Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
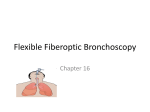
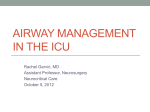
10 January 2014 No 01 AIRWAY FOREIGN BODIES P Slabber Moderator: Prof B Biccard Discipline of Anaesthetics CONTENTS INTRODUCTION ................................................................................................... 3 FOREIGN BODY ASPIRATION ............................................................................ 3 1. Demographics ............................................................................................... 3 2. Diagnosis ....................................................................................................... 4 (a) History: ....................................................................................................... 4 (b) Physical examination:................................................................................ 4 (c) Special investigations:............................................................................... 4 3. Management ................................................................................................... 7 ANAESTHETIC CONSIDERATIONS FOR REMOVAL OF AIRWAY FB’s ........... 7 PREOPERATIVE ASSESSMENT ......................................................................... 8 Middle of the night or the next morning? .......................................................... 9 Premedication ..................................................................................................... 9 INTRA-OPERATIVE CONSIDERATIONS ............................................................ 9 (a) Induction: IV or inhalational? ..................................................................... 10 (b) Ventilation: SV or PPV? ............................................................................. 11 (c) Maintenance: Volatile or TIVA? .................................................................. 12 (d) Pit falls during removal of the FB .............................................................. 13 POST-OPERATIVE CONSIDERATIONS............................................................ 13 CONCLUSION .................................................................................................... 14 REFERENCES.................................................................................................... 15 Page 2 of 16 AIRWAY FOREIGN BODIES INTRODUCTION Aspiration of foreign bodies (FB) by children into the airway is a common problem faced by anaesthetists. Asphyxiation from inhaled FB is one of the leading causes of accidental death among children younger than 4 years.(1) When they present for removal, especially when they are unstable, it often results in a very stressful period for the attending anaesthetist. Historically the mortality related to FB aspiration was estimated at 23%(1), largely due to the ineffective methods of treatment. These included purging, bleeding and the use of emetics. The first successful bronchoscopy for the removal of a pig bone from a bronchus was in 1897 and advances in the surgical and anaesthetic domains since then have resulted in a significant decrease in morbidity and mortality related to the management of airway FB’s(2). Anaesthetists are frequently involved from the initial presentation of the patient to casualty. We play an intricate role in the diagnostic dilemmas and management decisions of these patients and our advice and expertise are central to patient care. Knowledge obtained from the preoperative visit is key as correct decisions on anaesthetic techniques can only be made by an informed anaesthetist which may lead to the difference between a favourable outcome or not. FOREIGN BODY ASPIRATION 1. Demographics In a South African context ingestion of FB’s requiring removal are more prevalent than aspirated FB. Data from the Red Cross children hospital in Cape Town indicated a 5% incidence of aspirated FB, compared to 20% incidence of oesophageal and 40% incidence of nasal FB’s.(3) The vast majority of patients with aspirated FB’s are children. It is particularly prevalent in the age group between 2 and 4 years with the peak incidence at 3 years.(3) Boys account for 60% of these cases compared to girls.(1) The type of FB aspirated is linked to the patient’s age and geographical location. Frequent reports of headscarf pin aspiration by adolescent girls in Turkey are well described. (1) In children organic FB’s account for 80% of aspirated FB’s.