Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
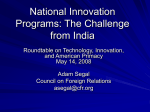
Fiscal aspects of health systems William Jack Georgetown University Motivated by “The fiscal sustainability of health care in Canada” Gregory Marchildon, Tom McIntosh, and Pierre-Gerlier Forest AUST CAN FR SWE UK US 2002 2001 2000 1999 1998 1997 1996 1995 1994 1993 1992 1991 1990 1985 1980 1970 1960 % of GDP Total health spending in Canada 16 14 12 10 8 6 4 2 0 Is spending sustainable? 1990-2002: ~constant, 9-10% of GDP But pressures lurk on the supply side: New technologies Prescription drugs …..and the demand side: Ageing How should additional costs be financed? Outline of comments Basic principles Mixed systems Some tax policy issues Basic principles Basic principles: I. Efficiency Raise money with minimal distortions Tax system design Maybe link taxes to benefits Spend money on the right things There is such a thing as too much health care Provide insurance …..without diluting incentives Basic principles: II. Equity Redistribute from rich to poor Use the income tax system Generally, don’t use differential commodity taxation, or the health system Redistribute from healthy to sick This is insurance Redistribute from low risks to high risks Risk adjustment mechanisms? Generating funds with mixed systems Public-private mixes Canada: separate by service type Public insurance for physician and hospital services Private (some public) insurance for drugs, dental, vision, long-term care An alternative: separate by service quality Public insurance for basic care (of all kinds) Private insurance for higher quality care Quality differentiated systems Chile: public-private Public health care: general tax finance ISAPREs: risk-based premiums Colombia: public-public Basic “subsidized regime”: general tax finance Higher quality “contributory regime”: payroll tax finance Dual public-private systems “Relieve the burden on the public system” Assumes taxes on those who opt out remain in place Allowing people to opt out with their taxes will not help budget position Paying them to opt out could reduce net revenues Compare with public-private education policies Should governments subsidize private schools? Insurance market competition Can competition help us “spend the money well”? Need to define the package – uniform or differentiated by risk? Adverse selection – the good risks drop out Affordability – package could be too expensive for bad risks and/or the poor Administrative/marketing costs Dual public-public systems Price discrimination Over-finance the higher quality public system Use extra funds to expand lower quality system Is this better than general taxation? efficiency, equity, political feasibility? Should the government get into other businesses to raise money for the poor? Tax policy User fees Raising money or spending it well? Is health care an efficient and/or equitable tax base? or are user fees “taxes on the sick”? “Distortionary” effects of user fees should in fact be positive The impact on risk exposure and equity might not be What is our model of demand? Do user fees deter only the use of “unnecessary” care? If not, then (a) some people who need care are making bad choices, and (b) some who don’t need care are being conned Suggests the need for supply-side costsharing Tax-subsidies to health insurance Effects of tax-subsidy – too much private insurance moral hazard? or too little support for public insurance? Is a tax-subsidy regressive? (a) Effective MTRs can be high on the nearpoor (b) Optimally designed tax system might include deductibility of health Tax treatment of out-of-pocket spending Medical savings accounts Use pre-tax income to pay OOP costs Can this reduce moral hazard problems? Nominal cost-sharing rate could increase Include insured expenses in taxable income Effect is to increase cost sharing But nominal cost-sharing rate could fall Is it efficient for different people to face different prices?