of the current consensus on the SER dysmorphism. Further research is needed to understand the origin of this dysmorphism and help avoid its occurrence. Therefore, until we have a better understanding of the situation, transfers of affected embryos should be carried out with caution. study funding/competing interest(s): We have no conflicts of interest to declare and no funding was received. Key words: smooth endoplasmic reticulum aggregates / oocyte dysmorphism / clinical outcome / embryology / assisted reproduction & The Author 2014. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: [email protected] Downloaded from http://humrep.oxfordjournals.org/ at South China Agricultural University on June 29, 2014 Chloë Shaw-Jackson*, Nina Van Beirs, Anne-Laure Thomas, Serge Rozenberg, and Candice Autin 1381 Smooth endoplasmic reticulum aggregates: a mini-review Introduction Methods A Pubmed systematic literature search using the keywords ‘Smooth Endoplasmic Reticulum’ and ‘oocyte’ limited to humans was performed (last search on 21st October 2013), as well as in the Human Reproduction, Fertility and Sterility and Reproductive Biomedicine Online Journals (last search on 7th November 2013). English articles identified by the search were selected for inclusion in the review if they reported data concerning the effect of the SER dysmorphism on at least one of the following outcomes: fertilization rate, pregnancy rate, miscarriage rate, implantation rate, embryo quality and neonatal outcome. Results Design and limitations of the studies The search identified a total of 297 records and 13 of these were selected for this review (Fig. 2). These included 5 articles, 7 abstracts and 1 case report. The design of the majority of the studies was retrospective (n ¼ 9) (Table I), although for one of them, the authors claimed the study to be randomized. Two studies were prospective, one specified that transfer of SERa+ embryo transfers was avoided (Ebner et al., 2008) and for the other one, no information on embryo selection was provided (Yang et al., 2008). Only two retrospective studies specified that embryos were selected for transfer irrespective of the presence of SERa (Bielanska and Leveille 2011; Mateizel et al., 2013) and one specified that SERa+ embryo transfers were avoided (Otsuki et al., 2004). In most studies, it was not mentioned whether information was provided to the patients concerning the presence of SERa nor if patients’ consent was obtained before transfer of affected embryos. In one study however, patients were informed about the presence of SERa+ oocytes and the risk of a reduced pregnancy rate even when SERa2 embryos are transferred (Otsuki et al., 2004). In a second study, the authors specified that the rare transfers of SERa+ embryos only occurred after consultation with the patients (Ebner et al., 2008). Preferential transfers of SERa2 over SERa+ embryos introduce a bias for cycle comparisons and even more so for oocyte comparisons. When studying the effect of oocyte morphology on clinical outcome, the endpoint should at least be childbirth. Data concerning neonatal outcomes for SERa+ embryos and even SERa2 embryos from SERa+ cycles are scarce in the literature. In 5 publications, mainly abstracts, no neonatal Figure 1 Human metaphase II oocytes as viewed by light microscopy. (A) A metaphase II oocyte containing an SERa (arrow) (400× magnification). (B) A metaphase II oocyte with a fluid-filled vacuole (arrow) (400× magnification). Downloaded from http://humrep.oxfordjournals.org/ at South China Agricultural University on June 29, 2014 In 2011, it was recommended not to inseminate oocytes affected by smooth endoplasmic reticulum aggregates (SERa), since they might be associated with an increased risk of abnormal outcome (Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology, 2011). Several reports focusing specifically on SERa+ cycles/oocytes have indeed shown negative outcomes in terms of fertilization, embryo development and pregnancy rates as well as