(1,4) Of these, nuts especially peanuts are at the top of this list, followed by seeds, beans and bones. Non organic FB account for 20% of which metal and plastic FB’s are most prevalent. Aspirated FB will lodge in the bronchial tree in 88% of cases. (1) The right main bronchus being slightly more common due to anatomical reasons. The rest (11%) will lodge in the larynx and trachea and a minority (1%) impact in different parts of the distal airways. Knowledge of the above trends in FB aspiration will impact on anaesthetic management. Page 3 of 16 Laryngeal or tracheal FB’s are rare but pose the greatest risk of asphyxia and carry a mortality rate of 45% prior to reaching a medical facility. (5) Nuts liberate an irritant oil which result in local inflammation and airway hyper reactivity. Organic FB’s are often missed on X-ray films and a delayed presentation is associated with worsening pulmonary function and reserve which will predispose these patients to perioperative hypoxemia. Organic FB’s are also more prone to fragmenting during removal and prolonged bronchoscopy might be required. 2. Diagnosis Rigid bronchoscopy which is often performed to diagnose aspirated FB is not an innocuous procedure. It carries a major complication rate of 2.4% and mortality rate of 0.42%.(1) For this reason it is imperative to make the correct diagnosis so to not expose patients to this dangerous procedure unnecessarily. To make the correct diagnosis can be difficult and is often based on an index of suspicion. Clinical presentation is variable and depends on; i) the time of presentation since aspiration i.e. “when”, ii) size and shape of the object i.e. “what” and iii) site of the object in the airway i.e. “where”. Unfortunately there is no symptom or sign that is 100% sensitive or specific for FB aspiration. Features on history and examination which lead to a high index of suspicion are valuable in guiding further special investigations and subsequent management.(6) (a) History: A witnessed aspiration event (usually choking) carries a sensitivity of 77% and a specificity of 64% and should lead to a high index of suspicion. (1) A history of coughing, although quite sensitive has a low specificity (40%) and therefore can result in a significant false positive rate which can lead to unnecessary bronchoscopy.(1) A history of cyanosis or stridor is very specific but has poor sensitivity and can result in a significant false negative rate which can lead to undiagnosed aspirated FB with devastating consequences.(1) (b) Physical examination: With an early presentation the clinical examination can range from a completely normal one to that of a severe acute upper airway obstruction. The presence of stridor, voice changes, barking cough or decreased level of consciousness can all indicate laryngeal or tracheal involvement and should heighten our sense of urgency. The clinical triad of acute coughing/choking, localized wheezing, and unilateral diminished breath sounds has a specificity of 98%.(6) Although if this triad is not present it certainly doesn’t exclude the possibility of an aspirated FB. With a late presentation children typically show signs similar to patients with pneumonia e.g. fever, tachypnoea and focal chest signs. (c) Special investigations: The workup of a stable patient should always include a chest X-ray (CXR). Even though 89% of FB’s aspirated is known to be radiolucent, the majority (83%) can show some sign of pathology.(1) Page 4 of 16 Most abnormal features on CXR are more commonly seen after 24 hours of presentation compared to early CXR where the sensitivity and specificity is often low.(7) Indirect signs on CXR include air trapping or localized emphysema (the most commonly found and specific feature), atelectasis, mediastinal shift and collapse/consolidation.(7) Pneumothorax or pneumomediastinum are rare findings. Comparing inspiratory and forced expiratory films will augment the features of air trapping. The hyper-lucent lung field seen is due to a ball valve obstruction by the FB leading to air trapping. Reflex oligaemia due to hypoventilation of the lung field distal to the obstruction also adds to the hyper lucent lung seen on CXR.(8) Co-operation is often not possible in small children and the use of lateral decubitus views looking at the dependent lung for features of air trapping is used to augment this feature. AP and lateral neck X-Ray is a valuable modality to determine location of upper aerodigestive tract FB’s. Flat objects e.g. coins typically align in a sagittal plane when located inside the trachea, but will align in a coronal plane when located inside the oesophagus (see figure 1).(1) A FB that overlaps the boundaries of the airway is unlikely to be located inside the airway, unless penetration of the wall of the airway has occurred.