Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
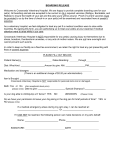
Name: Check In Date: Address: Check In Time: Account: Check Out Date: Phone: Check Out time: Patient: Cage Type: Age: Sex: Species: Tag: Breed: Weight: Color: Vaccination History -(Due Date) Microchip Canine Visitors: Feline Visitors: Rabies: Rabies: Dhpp: RCCP: Bordetella (Kennel Cough): FeLV: Other: Flea Treatment Applied? Yes No Date Applied: Sylvan Vet Food (Science Diet Maintenance) Feeding Instructions: Food to use: (Amount for each) Pet’s Own Food: Dry: Canned/Wet: Other: How Often? (Circle One) Once Daily - AM PM Twice Daily Three Times Daily Free Feed Treats? YES NO If yes, how often can pet be given a treat? Medications to be given: Bedding? Yes No Description/Color: Name of Prescription: Toys? Yes No Description/Color: Prescribed Dose: Leash/Collar? Yes No Description/Color: Frequency: Carrier? Yes No Description/Color: Bath? Yes No Description/Color: Special Instructions: Optional Additional: Nail Trim - $16.50 Express Anal Glands - $29.35 Fecal Testing - $29.35 Clean Ears - $34.75 Heartworm Test - $37.75 Clip/Comb-out - $46.50 Other (Estimate Provided For Authorization): Authorization for Boarding Admission: I, the undersigned owner or designated agent, hereby authorize Sylvan Veterinary Hospital, (Hereinafter ‘Hospital’) to board during the dates listed. I authorize the hospital to perform the services listed while is boarding. The Hospital will attempt to notify an owner if becomes ill while boarding. If the owner does not inform the Hospital regarding action to be taken, or if the state of health reasonably demands quick action in the opinion of the veterinarian, the Hospital will administer medical and/or surgical treatment as needed until the owner is notified. Charges for boarding are on a “per day” basis, not on a “per night” basis. Boarding charges will accrue beginning on the day of drop off. An additional day will be charged if the time of pickup exceeds 2:30pm on the scheduled pick up day. I understand that I am responsible for boarding with so the Hospital can use these accordingly and return any unused/remaining items. I understand that if I do not pick up my animal within 14 days of the scheduled pick up date, the Hospital will deem the animal as abandoned. If this occurs, the Hospital is authorized to remedy the abandonment as prescribed by law. I further understand that the abandonment DOES NOT release me of my financial obligation for services rendered, fees associated with abandonments, collection action, and/or legal services. If is not currently on flea prevention, I understand that if fleas are seen on my pet while boarding, flea treatment will be provided and I understand the fees incurred will be paid for at the time of discharge. Veterinary service is provided during night time hours as necessary in the judgment of the attending veterinarian. Continuous presence of a qualified personnel may not be provided. Emergency Contact Name: Signature Emergency Contact Number: Office Use Only: Patient Admission Initials: Patient Discharge Initials: