Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Maternal health wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Health system wikipedia , lookup
Epidemiology wikipedia , lookup
Social determinants of health wikipedia , lookup
Reproductive health wikipedia , lookup
Public health genomics wikipedia , lookup
Health equity wikipedia , lookup
Preventive healthcare wikipedia , lookup
Race and health wikipedia , lookup
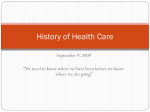
IS THE AGEING POPULATION A THREAT TO SUSTAINABLE HEALTH CARE? The Good News: We Are Living Longer Professor Raymond Tallis, Professor of Geriatric Medicine, University of Manchester British Association for the Advancement of Science September 2003 Let us begin with some extraordinary statistics. Global life expectancy has more than doubled over the last 140 years. Nearly two thirds of the increase in longevity in the entire history of the human race has occurred since 1900. If we confine ourselves to England and Wales the news remains pretty extraordinary. While in 1901 37% of all deaths occurred between 0 and 4 years of age and only 12% over the age of 75, in 1999, only 0.8% of deaths were under the age of 4 and 64% were over the age of 75. In the second half of the century (and the first 50 years of the NHS) infant mortality fell from 39/1000 to 7/1000 for girls and from 30/1000 to 5/1000 for boys and the proportion of people dying before reaching 65 from 40% to 7%.Life expectancy at birth increased by nearly a decade from 66 to 74.5 for men and from 70.5 to just under 80 for women. Much of this may be attributed to factors beyond medicine narrowly understood: increasing prosperity, better nutrition, education, public hygiene, housing, health and safety at work, technological advances fuelling increases in economic output, the emergence of liberal democracies protecting individuals against exploitation and abuse, and social welfare policies. Even so, medicine in the narrow sense has played a key role, as shown by the fact that life expectancy has continued to rise sharply long after public health measures and social policies have been fully in place: life British Association for the Advancement of Science September 2003 Raymond C Tallis 1 expectancy at birth increased in the last two decades of the 20th century by 4.7 years for men and 3.5 years for women. Male life expectancy at age 65 in England and Wales increased from from just under 12 years to just under 15 years between 1970 and 1995 - a little more than in the whole period from 1900 to 1970. (Similarly cheerful figures apply to females.) The percentage of people in England and Wales surviving to 85 more than doubled in males from 11.4 to 24.2 and in females from 27 to 41. Does Longer Life Mean More Illness? That the majority of people are enjoying a full life span would, one might think, be cause for rejoicing. Many commentators, however, including some who are themselves old, see the ageing of the population as a near disaster. For over 25 years, there has been talk of "the failures of the success" of medicine. Underpinning this view is the belief that increased life expectancy is almost inevitably bought at the cost of increased burden of disease. Is this the case? There are reasons for believing this might be so. First, most chronic disabling diseases have an almost exponential relationship to age: stroke, Parkinson’s disease, dementia, osteoarthritis, chronic respiratory problems, cardiac disease - to take just a few - show this relationship. For example, the chances of being disabled from a stroke increase nearly 100-fold between age 45 and age 85. A survey published by the Office of Populations Censuses and Surveys (OPCS) in 1988 confirmed this exponential relationship between chronic disability and increasing age. Most alarmingly, given that the greatest proportionate increases in the population are British Association for the Advancement of Science September 2003 Raymond C Tallis 2 anticipated in the over 75s, the curve flicks up sharply at around aged 75. The OPCS data are guite old, referring to a population studied in the middle 1980s. Since then, some surprising things have happened. First of all, what everyone knows has been officially acknowledged: the vast majority of people in later life enjoy excellent health or have health problems that are sufficiently under control not to be a barrier to the enjoyment of a full life. The consequence of this is that "a fresh map of life" has had to be drawn. Added years are not being bought simply at the cost of added troubles. 1. Disability Trends in the UK There are now some good data, on the basis of the General Household Survey and other studies, about trends in disability in older people in the United Kingdom, in particular the oldest old. The proportion of men over 85 able to bathe, feed and get to the toilet without help, rose from 69% to 79% between 1980 and 1991 and the proportion of women rose even faster - from 64% to 80%. Conversely, the proportion of years of life over 85 spent independent in activities of daily living rose between 1980 and 1991 from 69% to 80% for men and from 67% to 82% for women. The longer term trends are even more impressive; for example the proportion of men over the age of 85 unable to perform 4 activities of daily living fell from 45% in 1976 to 18% in 1994. 