(1) A lateral view (in combination with an AP view) will often reveal the true location of a FB. Figure 1. Coin in the oesophagus on AP and lateral views.(1) Airway fluoroscopy allows dynamic visualization of respiratory airways. It can display decreased diaphragm movements due to air trapping, narrowed airway lumens from a FB and mediastinal shift from air trapping. Although the exposure to radiation is much less compared to CXR, its role for investigating these patients is not yet established as it doesn’t seem to be as sensitive or specific as CT scans.(7) In fact, in a small study of 19 patients its specificity for airway FB was only 17%.(9) Page 5 of 16 Thoracic computed tomography (CT) and virtual bronchoscopy (VB) are new modalities to diagnose airway FB. VB is basically a reformatted 3-dimensional CT image that generates intra luminal views of the airway.(1) CT chest has shown a 100% sensitivity in two studies and therefore showed importantly a zero percent false negative rate.(10,11) Three out of forty five patients thought to have aspirated a FB where correctly identified as not having a FB in the airway by CT scan and so avoided rigid bronchoscopy in those 3 patients.(10) Secretions and airway obstructive lesions like tumours can cause false positives. Limitations to these seemingly perfect investigation modalities are: high cost, limited availability of equipment and staff, requirement of a stable and cooperative child and excessive radiation exposure.(1) An advantage of these investigations is the ability to delineate the shape and exact location of the FB and therefore allow surgical planning (choosing the correct instrument prior to bronchoscopy) and possibly shortening the bronchoscopy and anaesthetic time.(10) Because of its accuracy some authors suggest that a negative CT and VB in these patients do not warrant the currently accepted diagnostic gold standard of a rigid bronchoscopy.(1) A flexible bronchoscope still plays an important role in the diagnosis and recently the management of airway foreign bodies. It is more invasive than CT or VB, but much less traumatic or dangerous compared to diagnostic rigid bronchoscopy. The sensitivity and specificity is excellent and is reported to be close to 100% (comparable to CT).(7) It is typically utilized in patients without a clear history or positive radiological findings of FB aspiration and is able to decrease the negative finding rate of diagnostic rigid bronchoscopy. (1,7) It can be performed with sedation and topical local anaesthesia, but general anaesthesia is often necessary in the paediatric population. Although fewer surgeons utilize this technique for the routine removal of FB’s, it is better suited for removing small distal FB’s and those located in the upper lobes of the lung compared to its rigid counterpart. (1) Fewer instruments (stone baskets are generally used with flexible bronchoscopy) are available to remove FB’s and less control over the FB during removal are important reasons why surgeons generally opt for the rigid bronchoscope. Rigid bronchoscopy is considered the gold standard for diagnosis and management of suspected airway FB’s. Because of the significant complications associated with a missed airway FB, diagnostic rigid bronchoscopy is commonly performed where only a suspicion exists. More appropriately it is recommended that children undergo rigid bronchoscopy only if they have acute asphyxiation, a radio-opaque foreign body or convincing clinical and radiological features (clinical triad and signs of air trapping on X rays).(1) CT, VB or flexible bronchoscope will be appropriate in all other patients to help clarify the diagnosis and minimize unnecessary negative rigid bronchoscopies. A simple flow diagram for suspected airway foreign body diagnoses and management in children has been suggested (figure 2).(7) Page 6 of 16 Figure 2. Diagnostic algorithm for suspected bronchial foreign body in children according to Martinot, 1997. (VBS: vesicular breath sounds. BFB+: positive bronchial foreign body).(7) 3. Management The gold standard method and preferred technique by the majority of surgeons for the removal of airway FB’s is rigid bronchoscopy. This is largely because of the advantages a rigid bronchoscope provides in these cases namely, availability of multiple extraction instruments, good visualization, complete airway and FB control and an excellent conduit for ventilation.