compromised obstetric and neonatal outcomes (Otsuki et al., 2004; Ebner et al., 2008; Akarsu et al., 2009; Wallbutton and Kasraie, 2010; Sá et al., 2011). However, a recent publication demonstrated that healthy babies could be obtained using oocytes that contain SERa (SERa+ oocytes) (Mateizel et al., 2013). The data in the literature are controversial and some authors present results for SERa+ cycles, others for SERa+ oocytes. Indeed, oocytes that appear at first sight using light microscopy as negative for SERa but which arise from the same cohort of SERa+ gametes (defined as SERa+ cycles), may in fact also be affected when studied using transmission electron microscopy (Otsuki et al., 2004). In order to have a clear overview of what is known, we performed a systematic mini-review analyzing clinical outcomes for SERa+ cycles and oocytes. SERa can be clearly distinguished morphologically by light microscopy from fluid-filled vacuoles as shown in Fig. 1. 1382 Shaw-Jackson et al. data were available (Table I) and unfortunately, no full length articles were published at a later date. Methodology of studies on SERa In 2 studies, fertilization was significantly decreased for SERa+ oocytes and in one study for SERa+ cycles (Table II). There was a trend towards lower clinical pregnancy (CP) rates in all studies for SERa+ oocytes compared with SERa2 oocytes but this decrease was only significant in one study. For SERa+ and SERa2 cycles, one report showed a significant decrease in pregnancy rates for SERa+ cycles. Effect of SERa on miscarriage and implantation rates Three studies reported data on the effect of SERa+ oocytes on biochemical pregnancy and/or miscarriage rates. Transfer of SERa+ embryos was found to increase the risk of miscarriage by 20% in one of the studies (Braga et al., 2013). For SERa+ cycles, 6 studies reported data. One study showed that the combined biochemical pregnancy and miscarriage rates were significantly higher for SERa+ cycles compared with SERa2 cycles (Ebner et al., 2008). A second study reported an increased biochemical pregnancy rate for SERa+ cycles compared with SERa2 cycles (Otsuki et al., 2004). Four and 3 studies analyzed the effects of SERa+ cycles and SERa+ oocytes, respectively, on implantation rates. One study demonstrated a significant decrease of implantation rates for SERa+ cycles (Otsuki et al., 2004). Effect of SERa on embryo quality The effect of SERa on embryo quality was studied in 10 publications. These data included Day 3 and Day 5 analysis, cell fragmentation, cell number, embryo cleavage rate, blastulation, inner cell mass quality and cycle efficiency. Two studies found a significant decrease of embryo quality for SERa+ cycles (Sá et al., 2011; Mateizel et al., 2013) and 3 for SERa+ gametes (Ebner et al., 2008; Sá et al., 2011; Braga et al., Figure 2 Flow chart for the systematic literature search on ‘Smooth Endoplasmic Reticulum’ in humans. Table I Methodology employed and outcomes studied when evaluating smooth endoplasmic reticulum aggregate positive (SERa1) cycles in women. Authors, Year published Study design SERa1 cycles (n) SERa1 cycles (%) SERa1 oocytes (%) FR PR IR MR EQ PO ............................................................................................................................................................................................. Otsuki et al. (2004) RS 18 9.4 De Los Santos et al. (2005)* RS 107 9.2 Maldonado et al. (2006)* RRS1 16 y y Yang et al. (2008)* PS 71 2.8 19.0 y y 30 6.2 25.0 y y y y y y Ebner et al. (2008) POS Munaswamy et al. (2008)* RS Akarsu et al. (2009) CR 3 Sá et al. (2011) RS 60 y y y y y y y y y y y y y y y y y y 10.3 18.8 19.3 y y y 17.6 y y y Bielanska and Leveille (2011)* RS 121 Mateizel et al. (2013) 394 5.4 RS 34.4 Braga et al. (2013) CCS Miwa et al. (2013)* RS 86 7.3 y Hattori et al. (2013)* RS 102 7.8 y y y y y y y y y y y y 20.4 y y y RS, retrospective study; RRS, randomized retrospective study; PS, prospective study; POS, prospective observational study; CCS, case control study; CR, case report; FR, fertilization rate; PR, pregnancy rate; IR, implantation rate; MR, miscarriage rate and/or BCR biochemical rate; EQ, embryo quality; PO, perinatal outcome; % SERa+ cycles ¼ n SERa+ cycles/n total cycles; % SERa+ oocytes ¼ n SERa+ oocytes/n total oocytes in SERa + cycle; y ¼ yes, outcome studied. *Abstracts. 