2. Disability and Chronic Ill Health in USA There are equally encouraging data from the United States of America, where accountants have a firmer grip on healthcare and on who needs what billable item. Manton’s longitudinal studies on disability at different ages in the USA have shown that a) the populatio n is living British Association for the Advancement of Science September 2003 Raymond C Tallis 3 longer and b) that the prevalence of disability at each age is falling. Even more cheering is the finding that the rate of fall of age-adjusted prevalence of disability and chronic ill health is accelerating and has continued to the present. Particularly gratifying are the marked declines in the age-adjusted risk of dementia. Manton’s data are based upon several millions of subjects. The trends are due largely to a decline in the incidence and prevalence of conditions such as stroke and chronic heart disease. 3. Health Expenditure: UK The use of hospital services, in particular in-patient stay, is another marker of serious ill health in old age. Here, too, the facts are surprisingly cheering. In a carefully designed study, Himsworth examined the number of days spent in hospital in the last 15 years of their life by people who died at different ages. The total days of in-patient care for people who died at 90 was only about double that of people who died at 45; and there was hardly any difference at all when people who died in their 70s were compared with those who died in their 90s: the extra 20 years of life was not bought at the cost of an extra 20 years in hospital ! 4. Health Expenditure: USA Studies in the USA of Medicare expenditure are equally encouraging. Lubitz and others found that the average Medicare expenditure for those who died at 70 was $35,000 compared with $65,000 for those who died at 100+. This looks worrying until one realises that, since Medicare begins at 65, the average yearly expenditure is $7,000 dollars for those who died at 70 compared with $1,800 for the centenarians. The very long-lived get years of extra life more cheaply: in this, as in so many other things, there are economies of scale! Moreover, the notion that increasing amounts of money are spent in futile attempts to keep people alive in what turns out to be their last year is also unfounded. As Henry Shenkin has pointed British Association for the Advancement of Science September 2003 Raymond C Tallis 4 out, there is no evidence that medical care in the last year of life is becoming more aggressive, more expensive, or more highly technological. Firstly, the proportion of total Medicare dollars spent on individuals remained stable in the 12 year period between 1976 and 1988, despite rapid technological advances; moreover, the payments in the last two months of life, proportionally, did not increase. Secondly, only about 3% of those Medicare beneficiaries who die incur the very high costs suggestive of aggressive care at life's end. (This fits with the fact that dying in great old age is a less brutal and hard business.) Such increases as have incurred in health care expenditure in old age overall simply reflect the availability of new treatments, the appropriate expectation of older people that they will benefit from them, and their increased access to them. In sum, while the total volume of need for health care has increased, age-specific healthcare requirements, like age-specific disability rates, have fallen and are continuing to fall. The improved quality of life in old age goes beyond gross markers of health gains. Older people have access to more resources than their predecessors: more nutritious food, better housing, and more user-friendly technologies such as mobile phones and body worn alarms, and a variety of sources of home entertainment (To vary Shakespeare, "Our little life is rounded with a soap"). These goods, however, are inequitably distributed; and individuals who have been socially deprived in earlier years will often be doubly jeopardised in old age being more likely to be malnourished, underheated and subject to a variety of restrictions. (The social gradients of health and life expectancy in Britain, and the key role of poverty in determining health, are true, not tabloid, scandals that, after decades of political British Association for the Advancement of Science September 2003 Raymond C Tallis 5 denial, are now fully accepted.) But for the majority of old people, life has never been so good. Things Could Get Even Better The optimistic tone of what has just been said may provoke disbelief. Surely the longer people live, the more chance they have of becoming "a burden" or (more politely) "a challenge" – to themselves, to their friends and relatives who find themselves transformed into (willing or unwilling) carers, to the NHS and social services and to the economy as a whole. Do not old people cost money, time, effort, patience - and all in the aid of sustaining them through a miserable existence ? And is there not ubiquitous evidence of this burden placed on society by old people: hospitals overrun by gravely ill octogenarians who survive a five days wait on a trolley in casualty only to be readmitted again and again; harrowing tales of carers crushed by the demands of caring; panic in the Treasury as health and social care budgets spiral out of control? The dissociation between the public perception of old age and reality of life as an old person should perhaps occasion no surprise. Even so, the extent of the dissociation is arresting. The debate is highly negative: gloomy about the present and doomy about the future, it foccuses on the pressures on the health service, the coming crisis in the economy and the need to liberalise the laws relating to euthanasia. Meanwhile the vast majority of old people are in good health and enjoying a quality and style