(1) ANAESTHETIC CONSIDERATIONS FOR REMOVAL OF AIRWAY FB’s This is broken up into pre-, intra- and post-operative periods. Because the use of a rigid bronchoscope is almost exclusively used in our setting I will concentrate on the anaesthetic implications for this technique. Page 7 of 16 Please note that there is no consensus in the literature yet as to which anaesthetic techniques are considered optimal so I will discuss below some controversies and what is considered acceptable practice based on evidence from systematic reviews and large retrospective cohorts. PREOPERATIVE ASSESSMENT It is very important to make a full pre operative assessment of the patient prior to arrival in the OT. Three main questions that will impact on anaesthetic technique needs to be answered during the history, clinical examination and special investigations: (1) 1. Where is the FB located? Location determines the potential for complete airway obstruction, the most feared complication although very rare.(1) Laryngeal, tracheal and carinal FB’s therefore present the highest risk for inadequate oxygenation or complete airway obstruction.(5) Danger signs would include hypoxia on presentation, stridor, voice changes and dysphonia or aphonia.(5,13) Oesophageal FB’s are more commonly encountered than airway FB’s and morbidity and mortality related to their removal is considerably less as the airway is not shared.(3,13) 2. What was aspirated? Organic material is often problematic because it can absorb fluid and swell causing progressive airway obstruction.(1,13) These FB’s are more prone to fragmenting, but might also need to be crushed intentionally and removed piece by piece adding to anaesthetic time.(12) Nuts and seeds liberate irritant oils causing airway inflammation and irritability with the risk of bronchospasm.(5) Spherical shaped FB’s are prone to complete obstruction of bronchial airways because of their shape which can lead to distal atelectasis with distal suppuration and possible spillage of puss into unaffected parts of the lung once it is removed. (13) They are more difficult to grab and there is the potential to lose grip during retrieval causing a potentially dangerous situation of complete airway obstruction or contra lateral bronchial obstruction with resultant hypoxaemia.(13) 3. When did it happen? Recently aspirated FB’s are more likely to move when the patient coughs and can potentially lodge in the upper airway with detrimental consequences. (1) Delayed presentations are often associated with complications such as infection, airway oedema and formation of granulation tissue (FB is unlikely to move) which make retrieval more difficult and the anaesthetic time longer.(1) They rarely require emergency removal. In the majority of cases fasting (6 hours for solids and 2 hours for clear liquids) is appropriate unless the urgency of the case outweigh the risk of aspiration.(14) Page 8 of 16 In a review of 12979 cases for retrieval of airway FB’s there was no reports of aspiration during bronchoscope, although fatal progression of airway obstruction was reported in 2 cases.(1) The risk of aspiration is less than the risk of worsening hypoxia in urgent cases. Nasogastric tube placement in children after induction but prior to bronchoscopy is appropriate in urgent cases with a significant risk for aspiration.(1) Middle of the night or the next morning? Urgent bronchoscopy should be performed in all cases where airway patency is deemed threatened.(1) Lack of experience from both surgical and anaesthetic teams is a contributing factor to poor outcome in patients undergoing bronchoscopy.(12) In stable patients, a delay in bronchoscopy for removal of airway FB until the next day failed to show an increase in morbidity during a retrospective review of 165 patients.(15) The best timing for bronchoscopy is a controversial issue without adequate guidance available from the literature and is bound to cause tension between caregivers. I believe that individualization for each case is necessary and that all factors (patient status, availability of experienced staff and time of the day) should be considered by surgical and anaesthetic staff in a conjoint decision that best suites the wellbeing of the patient. Premedication Every effort should be made to keep the child calm and prevent coughing spells prior to induction to avoid FB dislodgement and possibly worsening airway obstruction.(14) Sedative premedication requires careful consideration though as sedation can worsen upper airway obstruction and decrease perioperative respiratory drive when a spontaneous ventilation technique is considered.