Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
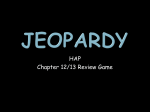
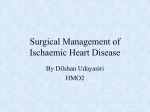
Indian Journal of Basic and Applied Medical Research; September 2014: Vol.-3, Issue- 4, P. 56-60 Case Report: Variations in the cystic and iliolumbar arteries with Psoas minor muscle 1Dr. 5Dr. Sibani Mazumdar, 2Dr. Susumna Biswas , 3Dr. Tridib Kumar, 4Sett Dr. Manotosh Banerjee , Barnali Mukherjee , 6Dr. Paramita Mukhopadhyay , 7Dr. Sudeshna Majumdar , 8Dr. Reshma Ghosh 1Professor and Head, Department of Anatomy, Calcutta National Medical College, Kolkata - 700014, West Bengal, India. 2Demonstrator, Department of Anatomy, Nilratan Sircar Medical College, Kolkata – 700014, West Bengal, India. 3Associate Professor, Malda Medical College and Hospital, Malda – 732101, West Bengal, India. 4Junior Resident, Department of Anatomy, Nilratan Sircar Medical College, Kolkata – 700014, West Bengal, India. 5Junior Resident, Department of Anatomy,KPC Medical College, Kolkata – 700032, West Bengal, India. 6Assistant Professor, 7Professor, Department of Anatomy, Nilratan Sircar Medical College, Kolkata -700014, West Bengal, India. Department of Anatomy, Nilratan Sircar Medical College, Kolkata -700014, West Bengal, India. 8Junior Resident, Department of Anatomy,Nilratan Sircar Medical College, Kolkata – 700014, West Bengal, India. Corresponding author: Prof. (Dr.) Sudeshna Majumdar Date of submission: 23 May 2014; Date of Publication: 15 September 2014 ABSTRACT The knowledge of multiple variations in peripheral blood vessels and muscles is important as these structures can be injured during a surgical procedure or regional anaesthesia. Some unusual clinical symptoms may arise due to these variations. While doing the routine dissection for MBBS Students, in the Department of Anatomy, NRS Medical College, Kolkata, India, few variations were found in abdomen of two male cadavers in December, 2013. In one cadaver, the cystic artery arose from the gastroduodenal artery. In the second cadaver, iliolumbar artery originated from the left common iliac artery and the psoas minor muscle was present on both sides. This case report will enhance our knowledge in gross and clinical anatomy. KEY WORDS: Hepatic artery, cystic artery, gastroduodenal artery, iliolumbar artery, psoas minor muscle INTRODUCTION cystic artery often varies. The most common variant According to normal anatomy, the hepatic artery, is an origin from the common hepatic artery, after its origin from the celiac axis, passes antero- sometimes from the left hepatic or gastroduodenal laterally to the upper border of the first part of the artery1. duodenum. It may be subdivided into the common The abdominal aorta bifurcates into right and left hepatic artery (from the coeliac trunk to the origin of common iliac arteries to the left side of the fourth the gastroduodenal artery), and the hepatic artery lumbar vertebral body. In addition to external iliac ‘proper’ (from the point of origin of gastroduodenal and internal iliac arteries each common iliac artery artery to its bifurcation into right and left hepatic also gives small branches to the peritoneum, psoas 1 arteries at the porta hepatis) . The cystic artery major, ureter, adjacent nerves and surrounding usually arises from the right hepatic artery and passes areolar tissue. Each internal iliac artery divides into anterior to the cystic duct and reaches the superior one anterior and one posterior trunk, behind the aspect of the neck of gallbladder to divide into superior margin of the greater sciatic foramen. superficial and deep branches. The origin of the Iliolumbar artery is usually the first branch of the 56 www.ijbamr.com P ISSN: 2250-284X , E ISSN : 2250-2858 Indian Journal of Basic and Applied Medical Research; September 2014: Vol.-3, Issue- 4, P. 56-60 posterior trunk of the internal iliac artery. It ascends muscle. On right side, the iliolumbar artery arose laterally anterior from the posterior division of the internal iliac artery to the sacroiliac joint and lumbosacral trunk to reach the medial border of the as usual. psoas major muscle where it divides into lumbar and Moreover, psoas minor muscle was present on both iliac branches. The common iliac artery occasionally sides in the posterior abdominal wall of the second 1 gives rise to Iliolumbar artery . cadaver. Both the muscles ended into long tendons Psoas minor is a muscle of the posterior abdominal in the lower part. wall. It is often absent, but when present, lies anterior to the psoas major. It arises from the bodies of the 12th thoracic and 1st lumbar vertebrae and from the disc between them. It ends in a long flat tendon attached to the pectineal line and ileopectineal eminence of the hip bone and laterally to the iliac fascia1. MATERIALS AND METHODS While doing the routine dissection for MBBS students in December, 2013, few variations were found in