of life that their predecessors (at any age) would have found unimaginable. The amount of time that older people spend waiting in A&E departments on hospital trolleys is of course outrageous and the more uncomfortable it makes government ministers the British Association for the Advancement of Science September 2003 Raymond C Tallis 6 better (so long as it does not prompt more targets and quick fixes that unfix other things). But this is a tip to which an iceberg of the wrong size is attached. The number of old people on trolleys in hospitals is a very inaccurate measure of the underlying health of the older population - after all, even the unfortunate minority spend only a very small part of their later years in this position. It is not even a measure of the demands (or the per capita demands) made by older people on health care services. At best it reflects the discrepancy between the demand for one sort of health care and the capacity to meet that demand. The pressure on hospitals, that is felt particularly acutely in A&E departments, is a measure less of the deteriorating health of an ageing population than of rising expectation of care (i.e. of good health) and the increasing ways that are available to meet those expectations. The failure to meet that pressure is almost wholly due to the wilfully ill-informed decimation of hospital beds over the last few decades. (It has been belatedly discovered that medical care cannot always be given to patients in the standing position.) At any rate, it tells us nothing about what being old is generally like and less than nothing about what it might be like in future. Moreover, further advancements are possible. Health throughout life can be improved by simple "lifestyle" measures: increased exercise, weight control, drinking in moderation, and stopping smoking. There is better understanding of how health promotional activities can themselves be promoted. There is even more potential for beneficial intervention in patients who are at high risk for various chronic disabling diseases, such as stroke, the commonest cause of severe disability in old age. We now know how to prevent over a half of strokes, by measures such as controlling high blood pressure, adequately treating high blood sugar and raised cholesterol, British Association for the Advancement of Science September 2003 Raymond C Tallis 7 giving aspirin for people at high risk and anticoagulants for people with certain cardiac arrhythmias and yet very many who could benefit from treatment of these risk factors do not receive them. Again and again, researchers find that the "rule of halves" applies: half of those who have the risk factor (such as high blood pressure) are not aware of it; half of those in whom it is detected are not treated; and half of those who are treated are not treated adequately. Here, then, is a huge amount of slack to take up. Universal availability of a ‘polypill’ of blood pressure medications, aspirin, folic acid and fat-lowering drugs – all in modest enough quantities to cause few side effects – could reduce heart attacks as well as stroke by 80%. We may be equally optimistic about improvement in our management of conditions that are not prevented or preventable. New strategies for the treatment of conditions such as Parkinson’s disease and Alzheimer’s disease will come from a deeper understanding of the underlying mechanisms; ‘end of pipe’ solutions, such as the use of cholinesterase inhibitors for Alzheimer’s dementia – which already afford modest but worthwhile gains – will be supplanted by much more potent treatments that address the problem further up the causal chain; and more precise diagnosis and subtyping of conditions will enable tailored treatments to be given earlier in the course of the disease before secondary adverse events, with a progressive, self-fuelling shrinkage of the patient’s life space, occur. Even if these new treatments do not materialize – and there have been many disappointments, for example in attempts to repair chronic neurological damage or limit the havoc caused to the nervous system by acute stroke - there are still huge gains to be made from optimising the use of the treatments that are already British Association for the Advancement of Science September 2003 Raymond C Tallis 8 available. There have been numerous studies (including those of my own group), which have shown that older patients are often give inappropriate (and not infrequently contraindicated or adversely interacting) drugs, sometimes in wrong doses (too low or too high) and that, even where the correct drugs are prescribed in appropriate doses, they are not taken because of a lack of concordance of views between doctor and patient. The new science of pharmacogenomics (using genetic profiling to tailor treatment to the individual rather than to the disease alone) will increase the number of people able to benefit from treatments and reduce the number of nasty surprises from hitherto unpredicted adverse effects. Gentler, more sophisticated health technologies for both diagnosis and treatment, suitable for older and frailer people are or already available - for example scans rather than "open up and see" surgery for diagnosis; and minimally invasive techniques such as angioplasy for coronary artery disease – and are extending the range of people who can benefit. Even where the underlying biology of a disabling chronic disease cannot be addressed, there is now increasing understanding of the extent to which recovery is possible, given the right environment and the right inputs. This is particularly