1the authors claim that their study was an RR study, but we have no way to clarify this point. Downloaded from http://humrep.oxfordjournals.org/ at South China Agricultural University on June 29, 2014 For 2 studies, the frequency of SERa was provided per embryo (375/5516); (Braga et al., 2013) or per patient (53/510); (Munaswamy et al., 2008) instead of per cycle (Table I). For 10 studies, authors analyzed either differences between SERa+ and SERa2 cycles (n ¼ 3) or between SERa+ and SERa2 oocytes in the same cycle (n ¼ 2) or data from both (n ¼ 5). Two studies were only included for their data provided on neonatal outcome (Akarsu et al., 2009; Miwa et al., 2013) and finally a case– control study reported on blastocyst quality and pregnancy outcomes per studied embryo (Braga et al., 2013). Fertilization and clinical pregnancy rates for SERa1 versus SERa2 cycles and oocytes 1383 Smooth endoplasmic reticulum aggregates: a mini-review Table II Comparison of fertilization and CP rates between SERa1 and SERa2 cycles and oocytes in women. Authors, year published Fertilization rate CP rate ........................................................................ ........................................................................ SERa1 cycles (%) SERa2 cycles (%) SERa1 oocytes (%) SERa2 oocytes (%) SERa1 cycles (%) SERa2 cycles (%) SERa1 oocytes (%) SERa2 oocytes (%) ............................................................................................................................................................................................. Otsuki et al. (2004) 81.6 85.2 Maldonado et al. (2006) 69.8 71.0 Munaswamy et al. (2008) 5.6* 47.1 86.0 Yang et al. (2008) 28.2* 50.1 88.0 32.0* 68.0* 73.0 36.5 45.2 71.9 58.9** 77.4** 26.7 41.1 73.0 77.0 21.0 36.0 Sá et al. (2011) 69.9* 76.0* 44.7* 75.8* 47.3 38.4 25.0 52.5 Mateizel et al. (2013) 76.2 73.5 72.9 77.0 33.0 32.4 22.6 32.4 Hattori et al. (2013) 68.9 70.7 62.6 70.2 25.4 21.0 13.5 29.2 Bielanska and Leveille (2011)*** Blanks in table reflect no available data. CP: clinical pregnancy; P values refer to the comparisons between SERa+ and SERa2 cycles or oocytes. *P , 0.05 **P , 0.01 and *** no statistics. A total of 171 healthy babies were born from SERa+ cycles and perinatal complications occurred in 16 pregnancies (Table III). These complications included 1 stillborn, 2 neonatal deaths and 13 malformations, which led to 4 pregnancy terminations and 1 neonatal death (Table III). Altogether, 22 healthy babies were born specifically from SERa+ embryos, including fresh and cryopreserved transfers and also twin births originating from mixed transfers. Malformations were observed in 3 pregnancies with SERa+ embryos. Three studies (Ebner et al., 2008; Sá et al., 2011; Mateizel et al., 2013) allowed us to calculate the malformation rate per live birth for SERa+ cycles: a malformation rate of 5.6% (7/126) was obtained, compared with 2.2% (38/1762) for SERa – cycles. small SERa and associated mitochondria act as Ca2+ stores (Sá et al., 2011; Sathananthan, 2013). The fundamental role of Ca2+ in fertilization and early embryo development has been demonstrated by numerous studies (Homa et al., 1993; Carroll et al, 1996). The presence of SERa disturbs Ca2+ stores and oscillations (Van Blerkom, 2011). When normal metaphase II oocytes and SERa+ oocytes were loaded with a fluorescent Ca2+ reporter and activated with the Ca2+ ionophore A23187, instead of a normal transient and uniform signal, free Ca2+ increases occurred in distinct regions for longer durations in affected oocytes (Van Blerkom, 2011). Otsuki et al. (2004) showed that SERa disappear 16 –20 h after ICSI. Indeed, when