the abdomen of two male cadavers, in the Department of Anatomy, NRS Medical College of Figure – 1; The cystic artery (D) arose from the Kolkata, India. One subject was about sixty years old gastroduodenal artery (C) instead of the right hepatic and the other was about seventy years. Dissection artery (E), passed upwards and it inclined towards the was done properly in abdomen of the two cadavers. gallbladder (G) on right side. All the structures were observed minutely and Index: A – Common hepatic artery, B – Hepatic relevant photographs were taken. artery proper, C – Gastroduodenal artery, OBSERVATIONS D - Cystic artery, E – Right hepatic artery, F – Left In the first cadaver, the cystic artery arose from the hepatic artery, G – Gallbladder, gastroduodenal artery instead of the right hepatic artery, passed upwards to the right side and it H – Liver, I – Common bile duct, J– Ist part of the duodenum. inclined towards the cystic duct and gall- bladder. The hepatic artery proper divided into right and left hepatic branches below the porta hepatis, before running into the liver parenchyma as usual. Medworld asia In the second cadaver, the left iliolumbar artery originated from the left sided common iliac Dedicated for quality research artery (instead of the posterior division of the internal iliac artery). Then it divided into iliac and lumbar arteries reaching the medial border of the psoas major 57 www.ijbamr.com P ISSN: 2250-284X , E ISSN : 2250-2858 Indian Journal of Basic and Applied Medical Research; September 2014: Vol.-3, Issue- 4, P. 56-60 Index: A- Left psoas major muscle, B - Left kidney, C – Left ureter, D - Abdominal Aorta, E - Left common iliac artery, F - Left lateral femoral cutaneous nerve. DISCUSSION The cystic arteries vary markedly in regard to the arterial stem from which they arise. A cystic artery arise from a source other than the right hepatic artery in about 10% of the bodies2,3. Daseler et al (1947) Figure – 2; In the second cadaver, the left iliolumbar found in their study that in 85-90% cases cystic artery artery (A) originated from left the sided common arose from the right branch of the hepatic artery and iliac artery (B) and it divided into two branches in 2.5% cases from the gastroduodeanal artery3. reaching the medial border of psoas major (C). According to Hollinshead (1971), this artery may arise from the aberrant right hepatic artery, the left hepatic artery (in about 5% cases or more), branches of the coeliac trunk, or even from the superior mesenteric artery4. Bergman et al stated that the cystic artery may arise from the downward-directed vessel, the gastroduodenal artery, or its branch, the superior pancreaticoduodenal artery. Origin from the more distant source is far less common (0.3%) than Figure – 3; Right sided psoas minor muscle (lying on the belly of psoas major muscle) was held with forceps. the nearer (2.6%) 5. Pushpalatha et al (2010) found in their study Index: A – Right psoas major muscle, B – Right that the cystic artery arose from the right hepatic kidney, C – Right lateral femoral cutaneous nerve, D – artery in 54% cases, from the hepatic artery proper in Right ureter, E – Abdominal Aorta, F – Right common 22% cases, from the common hepatic artery in 12% iliac artery. cases, from the gastroduodenal artery in 8% cases, from the superior mesenteric artery in 2% cases and from the accessory hepatic artery in 2% cases6. In another study, among 150 cases, cystic artery arose from the right branch of the hepatic artery proper in 147 (98%) cases and from the gastroduodenal artery in 3 (2%) cases (including a case of double gallbladder) 7. According to another recent study most common source of origin of the cystic artery Figure – 4; Left sided psoas minor tendon (lying on was the right hepatic artery in 92% cases, followed the belly of psoas major muscle) was held with by aberrant right hepatic artery in 4% cases, the left forceps. 58 www.ijbamr.com P ISSN: 2250-284X , E ISSN : 2250-2858 Indian Journal of Basic and Applied Medical Research; September 2014: Vol.-3, Issue- 4, P. 56-60 hepatic artery in 1% case and the gastroduodenal 8 of the femur or lesser trochanter with psoas major11. artery in 1% case . Knowledge of cystic artery variability, as revealed from may end on the iliac fascia, inguinal ligament, neck facilitates the second part lying deep to the first. A subdivision intraoperative identification of vessels in both or splitting of its tendon may occur with one part classical cholecystectomy or going to the fifth lumbar and the first sacral surgery of bile ducts. Uncontrolled bleeding from vertebrae, and the second going to the iliopectineal cystic artery and its branches may increase the risk of line. This was also observed that this muscle had lesions to vital vascular and other structures during been replaced by a tendon or its insertion lost in the hepatobiliary surgery and also