(14) Anticholinergic medication (atropine or glycopyrolate) may be used to dry airway secretions, prevent vagal-induced bradycardia during insertion of the bronchoscope and attenuate cholinergic-mediated bronchoconstriction during airway manipulation, but there use is not routine.(5,14) Antibiotic and steroid medications are indicated to treat infection and laryngeal oedema respectively, especially in delayed presentations where bronchoscopic manipulation is expected to be excessive.(1,12,14) INTRA-OPERATIVE CONSIDERATIONS The main goals of anaesthesia for rigid bronchoscopy are: 1- OXYGENATION 2- IMMOBILE PATIENT These goals are based on the most frequent complications seen during rigid bronchoscopy. Significant morbidity and mortality rates are associated with rigid bronchoscopy when these goals are not met (suboptimal surgical conditions are provided.)(1) Page 9 of 16 Complications include severe laryngeal oedema or bronchospasm, pneumothorax, hypoxic cardiac arrest, hypoxic brain damage and tracheal or bronchial laceration.(1,14) Prior to induction it is vital for the surgeon to be in theatre with the immediate ability to perform rigid bronchoscopy if total airway obstruction occurs. A minimum of two anaesthetists (one for drug administration and the other for airway management) is critical to a successful outcome.(12) Communication between surgeon and anaesthetist is important prior to induction and throughout the whole procedure. Pre-operative concerns and planning (step 1,2,3….) should be raised by both surgeon and anaesthetist and consensus reached before induction.(13) In the ideal situation intravenous access would be established prior to induction with the use of topical local anaesthetic to prevent anxiety in a child. However in a distressed child with difficult veins or in an emergency, establishing IV access immediately after inhalation induction is acceptable.(12,14) Various successful anaesthetic techniques are described for airway FB removal. There is no universally accepted standard method or even evidence based best recipe described. Individualization for each patient seems to be a good approach taking into consideration the condition of the patient, location of the foreign body and personal preference or familiarity with a particular technique.(5) The 4 main intra-operative anaesthetic issues during bronchoscopy are discussed below under induction, ventilation, maintenance and pitfalls: (a) Induction: IV or inhalational? Both intravenous (IV) and inhalational induction are described in the literature with successful outcomes. The choice between IV and inhalational induction seems to be dominated by the location of the FB.(1) In theory, proximal airway FB’s (larynx, trachea and carina) have the ability to move and completely obstruct the airway once spontaneous ventilation (SV) is converted to positive pressure ventilation (PPV) as commonly occur after IV induction.(1,5) For this reason inhalational induction is advocated when proximal airway FB’s are present even though there is a lack of evidence to confirm this theory. Cautious IV induction that maintains spontaneous ventilation is possible, although technically more challenging to achieve. There are no prospective clinical trials that compare the complication rates between IV and inhalational induction techniques. Although hypoxic arrest during the initial stages of anaesthesia and bronchoscopy does occur, we are not able to draw conclusions from the available literature whether choice of induction technique affects outcome. (1) Inhalational induction is preferred by most anaesthetists for the removal of FB’s in children.(14,16) Advantages of inhalational induction include; familiarity with its use in paediatric patients, avoidance of the need to attain IV access in the awake child, high success rate with maintaining spontaneous ventilation, haemodynamic stability Page 10 of 16 and the ability to titrate and quickly reverse the volatile once signs of airway obstruction appear. Inhalational induction also doesn’t appear to increase the risk of aspiration in these patients compared to IV induction.(12) Evacuating the stomach with a nasogastric tube after induction but prior to bronchoscopy is considered acceptable practice.(1)The optimal method of induction is not definitively established and probably does not change the outcome in the majority of cases (where FB’s are lodged distal to the carina). Maintaining spontaneous ventilation during the induction of a patient with a proximal FB is commonly practiced though.