true of degenerative diseases causing damage to the brain - possibly the single greatest scourge of old age. New techniques have shown how the "so ft-wired" nervous system is able to reorganise on a microscopic and macroscopic scale, to bring about dramatic improvements, and how those improvements may be promoted. Other techniques, such as the use of stem cells and synthetic nerve growth factors are, after many years of disappointment, looking increasingly likely to deliver on the hopes that British Association for the Advancement of Science September 2003 Raymond C Tallis 9 have been invested in them, in the next decade. I could go on; noting, for example, that people are entering old age in generally better health (so there is more capacity to withstand disease when it strikes), due to better nutrition, health and safety at work and education in the years leading up to old age and to improved intra-uterine health (one of the major determinants of illness in later life); or that the wide availability of labour-saving devices, of communications systems and user-friendly efficient methods of domestic heating and lighting, will make it less likely that impairments will translate into frustrating disability and dependency. But I have probably said enough to support my contention that the present for more people in old age - at least in developed countries – is good and the future likely to be even better. A progressive improvement in the quality of old age, in which the health span of a long life gradually approximates the life span, is feasible. Squaring the Circle The pre-eminent medical historian, the late Roy Porter, worried that the "ignominious destiny" of medicine in the future would be "bestowing meagre increments of unenjoyed life". Since the age of premature death from infectious diseases has given way to the age of chronic disorders, he argued, doesn't longer life mean more time to be ill? How do we explain how long life is not associated with prolonged illness? The answer lies in the ageing process, which explains the extremely cheerful and seemingly paradoxical findings that people are living longer and yet enduring, on average, shorter periods of ill health before death. To understand this, we need to fo rm a clearer idea of the consequences of ageing for the organism as a whole. British Association for the Advancement of Science September 2003 Raymond C Tallis 10 Ageing has been defined as "a progressive, generalized impairment of function" which results in "an increased probability of death". In order to see how the former leads to the latter, we need to understand the notion of the "adaptive capacity" of an organism. Nearly 150 years ago, Claude Bernard enunciated the principle that, for higher organisms at least, the condition of life was the constancy of the internal environment. Survival depends on the exquisite regulation of a vast number of parameters: blood pressure, levels of electrolytes, sugar and a variety of other substances in the blood, body temperature, the total amount of fluids in the different body compartments; and so on. The capacity to hold these parameters steady, so that organs can perform their functions (some of which are to regulate these parameters), was later called "homoeostasis". Although these regulatory mechanisms can cope with most of the contingencies of everyday life, they have their limits. While the body can adapt to a hot climate and water shortage by eliminating heat generated from the body and by water conservation mechanisms so that the kidneys getting rid of unwanted substances in highly concentrated urine, there are limits. Sooner or later the unprotected desert traveller with insufficient water will die. Likewise, mechanisms to maintain the blood pressure, and so ensure continuing perfusion of tissues with blood bearing oxygen and nutriments, can withstand quite an impressive loss of blood but not a catastrophic haemorrhage. The upshot of all the processes we can plausibly gather under the heading of "ageing" British Association for the Advancement of Science September 2003 Raymond C Tallis 11 is progressive narrowing of the capacity to adapt to events that threaten homoeostasis: this narrowing (or "homoeostenosis") means that the size of the adverse event - a pathological process, trauma, exposure to extremes of temperature - necessary to result in irreversible changes leading to the death of the organism is much smaller than it would be in a younger person. Homoeostenosis, reduced adaptive capacity, is in essence what "frailty" is. It is clearly associated with an increased probability of death but death will come more easily: in extreme old age, relatively minor pathological events or external upsets may be fatal. The death of an extremely frail person is easier than that of a person with homoeostatic mechanisms intact. Frailty is not itself unpleasant: it is quite distinct from decrepitude; it is not associated with the symptoms characteristic of focal disease - such as nausea, pain or breathlessness (though, for example, exercise capacity will be significantly reduced) - because it is, as the definition just given emphasises, generalised. As Kirkwood has put it, "ageing is an harmonious decline in organ systems". It is focal, out-of-synch, declines that are associated with unpleasant symptoms. The out-of-synch declines are the (organic-specific) diseases which may be necessary to tip the person over into irreversible loss of homoeostenosis. The later in the course of ageing that the pathological process occurs, the less drastic the illness will