during other upper pelvic fascia12.The psoas minor muscle has been abdominal surgeries like resection of pancreas 6, 9. clinically ignored as a functional hip flexor. Patient and different laparoscopic studies, According to Macalister this muscle may be doubled, The Iliolumbar artery, though it is usually the complaints of pain in the anterior inguinal area first branch of the posterior division of the internal during psoas minor strain which will interfere with iliac artery, may be absent, reduced in size, or their ability to run, jump or rotate on hip joint13. partially replaced by one of the lumbar arteries. It CONCLUSION occasionally gives rise to a lateral superior sacral This case report with variant anatomy of the cystic artery10. It has been occasionally seen as a branch of artery may be of help for the surgeons to minimize the common iliac, one lumbar, middle sacral and the the risk of haemorrhage and injury to vital structures lateral sacral including biliary apparatus during upper abdominal arteries 1,10. surgeries like cholecystectomy 6,8 . The variation in Psoas minor muscle is not constant in the iliolumbar artery and the presence of psoas minor humans. In a report of 182 subjects it was present on muscle are also important for surgery in the posterior both sides in 70 subjects, on the right side in 12, on abdominal wall. Psoas minor strain has importance in the left side in 8, and absent on both sides in 92 Sports Medicine. subjects. Various sources report that the muscle is ACKNOWLEDGEMENT 11 present in about 56% of bodies . When present, the We are grateful to all the members of the Department muscle varies considerably in its site of origin. It may of Anatomy, Nilratan Sircar Medical College, be connected only with the first lumbar vertebra, or Kolkata –14, West Bengal, India, for their cordial with the second lumbar and intervertebral disc (above help to complete this case report. it) or it may arise from two heads. At its insertion it REFERENCES 1. Standring S, Collins P, Healy JC, Borley NR, Wigley C, Brown JL, Khan N, Moore LA (editors). In : ‘Gray’s Anatomy, The Anatomical Basis of Clinical Practice’: Posterior Abdominal Wall and Retroperitoneum; The pelvis, pelvic floor and perineum; Liver; Gallbladder and biliary tree. 40th Edition. Spain, Churchill Livingstone Elsevier. 20011; 1071-72, 1086 - 87, 1169-70, 1179-80. 2. Micheles NA. Collateral Pathways to the liver after ligation of hepatic artery and removal of coeliac axis. Cancer.1953; 6:708. 59 www.ijbamr.com P ISSN: 2250-284X , E ISSN : 2250-2858 Indian Journal of Basic and Applied Medical Research; September 2014: Vol.-3, Issue- 4, P. 56-60 3. Daseler EH, Anson BJ, Humbly WC, Riemann AF. The cystic artery and constituents of the hepatic pedicles: A Study of 500 specimens. Surgery, Gynaecology and Obstetrics. 1947; 85: 47. 4. Hollinshead WH. Anatomy for Surgeons; In the Liver and Gallbladder. 2nd Edition, Volume 3. Harper & Row, Publishers, Inc., New York, San farncisco, London. 1971; 338-356 (s). 5. Bergman RA, Afifi AK, Miyauchi R. Illustrated Encyclopedia of Human Anatomic Variation: Opus II: Cardiovascular System: Arteries: Abdomen: Variations in Branches of Celiac Trunk: Cystic artery. Viewed from http://www.anatomyatlases.org/AnatomicVariants/Cardiovascular/Text/Arteries/Cystic.shtml (accessed in July, 2014) 6. Pushpalatha K, Shamasundar NH. Variation in the Origin of the Cystic Artery. Journal of Anatomical Society of India. 2010; 59(1) 35-37. 7. Gupta I, Majumdar S, Chakraborty P, Ghosh S. A Study on the Anomalies of Gallbladder and associated Structures. J.Anat.Soc.India. 2012; 61(2) 205-213. 8. Tejaswi HL, Dakshayani KR, Ajay N. Prevalence of anatomical variations of cystic artery in South Indian cadavers. Int J Res Med Sci. 2013; 1(4): 424-428. 9. Patil S, Rana K, Kakar S, Mittal A. Origin of cystic artery from hepatic artery proper and its surgical implications. Int J Res Med Sci. 2013; 1(1): 16- 18. 10. Bergman R A, Afifi A K, Miyauchi R. Illustrated Encyclopedia of Human Anatomic Variation: Opus II: Cardiovascular System: Arteries: Pelvis: Iliolumbar Artery. Viewed from http://www.anatomyatlases.org/AnatomicVariants/Cardiovascular/Text/Arteries/Pelvis.shtml (accessed in July, 2014) 11. Bergman R A, Afifi A K, Miyauchi R. Illustrated Encyclopedia of Human Anatomic Variation: Opus I: Muscular System: Alphabetical Listing of Muscles: P. Psoas Minor. Viewed from http://www.anatomyatlases.org/AnatomicVariants/MuscularSystem/Text/P/Psoas.shtml (accessed in July, 2014) 12. Macalister A (1875). Observations on muscular anomalies in the human anatomy. Third series with a catalogue on the principal muscular variations hitherto published. Trans. Roy. Irish Acad. Sci. 25:1-130. 13. Psoas minor strain. Sports Medicine and Rehabilitation. International Bradenton. FL 941.755.8819. Accessed in July, 2014. 57 60 www.ijbamr.com P ISSN: 2250-284X , E ISSN : 2250-2858