fertilization of an affected egg occurs, the calcium release would be accompanied by the disappearance of the aggregates. On the other hand, several authors describe the presence of SERa in unfertilized eggs after conventional IVF (Van Blerkom and Henry, 1992; Meriano et al., 2001). In this case, the absence of a Ca2+ release might explain the unfertilized status of the egg and the continued presence of the SERa. Although the rescue of unfertilized eggs containing SERa with Ca2+ ionophores might be considered, extreme caution should be taken, since calcium patterns may be far from normal. A study in rabbits, where the first calcium rise was increased experimentally did not appear to affect preimplantation embryo development. However, during the fetal stages, major developmental and differentiation defects in organogenesis were observed (Ozil and Huneau, 2001). Discussion Role of SERa in adverse clinical outcomes 2013). For SERa+ cycles, the first case described decreased embryo cleavage and blastocyst formation (Sá et al., 2011). The second case reported a reduced cycle efficiency (selection of embryos for transfer or cryopreservation) when embryos were cultured to Day 5 (Mateizel et al., 2013). Concerning SERa+ oocytes, a reduced cleavage rate (Sá et al., 2011), blastocyst formation (Ebner et al., 2008; Sá et al., 2011), inner cell mass quality (Braga et al., 2013) and blastocyst expansion (Braga et al., 2013) were observed. Perinatal outcomes, for embryos, originating from SERa1 cycles Origin of SERa and the role of calcium The appearance of SERa may be due to ovary hyper-stimulation (Van Blerkom and Henry, 1992). Indeed, several studies have demonstrated that the duration of ovarian stimulation was found to be longer and the total amount of gonadotrophins administered higher for cycles with affected gametes (Otsuki et al., 2004; Ebner et al., 2008; Sá et al., 2011). Analysis of the occurrence of SERa in spontaneous cycles as well as determining the effect of a change of stimulation protocol on aggregate recurrence would help our understanding of the origin of this pathology (Ebner et al., 2013). In normal oocytes, SER vesicles, Even though there are conflicting results in the literature, the data show that SERa do affect clinical and embryological outcomes to a certain extent. Variation in population, fertility etiology, stimulation protocols and study design and size can probably explain part of these discrepancies. In terms of perinatal complications, a total of 16 incidents out of 187 pregnancies were found in the literature when studying SERa. One must keep in mind though, that the majority of transfers included in these studies concern SERa2 embryos originating from SERa+ cycles. The largest study by Mateizel et al. (2013) described a major malformation rate per live birth for SERa 2 cycles of 2.1%. If we include pregnancy terminations and stillborns, this rate is increased to 4.2% Downloaded from http://humrep.oxfordjournals.org/ at South China Agricultural University on June 29, 2014 72.0 72.8 Ebner et al. (2008) 1384 Shaw-Jackson et al. Table III Perinatal outcomes for babies born from fresh or cryopreserved SERa1 cycles. Authors, year published Type of embryo transfer Perinatal outcomes .............................................................................................. HB PC Type of PC ............................................................................................................................................................................................. Akarsu et al. (2009) SERa+ Sá et al. (2011) SERa+ Bielanska and Leveille (2011) SERa+ 1 Mateizel et al. (2013) SERa+ 10 Hattori et al. (2013) SERa+ 4 SERa2 SERa2 3 Bielanska and Leveille (2011) SERa2 16 Sá et al. (2011) SERa2 23 Miwa et al. (2013) SERa2 14 Mateizel et al. (2013) SERa2 59 Ebner et al. (2008) Mix Sá et al. (2011) Mix 52 Bielanska and Leveille (2011) Mix Mateizel et al. (2013) Mix Total 2 multiple malformations (1 PT, 1 neonatal death) 1 1 ventricular septal defect 1 1 Beckwith-Wiedemann syndrome 1 1 diaphragmatic hernia 4 1 stillborn, 3 malformations* 2 2 neonatal deaths 133 2 1 heart defect + omphalocele (PT) and 1 Down syndrome (PT) 232 3 1 47 XX+18 (PT), 2 malformations* 171 16 HB, healthy babies; PC, perinatal complications; Mix, mixed transfer of SERa+ and SERa2 embryos; PT, pregnancy termination. 