have to be in order to exceed the "homoeostatic elastic limit" from which the individual can bounce back. This, then, is how ageing comes to the rescue: death occurs more easily from pathological processes; survival with very severe disease is ever less likely as the individual becomes biologically more aged. (This is particularly liable to be true British Association for the Advancement of Science September 2003 Raymond C Tallis 12 as many of the symptoms of illness - such as the malaise associated with viral infections or the pain associated with inflammation - are themselves the products of adaptive responses, which are blunted in the biologically aged.) As Grim ley Evans has put it: By delaying the onset of disabling diseases to ageing has raised later ages when intrinsic fatality by reducing adaptability, the average disability before death will be duration of shortened. In brief, we shall spend a longer time living and a shorter time dying. Thus is the seeming circle squared and the paradoxical decrease of disability before death is explained. There are data that bear rather directly on this theoretical framework. It has been observed that those who die in their late 60s have on average a longer period of dependency before death compared with those who died in their late 80’s. Patients who have a stroke later in old age have a much reduced six month survival compared with those who have their strokes early in old age. As Grimley Evans said, more years of living and fewer years of dying. The Future When we think about the possible futures of our life span, health span and our health in old age, it seems that there are three possible scenarios: the "Nightmare Scenario" ; the "Receding Horizon" scenario; and the "Approaching Asymptote" scenario: British Association for the Advancement of Science September 2003 Raymond C Tallis 13 The Possible Futures of Old Age MRI March 2003 43 Each curve in the diagram represents the average level of disability or chronic illness severity against age. The first graph represents the present; what (I hope) we shall come to look back on as "the bad old days", rather as I now look back on the early 1970s when I first became a doctor or, indeed, the early 1980's when I became a consultant. In this graph, we see that Mr and Mrs Unisex Average live a pretty healthy life, free of chronic illness or significant disability until, say their late sixties. Then problems start to pile up until, eventually, death supervenes at a unisex average of approximately 75 years of age. The period between the onset of significant illness and death is what we have in our sights; and the aim of medicine British Association for the Advancement of Science September 2003 Raymond C Tallis 14 as defined above is to reduce the shaded area of person years of medically unsatisfactory life. According to Nightmare Scenario, beloved of the media, serious illness begins at about the same time, but due to the unwise wonders of modern medicine, Mr and Mrs Unisex average are "kept alive" much longer. A longer life is bought at the cost of a longer death: medicine adds to the sum total of human woe. In accordance with this scenario, it would not be unusual to have a long Fourth Age of life entirely spent in an acute hospital and a significant portion of it on a ventilator! The third scenario - the "Receding Horizon" - is the outcome of two matched changes: the postponement of the onset of chronic ill health – and its progression to each level of severity - and the postponement of death. While there is a satisfying gain in life expectancy, the goal of "a health span that approximates to the life span" retreats as fast as the age of onset of chronic illness advances. The shaded area of medically unsatisfactory life remains unchanged. In the final scenario - "The Approaching Asymptote" - the onset of chronic illness is postponed much more than is death because at very late old age, death occurs easily. There are gains in life expectancy but greater gains in healthy active years of life: the period of chronic illness before death is shortened and the ideal of a long life in which the health span approximates the life span ever more closely - the shaded area progressively thins with medical advance - itself comes nearer. It will never be fully achieved because, as my father pointed out (at the age of 92), “you have to die of British Association for the Advancement of Science September 2003 Raymond C Tallis 15 something” and that means some illness before death. The evidence given earlier does not suggest that The Approaching Asymptote Scenario is impossible or even unlikely. The twin aims of medicine, that of postponing death and of minimising suffering due to illness, are not therefore in conflict. A health span that is all but co-terminous with life span is a goal that is both supremely worthwhile and achievable. In the meantime, we m ay all of us look forward to a better and better old age in which we do not place ever-increasing, unsustainable burdens on the NHS, our supporters and the Treasury. NOTE This paper is based upon the following articles: Raymond Tallis, ‘Going, going, gone'; - London Review of Books 1996; 18(7):26-7. Raymond Tallis, 'Finding the True Significance of the Demographic Revolution; Times Higher Education Supplement 9th July 1999. Raymond Tallis, 'Age Concern'; Telegraph Magazine; and on two chapters from Raymond Tallis: Hippocratic Oaths: Medicine, the NHS and their Discontents; Atlantic Press - forthcoming 2004. British Association for the Advancement of Science September 2003 Raymond C Tallis 16