Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
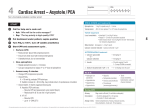
Lifesaver Associates www.tosavelives.com (501) 779-4842 [email protected] (877) NEED CPR Tips on our Classes There will be NO stress (we promise)! We teach more than 40 PALS courses a year, so we’re comfortable with how to present the material so that your retention of the material can be maximized. In our scenarios, some patients may live and may die (which doesn’t necessarily indicate how well you did). Treat your patient, not your monitor. Utilize your resources (cheat books, posters, call pharmacy, etc.). Know your equipment (how to operate EKG monitors/defibrillators, etc.). Also, be familiar whether your defibrillator is monophasic or biphasic. We typically have the group do a mega-code check-off (because that’s the way it would be in real life in your environment). When taking the pre-test, note that the answers are at the very end. Dress comfortably….you will have to briefly provide CPR (it’s now required in all ACLS and PALS courses). Please notify us well before the course if you require a CPR check-off (we must bring additional equipment, tests and course completion cards). Lastly, there have been changes in PALS (effective November 2010). DO NOT get overwhelmed by the two textbooks…..look at this cheat sheet for 18 minutes and review the algorithms. We will highlight possible test questions throughout the course. Other resources, including the pre-test and EKG cards are available at our website (www.tosavelives.com). Go to the ‘Courses’ page and click on the ‘Pre-course information’ link. The username and password are ‘help’ and ‘help’. Please contact us if you experience difficulties in accessing the information. Please don’t hesitate to call us if you have any questions. Andy Goldthorpe [email protected] (501) 779-4842 PALS Priorities Everything begins with providing the CAB’s (circulation & oxygen/ventilation) until we can place the patient on an EKG monitor (to determine whether they are in a shockable or non-shockable rhythm). Everything revolves around the ‘cycles’ of CPR (30 compressions to 2 ventilations for one rescuer, 15:2 for additional rescuers) with a rate of 100 per minute. Ventilations are always 1 second in/1 second out (enough for a visible chest rise). During the first cycle of compressions of a code within a medical facility, the ‘Team Leader’ must start assigning roles. Rotate compressors every 2 minutes (to stay fresh). The first line drug in both pulseless rhythms and bradycardia is Epinephrine (preferably the 1:10,000 concentration via IV or IO). Pulseless Electrical Activity (PEA) is any non-pulsed rhythm that is not VF, VT or asystole. PEA is a problem with the pump, pipes or volume (not an electrical problem)….the electrical system of the heart is still functioning, but the mechanical part of the system is not working. With all pulseless rhythms, we assess the causes as soon as possible (H’s & T’s). Fluid boluses are still the isotonic crystalloids, repeating as needed. Following a defibrillation, we immediately resume cycles of CPR (without looking for rhythm change or feeling for a pulse). We no longer try to shock (or pace) asystole. Remember the levels of consciousness: o A (Alert) o V (Responsive to Verbal Stimuli) o P (Responsive to Painful Stimuli) o U (Unconscious/unresponsive) When tachycardic, we must first determine whether the patient is symptomatic (hypotension, delayed capillary refill, lethargy, absent peripheral pulses). Common Pulseless Rhythms Ventricular Fibrillation Ventricular Tachycardia (look for causes like metabolic/ ingestion) Torsades De Pointes (very uncommon in children) PEA (idioventricular) Asystole Common Rhythms With A Pulse Normal Sinus (normal for most, but make sure it doesn’t deteriorate) Sinus Bradycardia (grave sign….start CPR if less than 60) Sinus Tachycardia (normal in most kids)) Supraventricular Tachycardia (normal in infants/if child is crying) The Heart Blocks (rare) First Degree Second Degree (Type 1) Second Degree (Type 2) Third Degree Automated External Defibrillator (AED’s) Highest priority (coupled with excellent CPR) Recommend immediate CPR and shock with AED or defibrillator within 3 minutes Special Situations: o Children: Prefer using the pediatric patches if available, but could also use adult for anyone besides neonate. AED’s have the ability to buffer down the electricity to some degree o Water: Make sure that the patient’s chest is dry and that they aren’t in a puddle. o Medication patches: remove and dry off residue from patches if blocking the AED patches (if it’s where you need to put your AED patch) o Implanted defibrillator/pacemaker: Put AED patches at least 1 inch away If at any time an AED says ‘no shock is indicated’, check the ABC’s (especially circulation to see whether or not we need to continue CPR) Two phases that you need to remain clear of the patient/AED: o Analyzing (because it needs to get a clear picture of the EKG) o Shocking (because you don’t want to electrocute your co-workers) Vascular Access/Medications PALS still prefers medications to be given via IV or IO (STRONGLY discourage down the ET tube unless there is no other access). Meds that can be administered down the ET tube include ‘LEAN’: Lidocaine, Epinephrine, Atropine, Narcan Epinephrine is 0.01 mg/kg of the 1:10,000 for IV/IO administration and 0.1 mg/kg of the 1:1,000 via ETT. Repeat every 3-5 minutes.