2,3 Twin pregnancies for mixed transfers are specified: 22 twin pregnancies; 33 twin pregnancies. *Included the following: 1 47 XY+21, 1 duplicated kidney; 2 brachialis paresis, 1 hypospadias. (63/1490) compared with 8.6% for SERa+ cycles reported in this review. Amongst the variety of pathologies detected, one case of a Beckwith – Wiedemann syndrome was found. An increased incidence of imprinting diseases may be correlated with the use of assisted reproduction techniques (Manipalviratn et al., 2009). Whether there is an association between SERa and imprinting disorders is unknown. Akarsu et al. (2009) published a case report where multiple fetal malformations were found for two pregnancies where the patient systematically had all oocytes affected in 3 consecutive cycles. In a second case report (Wallbutton and Kasraie, 2010), a patient had fertilization failure by conventional IVF and practically all of her 15 oocytes displayed large SERa (.25 mm). In two subsequent ICSI cycles, again most oocytes were affected and poor fertilization, embryonic arrest and no pregnancies were reported. In this study, polscope analysis did not detect a displacement of the meiotic spindle and the authors concluded that a genetic element would help to explain the relative homogeneity of SERa formation within successive oocyte cohorts. These observations raise the question of whether a threshold exists between the frequency and/or size of the aggregates for which the risk of a negative outcome might exist (Ebner et al., 2013). On the other hand, malformations have been reported for transfers of non-affected embryos originating from SERa+ cycles (Otsuki et al., 2004; Ebner et al., 2008; Mateizel et al., 2013). Frequency of SERa1 cycles/oocytes and ethical considerations This review shows that up to 10% cycles can present SERa, and a range of 19– 34% of oocytes per affected cycle are shown to be positive for aggregates by observation under light microscopy. These percentages are underestimates since oocytes that are fertilized by conventional IVF would generally not show the dysmorphism at the time of fertilization assessment (Van Blerkom and Henry, 1992; Meriano et al., 2001; Otsuki et al., 2004). In addition, more subtle re-organization of the SER might go unnoticed by light microscopy (Otsuki et al., 2004). Cases other than those described above (Akarsu et al., 2009; Wallbutton and Kasraie, 2010) where a whole cohort of oocytes is affected by this dysmorphism have been reported. Indeed, Maldonado et al., (2006) published 16 cycles where patients had mixed ICSI/IVF cycles. All oocytes were affected in the ICSI cycles, but the status regarding SERa of oocytes treated by conventional IVF could not be assessed before Day 1. The chances that all oocytes were affected by SERa are high. Mateizel et al. (2013) reported a healthy birth from one patient in whom all 3 oocytes were affected. Finally, our own unpublished data revealed that over a period of 2 years, 24 cycles occurred with all oocytes affected. The majority of patients had few oocytes, though 7 women had over 3. Additionally, 11 transfers took place with affected embryos since no other embryo of equivalent quality was available (Shaw-Jackson et al., unpublished data). Eight healthy births and 2 ongoing pregnancies occurred from these affected embryo transfers. Taking into account the fact that the presence of SERa+ oocytes has been shown to be recurrent in just under 40% of subsequent cycles (Ebner et al., 2006; Sá et al., 2011), if the ESHRE and Alpha guidelines were to be followed, some couples would have to consider oocyte donation or adoption to achieve a family. Although, these patients represent