(1) After induction but prior to bronchoscopy the use of topical local anaesthesia is indicated in all cases, except when the condition of the patient is critical or when a local anaesthetic allergy exists. Lignocaine 1% (maximum safe dose is 4mg/kg) sprayed onto the larynx and into the trachea reduces the cardiovascular and tussive response to bronchoscopy.(12,14) It will allow a lighter level of anaesthesia to be tolerated during bronchoscopy, which is often the case with spontaneously breathing patients. b) Ventilation: SV or PPV? Considerable controversy exists as to how to conduct ventilation during rigid bronchoscopy.(14) It is difficult to demonstrate superiority of one type of ventilation technique over the other from the current literature. Both SV and PPV has been used successfully by various authors and it seems that there are no significant difference in major outcomes like mortality.(1,5,12,17) SV has the advantage of continued ventilation and oxygenation despite interruptions with the anaesthetic breathing circuit.(5) Although due to the underlying lung pathology (atelectasis and/or pneumonia) and high resistance to breathing through the bronchoscopes lumen the episodes and severity of desaturation is comparable between SV and PPV techniques.(18) The major disadvantage of SV is the high incidence of coughing and/or bucking during bronchoscopy because of inadequate depth of anaesthesia.(18) Traditionally it was thought that with the use of PPV, the FB can be pushed more distally making retrieval more difficult for the surgeon. The most feared complication is total proximal airway occlusion, was also thought to occur when PPV created a ball valve effect in the proximal airways preventing inspiration. These are overstated and unsubstantiated fears. If it is relevant, it remains a very rare phenomenon.(1,5,18) Most FB’s that require removal are lodged and PPV is unlikely to change the position. Because airway trauma and rupture are significant and potentially fatal complications the immobility of the patient during bronchoscopy is vital.(1) Adequate depth of anaesthesia so to render the patient immobile (without the use of muscle relaxants) is often not achieved with techniques that maintain SV. The significant conversion rate from SV to PPV during bronchoscopy to attain optimal surgical conditions (immobility) demonstrate this fact.(17,18) Page 11 of 16 Taking into consideration that two main goals are oxygenation and immobilization during bronchoscopy and the fact that PPV is often required to achieve these goals with a high success rate, its routine use cannot be frowned upon and should probably be investigated in larger prospective clinical trials. The use of muscle relaxants (mivacurium or suxamethonium) is the most reliable way of achieving immobility and is utilized most often on a “as needed” basis, but will commit the anaesthetist to the use of PPV.(1) SV during proximal airway FB’s (proximal to carina) is currently advocated.(1) PPV often result in leakage of air around the bronchoscope with inadequate ventilation. One way to overcome this problem is by manually closing the mouth and nose, although this will restrict the surgeon’s ability to manipulate the bronchoscope. (1) An alternative solution to this problem is the use of jet ventilation. Manual jet ventilation via a side port of the bronchoscope is described and was shown to have fewer episodes of hypoxaemia compared to PPV with a T-piece during FB retrieval.(19) Its use in children is not advocated, especially when experience with the use of it is lacking as barotrauma is a common complication.(12) Its use is valuable when inadequate oxygenation or ventilation during PPV cannot be achieved with the T-piece due to a significant leak around the bronchoscope. (c) Maintenance: Volatile or TIVA? Halothane was commonly used during bronchoscopy because of its ability to provide very deep inhalational anaesthesia during SV. The one major side effect was the high incidence of cardiac arrhythmias in these patients because halothane sensitizes the myocardium to catecholamines especially in the hypercarbic state as you would often find in patients with airway FB’s. (1) Sevoflurane has been shown in multiple trials to be similar in efficacy but has a much lower incidence of arrhythmias compared to halothane during bronchoscopy.(20) Traditionally only volatile anaesthetic agents were used for maintenance of anaesthesia during bronchoscopy for airway FB removal. Nowadays the use of total intravenous anaesthesia (TIVA) is becoming popular for these procedures due to the advantages it offers.(1) TIVA provides a constant depth of anaesthesia irrespective of ventilatory mode (SV or PPV), but also during manipulation of the bronchoscope in and out of the airways and there is also less theatre pollution with volatile anaesthetic.