Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
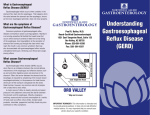
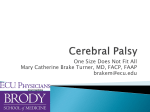
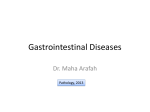
Reflux of Contrast Medium into the Inferior Vena Cava on Computerized Tomographic Pulmonary Angiography Alerting for Cardiac Diseases Poster No.: C-0702 Congress: ECR 2012 Type: Scientific Exhibit Authors: G. Aviram, D. Cohen, A. Steinvil, S. Berliner, O. Rogowski; TelAviv/IL Keywords: Hemodynamics / Flow dynamics, Diagnostic procedure, CTAngiography, Thorax, Cardiac DOI: 10.1594/ecr2012/C-0702 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 16 Purpose The aim of the present study was to investigate the prevalence, severity, associated diagnoses and eventual prognostic significance of reflux of contrast medium into the IVC in a large cohort of patients who underwent CTPA. The number of computerized tomographic pulmonary angiographic (CTPA) examinations performed for evaluating patients presenting with acute dyspnea has been growing exponentially during recent years, with a relatively low prevalence (sometimes even less than 10%) of findings consistent with the suspected diagnosis of acute pulmonary 1 embolism (PE) . Reflux of contrast medium from the right atrium to the inferior vena cava (IVC) and hepatic veins during the first pass of the injected bolus of contrast medium is often present on CTPA. Only a few preliminary small series have described this finding in association with right heart failure 2-5 . The aim of the present study was to investigate the prevalence, severity, associated diagnoses and eventual prognostic significance of reflux of contrast medium into the IVC in a large cohort of patients who underwent CTPA. We considered that these imaging findings might serve as a pathophysiological marker of right heart dysfunction, thus tapping information obtained by the radiologist to help explain the patient's clinical presentation. Images for this section: Page 2 of 16 Fig. 1: Example of a severe refulx of contrast on CT pulmonary angiography Page 3 of 16 Methods and Materials Study population We evaluated 1065 consecutive CTPA studies performed in 1027 patients between January 1, 2007 and January 7, 2008. The patients' chartsgender and age, were reviewed for the reason for referral to CTPA scan, final diagnoses during the index hospitalization, background and co-morbid conditions. Information on mortality was collected from the database of the country's Ministry of Internal Affairs. CT Acquisition All study patients were scanned by a multi-detector CT scanner with 16 or 64 detector rows, according to our routine non-electrocardiographic (ECG)-gated PE protocol , with injections of contrast medium comprised of 80-100 mL of iodinated contrast material at rates of 3-4 mL/sec. All scans were obtained in a caudal-cranial direction covering the chest from the lung bases to the thoracic inlet at end-of-inspiration during a single breath#hold. CT Assessment The CT scans were reviewed by two radiologists who were unaware of the patient's clinical history, results of other imaging techniques, and outcome. The severity of reflux of contrast medium into the IVC and the hepatic veins was graded 5 from the axial images on a scale of 1-6 as described by Groves et al . (Fig. 2-7): 1 = no reflux into the IVC, 2 = a trace of reflux into the IVC only, 3 = reflux into the IVC but not the hepatic veins, 4 = reflux into the IVC and opacifying the proximal hepatic veins, 5 = reflux into the IVC and opacifying mid#part of the hepatic veins, and 6 = reflux into the IVC and opacifying the distal hepatic veins. These six grades of reflux were reduced to three groups for statistical analyses: no reflux (grade 1), mild reflux (grades 2-3) and extensive reflux (grades 4-6). Grading of reflux of contrast medium into the IVC was performed separately by the two radiologists in the first 500 consecutive CTPA in order to assess interobserver variation. Statistical Analysis Data were summarized as mean±standard deviation (SD) for continuous variables, and as number of individuals for categorical variables. These clinical data and mortality data were correlated with the severity of reflux. Kappa was calculated in order to measure agreement between the two independent observers for grading the extent of reflux. Comparison of frequencies between the groups of reflux grades was by chi- Page 4 of 16 square statistics. Univariate and multivariate logistic regression models were used to calculate the odds ratio (OR) for having extensive reflux in each diagnosis. We used Cox proportional hazard models to evaluate the hazard ratios (HR) of severe reflux for the outcome of mortality. All the above analyses were considered significant at P<0.05 (two-tailed). The SPSS statistical package was used to perform all statistical evaluations (SSPS Inc., Chicago, IL, USA). Images for this section: Fig. 2: Reflux grade 1 = no reflux into the IVC Page 5 of 16 Fig. 3: Reflux grade 2 = a trace of reflux into the IVC only Page 6 of 16 Fig. 4: reflux grade 3 = reflux into the IVC but not the hepatic veins Page 7 of 16 Fig. 5: Reflux grade 4 = reflux into the IVC and opacifying the proximal hepatic veins Page 8 of 16 Fig. 6: Reflux grade 5 = reflux into the IVC and opacifying mid part of the hepatic veins Page 9 of 16 Fig. 7: Reflux grade 6 = reflux into the IVC and opacifying the distal hepatic veins Page 10 of 16 Results The final study group included 967 CTPA scans of 367 males (38%) and 600 females (62%) whose mean age was 62±20 years (range 17-103). The two most common reasons for referral were symptoms of dyspnea and/or low oxygen saturation (763 CTPA, 76.1%) and chest pain (116 CTPA, 11.6%). PE was diagnosed