a minority of those undergoing treatment, each couple should be treated as unique and offered a fair chance of conceiving with their own gametes. This is especially relevant in countries where the Downloaded from http://humrep.oxfordjournals.org/ at South China Agricultural University on June 29, 2014 Otsuki et al. (2004) Ebner et al. (2008) 2 Smooth endoplasmic reticulum aggregates: a mini-review number of fertilized oocytes is restricted. Moreover, supernumerary affected embryos of good quality in larger oocyte cohorts, capable of possibly developing into healthy babies could be cryopreserved and transferred in frozen cycles. Oocyte dysmorphisms affect an important proportion of oocytes. The majority of studies in the past has analyzed pooled data for different dysmorphisms and has not allowed determining which ones are relevant in embryo selection (Rienzi et al., 2011). There is clearly a need to clarify the issue concerning clinical outcomes for SERa+ embryos in order, on the one hand, to reassure the couples involved and on the other hand, to avoid oocyte or embryo wastage. Data in the literature concerning clinical outcomes for SERa as a unique feature are sparse and controversial. It remains unclear whether there is truly an association between SERa and fetal malformations. It is possible that only scattered alarming results are published and that they might not be related to SERa, thus resulting in a biased conclusion. Alternatively, an under-reporting of complications cannot be excluded. Laboratories should record information concerning SERa, and report the clinical outcome or destroy affected gametes. Data should be published with details on frequency and size of aggregates, and a follow-up of babies carried out, in order to determine whether SERa transfers are associated with adverse outcomes. As recently suggested in a letter to the editor (Ebner et al., 2013), the birth of apparently healthy babies from affected gametes might lead to a revision of the current consensus in the future. In the meanwhile, if transfers of affected embryos are performed, they should take place with caution and only when no alternative embryos of sufficient quality are available. Acknowledgements The authors are grateful to Evelyne Bertrand, Jérôme Colin and Bénédicte Becker for helpful scientific discussions. Authors’ roles C.S.-J. did the literature search, data analysis and wrote the manuscript. A.-L.T. and N.V.B. helped with the literature search, C.A. and S.R. were involved in the data analysis. All authors contributed to the scientific discussions. Funding No funding was received for this study. Conflict of interest None declared. References Akarsu C, Cağlar G, Vicdan K, Sözen E, Biberoğlu K. Smooth endoplasmic reticulum aggregations in all retrieved oocytes causing recurrent multiple anomalies: case report. Fertil Steril 2009;92:1496.e1 –1496.e13. Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: proceedings of an expert meeting. Hum Reprod 2011; 26:1270– 1283. Bielanska M, Leveille MC. Live births from oocytes with smooth endoplasmic reticulum (SER) dysmorphism (Abstract of the 27th Annual Meeting of ESHRE: P-105). Hum Reprod 2011;26(Suppl. 1):il63. Braga DP, Setti AS, Figueira Rde C, Machado RB, Iaconelli A Jr, Borges E Jr. Influence of oocyte dysmorphisms on blastocyst formation and quality. Fertil Steril 2013;100:748 – 754. Carroll J, Jones KT, Whittingham DG. Ca2+ release and the development of Ca2+ release mechanisms during oocyte maturation: a prelude to fertilization. Rev Reprod 1996;1:137 – 143. De Los Santos Molina JM, Gamiz P, Albert C, Escribá MJ, Romero JL, De Los Santos MJ. Peculiar embryo phenotypes, are they related with embryo quality, do they affect IVF outcome? (Abstract P-833). Fertil Steril 2005; 84(Suppl. 