(1,5) The success of this technique to provide a haemodynamically stable and immobile patient depends on giving the correct dosage of IV drug and also operator experience with the technique. (21,22) There are several variations of IV drugs used (propofol, remifentanil, dexmeditomidine, midazolam) and combinations of these drugs described, but there is no clear evidence to suggest a superior drug or combination. Dosages in the range of 0.2 μg/kg/min of remifentanil and 100–250 μg/kg/min of propofol provide adequate surgical conditions.(21) Page 12 of 16 The ability to maintain SV with the use of a remifentanil infusion is described and together with the use of sevoflurane and topical local anaesthesia, it is an effective and save method to use during bronchoscopy.(23) (d) Pit falls during removal of the FB. Airway compromise is most likely during manipulation of the FB by the bronchoscopist. Dropping the FB during removal in the trachea or getting it stuck at the larynx is a complication that is well described and that have accounted for multiple intra-operative deaths.(1,12) Clear communication between surgeon and anaesthetist is vital during the period of removal of the FB. Incomplete vocal cord relaxation can contribute to the inability to remove the FB and immediate paralysis with the use of suxamethonium is then required. If ventilation suddenly becomes impossible during removal of the FB, the possibility of tracheal obstruction should be considered first. A dropped FB in the trachea needs to be either removed immediately or pushed back down the trachea into the same bronchus it was located in to provide ventilation. If the FB is displaced into the contra lateral bronchus (healthy lung) there is a possibility of complete airway obstruction and severe hypoxaemia due to oedema and inflammation at the original bronchial site.(1) In rare circumstances the inability to remove a FB can result in inadequate ventilation and will need to be optimized to provide oxygenation. Slow prolonged breaths with adequate pressure after endotracheal intubation can provide ventilation past a partially obstructed airway.(1) Extracorporeal membrane oxygenation can be a life saving modality if available during such cases.(24) POST-OPERATIVE CONSIDERATIONS Significant pulmonary compromise (hypoxaemia) and upper airway obstruction from laryngeal oedema should be anticipated after FB removal, especially in delayed presentations where bronchoscopy was difficult and prolonged. Nursing the child with the affected lung down can help prevent contamination of the unaffected lung. Supplemental oxygen and adrenalin nebulisation can be used post-operatively for airway oedema. Uncomplicated bronchoscopy and FB removal will allow the majority of patients to be discharged on the same day.(12) Predictive factors for a prolonged recovery period include the presence of infiltrates on preoperative CXR, delayed presentation, non resolving signs on post operative CXR and prolonged duration of bronchoscopy.(1) Page 13 of 16 CONCLUSION FB aspiration is common in children. A combination of a good history, physical examination and special investigations should eliminate the need for diagnostic rigid bronchoscopy as anaesthesia for this procedure is associated with significant morbidity and mortality. There is no consensus from the literature as to which anaesthetic technique is considered optimal. Keeping in mind the two main goals of oxygenation and patient immobility an individual plan for each patient based on FB type and location, surgeon preferences and personal familiarity with an anaesthetic technique must play a role in the final method chosen for anaesthesia. Clear communication and experienced team members are essential to a good outcome as intra-operative findings or events might significantly change the initial plans. Page 14 of 16 REFERENCES 1. Fidkowski CW, Zheng H, Firth PG. The Anesthetic Considerations of Tracheobronchial Foreign Bodies in Children: A Literature Review of 12,979 Cases. Anesth Analg. 2010;111(4):1016-25. 2. Clerf LH. Historical aspects of foreign bodies in the air and food passages. South Med J 1975;68:1449–54. 3. van As AB, du Toit N, Wallis L, Stool D, Chen X, Rode H. The South African experience with ingestion injury in children. International journal of pediatric otorhinolaryngology. 2003 12//;67, Supplement 1(0):S175-S8. 4. Kaushal P, Brown DJ, Lander L, Brietzke S, Shah RK. Aspirated foreign bodies in pediatric patients, 1968–2010: A comparison between the United States and other countries. International journal of pediatric otorhinolaryngology. 