in 17% of patients, while infection and oncologic diseases were the most frequent acute final diagnoses, (Table 1). There were 480 patients (49.6%) with no evidence of reflux (grade 1), 310 (32.1%) with mild reflux (grade 2-3), and 177 (18.3%) with extensive reflux into the IVC and the hepatic veins (grade 4-6). Tables 2-4 present the number and percentage of the individuals with each grade of reflux and the age-adjusted odds ratio (OR) and 95% confidence interval (CI) for having extensive reflux for each diagnosis. Advanced age, most cardiac diagnoses and obesity were associated with an increased prevalence and odds for having extensive reflux. On the other hand, none of the pulmonary diagnoses were associated with extensive reflux, while an oncologic diagnosis was associated with low prevalence of reflux. Table 5 presents the multivariate logistic regression model: pulmonary hypertension, a history of congestive heart failure (CHF), chronic atrial fibrillation (CAF), and acute PE had significant independent associations with extensive reflux. Three-hundred fifty-nine (37.1%) patients died during a median follow-up of 40 months (range 0-50 months) following the performance of the CTPA scan. Mortality analysis using Cox proportional hazard models revealed that a reflux grade of 4-6 was associated with increased mortality, with a crude HR (95% CI) of 1.42 (1.10 1.83), P=0.007. The multivariate analysis, however, showed that this association was non-significant following adjustment for age. As such, a grade 4-6 reflux is not an independent predictor of mortality, but rather a finding which is associated with morbidity that is more prevalent in older patients. Interobserver agreement between the two readers for reflux grading was good (kappa=0.77). Page 11 of 16 Images for this section: Table 1: The baseline characteristics of the study cohort, including final diagnoses during the index hospitalization, background and co-morbid conditions Table 2: Reflux grade and odds ratio for extensive reflux according to age, gender and PE status Page 12 of 16 Table 3: Reflux Grade According to Patients' Cardiac Diagnoses Table 4: Reflux Grade According to Patients' Non-Cardiac Diagnoses Page 13 of 16 Table 5: Logistic Regression for Extensive Reflux of Age, Gender, Obesity and Pulmonary Embolism Status Page 14 of 16 Conclusion Pulmonary hypertension, CHF, CAF, and PE emerged as being the most frequent diagnoses associated with the highest grade of reflux. The common denominator of all these diagnoses is the possible existence of congestion at the entrance to the right atrium. The primary contribution of the present study is the singling out of cardiac conditions as the main determinants of contrast medium reflux into the IVC as opposed to a relatively large number of other clinical conditions, including pulmonary diseases, which can be encountered in a population of patients who have signs and symptoms justifying their referral to CTPA We postulate that the contrast column created by the reflux to the IVC can serve as a radio-physiological measure similar to jugular venous pressure assessment on physical examination. As such, it can alert clinicians to the presence of congestion at the entrance to the right atrium which is producing the backflow of contrast material into the IVC. References 1. Mamlouk MD, vanSonnenberg E, Gosalia R, Drachman D, Gridley D, Zamora JG, Casola G, Ornstein S. Pulmonary embolism at CT angiography: implications for appropriateness, cost, and radiation exposure in 2003 patients. Radiology 2010;256:625-632. 2. Holley HC, Koslin DB, Berland LL, Stanley RJ. Inhomogeneous enhancement of liver parenchyma secondary to passive congestion: contrast-enhanced CT. Radiology 1989;170:795-800. 3. Collins MA, Pidgeon JW, Fitzgerald R. Computed tomography manifestations of tricuspid regurgitation. Br J Radiol 1995;68:1058-1060. 4. Yeh BM, Kurzman P, Foster E, Qayyum A, Joe B, Coakley F. Clinical relevance of retrograde inferior vena cava or hepatic vein opacification during contrast-enhanced CT. AJR Am J Roentgenol 2004;183:1227-1232. 5. Groves AM, Win T, Charman SC, Wisbey C, Pepke-Zaba J, Coulden RA. Semiquantitative assessment of tricuspid regurgitation on contrast-enhanced multidetector CT. Clin Radiol 2004;59:715-719. Page 15 of 16 6. Shapira Y, Porter A, Wurzel M, Vaturi M, Sagie A. Evaluation of tricuspid regurgitation severity: echocardiographic and clinical correlation. J Am Soc Echocardiogr 1998;11:652-659. 7. Dusaj RS, Michelis KC, Terek M, Sanai R, Mittal R, Lewis JF, Zeman RK, Choi BG. Estimation of right atrial and ventricular hemodynamics by CT coronary angiography. J Cardiovasc Comput Tomogr 2011;5:44-49. 8. LaBounty TM, Glasofer S, Devereux RB, Lin FY, Weinsaft JW, Min JK. Comparison of cardiac computed tomographic angiography to transesophageal echocardiography for evaluation of patients with native valvular heart disease. Am J Cardiol 2009;104:1421-1428. 9. Ghaye B, Ghuysen A, Willems V, Lambermont B, Gerard P, D'Orio V, Gevenois PA, Dondelinger RF. Severe pulmonary embolism:pulmonary artery clot load scores and cardiovascular parameters as predictors of mortality. Radiology 2006;239:884-891. 10. Aviram G, Rogowski O, Gotler Y, Bendler A, Steinvil A, Goldin Y, Graif M, Berliner S. Real-time risk stratification of patients with acute pulmonary embolism by grading the reflux of contrast into the inferior vena cava on computerized tomographic pulmonary angiography. J Thromb Haemost 2008;6:1488-1493. Personal Information Corresponding author: Galit Aviram, MD, Department of Radiology, Tel Aviv Medical Center, 6 Weizman Street, Tel Aviv 64239, Israel. Telephone: +972#3#6973504, Fax: +972#3#6974659, E#mail: [email protected] Page 16 of 16