1):S458. Ebner T, Sommergruber M, Moser M, Shebl O, Schreier-Lechner E, Tews G. Basal level of anti-Müllerian hormone is associated with oocyte quality in stimulated cycles. Hum Reprod 2006;21:2022– 2026. Ebner T, Moser M, Shebl O, Sommerguber M, Tews G. Prognosis of oocytes showing aggregation of smooth endoplasmic reticulum. Reprod Biomed Online 2008;16:113– 118. Ebner T, Shebl O, Oppelt P. Delivery of normal babies from embryos originating from oocytes showing the presence of smooth endoplasmic reticulum aggregates. Hum Reprod 2013;28:2880. Hattori H, Hattori M, Suzuki S, Araki Y, Takeuchi T, Kyono K. Development of babies following use of embryos with smooth endoplasmic reticulum clusters (sERC) in human metaphase II oocytes (Abstract of International Federation of Fertility Societies 21st World Congress on Fertility and Sterility and the 69th Annual Meeting of the ASRM: P-336). Fertil Steril 2013;100(Suppl. 3):S244. Homa ST, Carroll J, Swann K. The role of calcium in mammalian oocyte maturation and egg activation. Hum Reprod 1993;8:1274 – 1281. Maldonado I, Gonzales E, Chamorro M, Luna JJ, Gaytan J, Remohı́ J. Clinical outcome of transferences of human embryos derived from oocytes with smooth endoplasmic reticulum clusters (Abstract of the 62nd annual meeting of ASRM: P-55). Fertil Steril 2006;86(Suppl. 3): S149 – S150. Manipalviratn S, DeCherney A, Segars J. Imprinting disorders and assisted reproductive technology. Fertil Steril 2009;91:305 – 315. Mateizel I, Van Landuyt L, Tournaye H, Verheyen G. Deliveries of normal healthy babies from embryos originating from oocytes showing the presence of smooth endoplasmic reticulum aggregates. Hum Reprod 2013;28:2111 – 2117. Meriano JS, Alexis J, Visram-Zaver S, Cruz M, Casper RF. Tracking of oocyte dysmorphisms for ICSI patients may prove relevant to the outcome in subsequent patient cycles. Hum Reprod 2001;16: 2118 – 2123. Munaswamy VT, Shalu G, Hema S, Sathya B, Re VT. Smooth endoplasmic reticulum clusters and ICSI outcome (Abstract of ‘ART Paving the Way for New Frontiers: ABR-005). Reprod Biomed Online 2008;16(Suppl. 2):S17– S18. Miwa A, Nagai Y, Momma Y, Takahashi K, Chuko M, Nagai A, Otsuki J. Avoiding the occurrence of smooth endoplasmic reticulum clusters in oocytes improves ART outcomes (Abstract of the 29th Annual Meeting of ESHRE: P-165). Hum Reprod 2013;28(suppl. 1):i184– i185. Otsuki J, Okada A, Morimoto K, Nagai Y, Kubo H. The relationship between pregnancy outcome and smooth endoplasmic reticulum clusters in MII human oocytes. Hum Reprod 2004;19:1591– 1597. Ozil JP, Huneau D. Activation of rabbit oocytes: the impact of the Ca2+ signal regime on development. Development 2001;128:917 – 928. Downloaded from http://humrep.oxfordjournals.org/ at South China Agricultural University on June 29, 2014 Conclusion 1385 1386 Rienzi L, Vajta G, Ubaldi F. Predictive value of oocyte morphology in human IVF: a systematic review of the literature. Hum Reprod Update 2011; 17:34 – 45. Sá R, Cunha M, Silva J, Luı́s A, Oliveira C, Teixeira da Silva J, Barros A, Sousa M. Ultrastructure of tubular smooth endoplasmic reticulum aggregates in human metaphase II oocytes and clinical implications. Fertil Steril 2011; 96:143 – 149. Sathananthan AH. Ultrastructure of human gametes, fertilization and embryos in assisted reproduction: a personal survey. Micron 2013;44:1–20. Van Blerkom J. Mitochondrial function in the human oocyte and embryo and their role in developmental competence. Mitochondrion 2011;11:797–813. Shaw-Jackson et al. Van Blerkom J, Henry G. Oocyte dysmorphism and aneuploidy in meiotically mature human oocytes after ovarian stimulation. Hum Reprod 1992; 7:379 – 390. Wallbutton S, Kasraie J. Vacuolated oocytes: fertilization and embryonic arrest following intra-cytoplasmic sperm injection in a patient exhibiting persistent oocyte macro vacuolization—case report. J Assist Reprod Genet 2010;27:183– 188. Yang X, Rosen MP, Abeyta M, Choi T, Cedars MI, Shen S. Impact of smooth endoplasmic clusters (SER) in oocyte cytoplasm on embryo quality and pregnancy outcome (Abstract of the 64th annual meeting of ASRM: P-661). Fertil Steril 2008;90(Suppl. 1):S329 – S330. Downloaded from http://humrep.oxfordjournals.org/ at South China Agricultural University on June 29, 2014