2011 10//;75(10):1322-6. 5. Zur KB, Litman RS. Pediatric airway foreign body retrieval: surgical and anesthetic perspectives. Pediatric Anesthesia. 2009;19:109-17. PubMed PMID: 42419849. 6. Tomaske M, Gerber AC, Stocker S, Weiss M. Tracheobronchial foreign body aspiration in children - diagnostic value of symptoms and signs. Swiss medical weekly. 2006 Aug 19;136(33-34):533-8. PubMed PMID: 16983595. Epub 2006/09/20. eng. 7. Hitter A, Hullo E, Durand C, Righini CA. Diagnostic value of various investigations in children with suspected foreign body aspiration: Review. European Annals of Otorhinolaryngology, Head and Neck Diseases. 2011 11//;128(5):248-52. 8. Tokar B, Ozkan R, Ilhan H. Tracheobronchial foreign bodies in children: importance of accurate history and plain chest radiography in delayed presentation. Clinical Radiology. 2004 7//;59(7):609-15. 9. Ikeda M, Himi K, Yamauchi Y, Ikui A, Shigihara S, Kida A. Use of digital subtraction fluoroscopy to diagnose radiolucent aspirated foreign bodies in infants and children. International journal of pediatric otorhinolaryngology. 2001 Dec 1;61(3):233-42. PubMed PMID: 11700193. Epub 2001/11/09. eng. 10. Weiliang B, Xinjia Z, Xin G, Chunbo S, Califano JA, Ha PK. Value of chest CT in the diagnosis and management of tracheobronchial foreign bodies. Pediatrics International. 2011;53(4):515-8. PubMed PMID: 65014031. 11. Hong SJ, Goo HW, Roh JL. Utility of spiral and cine CT scans in pediatric patients suspected of aspirating radiolucent foreign bodies. Otolaryngol Head Neck Surg 2008;138:576–80. 12. Farrell PT. Rigid bronchoscopy for foreign body removal: anaesthesia and ventilation. Pediatric Anesthesia. 2004;14(1):84-9. PubMed PMID: 11912232. 13. Rodríguez H, Passali GC, Gregori D, Chinski A, Tiscornia C, Botto H, et al. Management of foreign bodies in the airway and oesophagus. International Page 15 of 16 journal of pediatric otorhinolaryngology. 2012 5/14/;76, Supplement 1(0):S84S91. 14. Skinner A. Inhaled foreign body in children anaesthesia tutorial of the week 99. 2008 (08/07/2008); Available from: http://www.aagbi.org/sites/default/files/99-Inhaled-foreign-body-inchildren.pdf 15. Mani N, Soma M, Massey S, Albert D, Bailey CM. Removal of inhaled foreign bodies—Middle of the night or the next morning? International journal of pediatric otorhinolaryngology. 2009 8//;73(8):1085-9. 16. Kain ZN, O’Connor TZ, Berde CB. Management of tracheobronchial and esophageal foreign bodies in children: a survey study. J Clin Anesth 1994; 6:28–32. 17. Litman RS, Ponnuri J, Trogan I. Anesthesia for tracheal or bronchial foreign body removal in children: an analysis of ninety-four cases. Anesth.Analg. 2000; 91: 1389–1391. 18. Soodan A, Pawar D, Subramanium R. Anesthesia for removal of inhaled foreign bodies in children. Paediatric anaesthesia. 2004. Nov;14(11):947-52. PubMed PMID: 15500496. Epub 2004/10/27. eng. 19. Li S, Liu Y, Tan F, Chen J, Chen L. Efficacy of manual jet ventilation using Manujet III for bronchoscopic airway foreign body removal in children. International journal of pediatric otorhinolaryngology. 2010. Dec;74(12):1401-4. PubMed PMID: 20951443. Epub 2010/10/19. eng. 20. Batra YK, Mahajan R, Bangalia SK, Chari P, Rao KL. A comparison of halothane and sevoflurane for bronchoscopic removal of foreign bodies in children. Annals of cardiac anaesthesia. 2004 Jul;7(2):137-43. PubMed PMID: 17827546. Epub 2007/09/11. eng. 21. Teksan L, Baris S, Karakaya D, Dilek A. A dose study of remifentanil in combination with propofol during tracheobronchial foreign body removal in children. Journal of Clinical Anesthesia. 2013 5//;25(3):198-201. 22. Liao R, Li JY, Liu GY. Comparison of sevoflurane volatile induction/maintenance anaesthesia and propofol-remifentanil total intravenous anaesthesia for rigid bronchoscopy under spontaneous breathing for tracheal/bronchial foreign body removal in children. European journal of anaesthesiology. 2010 Nov;27(11):930-4. PubMed PMID: 20683333. Epub 2010/08/05. eng. 23. Sheng H, Dong H-l, Sun Y-y, Xiong D-f, Zhang H-p, Chen S-y, et al. Anesthesia with sevoflurane and remifentanil under spontaneous respiration assisted with high-frequency jet ventilation for tracheobronchial foreign body removal in 586 children. Pediatric Anesthesia. 2012;22(11):1100-4. PubMed PMID: 83751497. 24. Brown KL, Shefler A, Cohen G, DeMunter C, Pigott N, Goldman AP. Near-fatal grape aspiration with complicating acute lung injury successfully treated with extracorporeal membrane oxygenation. Pediatr Crit Care Med 2003; 4:243–5. Page 16 of 16